Best Peptides for Menopause Symptoms: 2026 Research Guide

Introduction#
Menopause marks a fundamental shift in female physiology. The decline in estrogen and progesterone production triggers a cascade of changes affecting virtually every organ system -- from bone density and cardiovascular function to neurological health, skin integrity, and metabolic regulation. While hormone replacement therapy (HRT) remains the standard of care for many menopausal symptoms, research into peptide-based approaches has expanded as scientists seek to address specific aspects of menopausal decline through targeted mechanisms.
This guide examines 11 peptides being studied for their relevance to menopause symptoms. These compounds address different aspects of the menopausal transition -- hormonal regulation, bone loss, skin aging, sleep disruption, sexual health, immune changes, and metabolic shifts. For a broader overview of peptides relevant to female health, see our Peptides for Women guide.
Important note: Most of these peptides are not FDA-approved for menopause indications. Only abaloparatide (for postmenopausal osteoporosis) and PT-141 (for hypoactive sexual desire disorder in premenopausal women) have FDA approvals for conditions related to this discussion. This article is for educational and research purposes only -- consult a qualified healthcare provider before considering any peptide therapy.
Understanding Menopause and Peptide Research#
The menopausal transition typically occurs between ages 45 and 55 and involves the progressive decline of ovarian function. Estrogen, the primary female sex hormone, plays roles far beyond reproduction -- it maintains bone density, supports cardiovascular health, regulates neurotransmitter systems, maintains skin collagen, and modulates immune function. When estrogen levels fall, these systems are all affected.
Peptide research in this area generally falls into two categories: peptides that may directly address hormonal signaling (such as kisspeptin), and peptides that target downstream consequences of estrogen decline (such as bone loss, skin aging, or metabolic changes). Neither category is intended to replace HRT, but they represent active areas of investigation.
Hormonal Regulation#
Kisspeptin#
Evidence Level: Clinical research | Research Status: Investigational
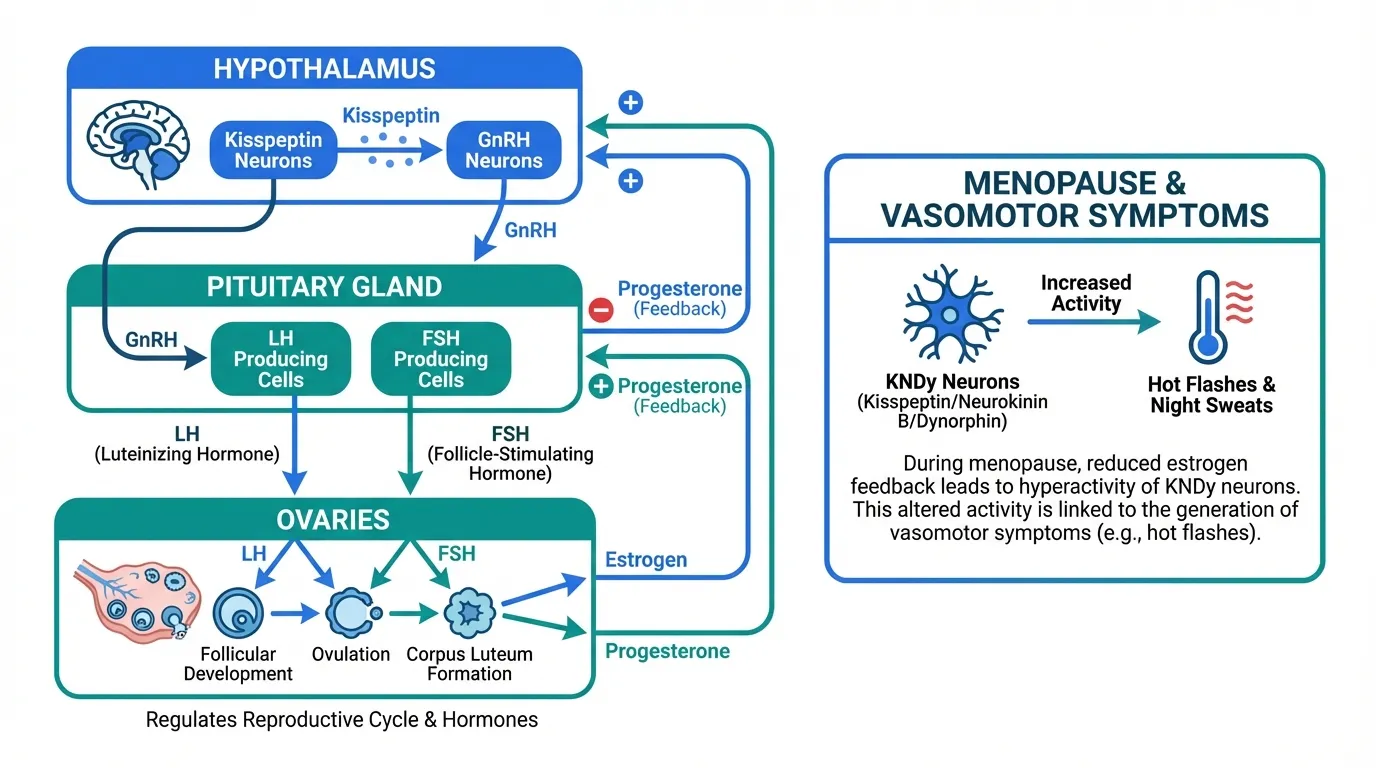
Kisspeptin is a hypothalamic neuropeptide that functions as the upstream regulator of the GnRH (gonadotropin-releasing hormone) pulse generator. It is a central player in the neuroendocrine control of reproduction, triggering the cascade that leads to LH and FSH release from the pituitary.
During the menopausal transition, kisspeptin neuron activity changes significantly. Research has shown that kisspeptin expression in the hypothalamic infundibular (arcuate) nucleus increases after menopause -- this hypertrophy of KNDy (kisspeptin/neurokinin B/dynorphin) neurons is thought to contribute to vasomotor symptoms (hot flashes). The neurokinin B component of these neurons is now a validated drug target, with NK3 receptor antagonists (such as fezolinetant, FDA-approved in 2023) demonstrating efficacy for hot flashes.
Kisspeptin research relevant to menopause includes:
- Vasomotor symptom pathophysiology -- understanding kisspeptin neuron changes has directly informed the development of non-hormonal treatments for hot flashes
- Reproductive health -- kisspeptin is being studied in IVF protocols as a potentially safer trigger for oocyte maturation, relevant to women in perimenopause seeking fertility
- Neuroendocrine aging -- kisspeptin's role in the hypothalamic changes of menopause is an active area of research
Limitations: Kisspeptin itself is not being developed as a menopause treatment. Its primary clinical application is in reproductive medicine. However, research on kisspeptin neuron biology has directly informed treatments for vasomotor symptoms. For more on kisspeptin's reproductive applications, see Peptides for Fertility.
Sexual Health#
PT-141 (Bremelanotide)#
Evidence Level: FDA-approved for HSDD | Research Status: Approved (Vyleesi)
PT-141 (bremelanotide) is a melanocortin-4 receptor agonist that acts centrally in the brain to modulate sexual desire. Unlike phosphodiesterase inhibitors that target peripheral blood flow, PT-141 works through the CNS to influence arousal pathways. It was FDA-approved in 2019 as Vyleesi for hypoactive sexual desire disorder (HSDD) in premenopausal women.
Sexual desire changes are reported by approximately 40-50% of women during the menopausal transition, driven by both hormonal changes (declining estrogen and testosterone) and neurotransmitter shifts. While PT-141 is currently approved only for premenopausal women, its central mechanism of action suggests potential relevance to postmenopausal sexual health.
Research Findings#
- The RECONNECT Phase 3 trials demonstrated statistically significant improvements in sexual desire and reduction in distress related to low sexual desire
- PT-141 works through a distinct mechanism from hormonal therapies, potentially complementing rather than replacing estrogen or testosterone approaches
- The subcutaneous injection is self-administered as needed, approximately 45 minutes before anticipated sexual activity
Limitations: FDA approval is specifically for premenopausal HSDD. Data in postmenopausal women is limited. Common side effects include nausea (40% of patients in trials), flushing, and headache. PT-141 is not recommended for use with cardiovascular disease. For a comprehensive profile, see PT-141.
Bone Density#
Abaloparatide#
Evidence Level: Phase 3 clinical trials | Research Status: FDA-approved (Tymlos)
Abaloparatide is a synthetic analog of parathyroid hormone-related peptide (PTHrP) and is one of only two peptide-based anabolic bone therapies FDA-approved for postmenopausal osteoporosis (alongside teriparatide). Osteoporosis is one of the most significant long-term consequences of menopause -- women can lose up to 20% of bone density in the 5-7 years following menopause.
Research Findings#
- The ACTIVE Phase 3 trial demonstrated that abaloparatide reduced the risk of new vertebral fractures by 86% compared to placebo over 18 months
- Abaloparatide also significantly reduced nonvertebral fractures and showed numerical superiority over teriparatide for hip bone mineral density gains
- The ACTIVExtend extension study showed that transitioning from abaloparatide to alendronate maintained and extended fracture protection
- Abaloparatide received expanded FDA approval in December 2022 for use in men with osteoporosis at high risk of fracture
Limitations: Treatment duration is limited to 18-24 months due to theoretical osteosarcoma risk (observed in rats at high doses). Must be followed by an antiresorptive agent to maintain bone gains. Daily subcutaneous injection required. Not recommended for patients with hypercalcemia, Paget's disease, or prior radiation therapy involving the skeleton. For a complete profile, see Abaloparatide and our guide to Peptides for Bone Health.
Skin Aging#
GHK-Cu#
Evidence Level: In vitro and limited clinical data | Research Status: Category 2 (injectable); topical available
GHK-Cu is a copper-binding tripeptide that has been studied extensively for its effects on skin biology. Estrogen decline during menopause is associated with accelerated skin aging -- collagen content decreases by approximately 2% per year post-menopause, and skin thickness, hydration, and elasticity all decline. GHK-Cu research addresses several of these pathways.
Research Findings#
- GHK-Cu has been shown to modulate the expression of over 4,000 human genes, many involved in collagen synthesis, elastin production, glycosaminoglycan synthesis, and antioxidant defense
- In vitro studies demonstrate increased production of collagen types I and III, decorin, and other extracellular matrix components
- Gene expression studies suggest GHK-Cu may stimulate fibroblast growth factors and support dermal remodeling pathways that decline with estrogen loss
- Topical formulations have shown improvements in skin firmness and fine line appearance in small studies
Limitations: Most data is in vitro or from small topical studies. Injectable GHK-Cu is FDA Category 2 (banned from compounding). The relationship between in vitro gene expression changes and clinical skin outcomes is not fully established. Industry funding of some studies warrants cautious interpretation. For more on skin peptides, see Peptides for Skin Health and Collagen Peptides for Skin Rejuvenation.
Gut Health and Inflammation#
BPC-157#
Evidence Level: Preclinical (animal studies) | Research Status: Category 2
BPC-157 is a synthetic pentadecapeptide derived from a sequence found in human gastric juice. While not studied specifically for menopause, its researched properties in gut health and inflammation modulation may be relevant to several menopausal complaints.
Gastrointestinal symptoms are common during the menopausal transition. Estrogen receptors are present throughout the GI tract, and declining estrogen levels can affect gut motility, barrier function, and the gut microbiome. Many women report increased bloating, changes in bowel habits, and GI discomfort during perimenopause.
Research Findings#
- Preclinical studies demonstrate BPC-157's protective effects on gut mucosa and its ability to accelerate healing of various GI lesions in animal models
- Research suggests BPC-157 may modulate inflammatory pathways including the nitric oxide system
- Animal studies have shown effects on the gut-brain axis, potentially relevant to the mood and cognitive changes associated with menopause
- BPC-157 has also been studied for musculoskeletal healing, which may be relevant given the increased injury susceptibility associated with declining estrogen
Limitations: No human clinical trials exist for BPC-157. All data is from animal models, primarily by a single research group. BPC-157 is FDA Category 2, meaning it is banned from compounding pharmacies. Its effects on female reproductive hormones and safety during the menopausal transition have not been studied. For a complete profile, see BPC-157.
Sleep Disruption#
Sleep problems affect 40-60% of women during the menopausal transition. Contributing factors include vasomotor symptoms (night sweats), declining progesterone (which has sedative properties), and changes in circadian regulation. Two peptides have been studied for sleep-related effects.
Ipamorelin#
Evidence Level: Phase 2 clinical data | Research Status: Investigational
Ipamorelin is a selective growth hormone secretagogue that stimulates GH release through the ghrelin receptor (GHS-R1a). Growth hormone secretion naturally peaks during deep sleep, and the age-related decline in GH is associated with reduced sleep quality -- a decline that accelerates during menopause.
- Ipamorelin stimulates pulsatile GH release that mimics physiological patterns, potentially supporting the GH surge that occurs during slow-wave sleep
- Unlike broader GH secretagogues, ipamorelin is selective for GH release without significantly affecting cortisol or prolactin -- hormones that can independently disrupt sleep
- The metabolic effects of improved GH pulsatility (body composition, energy metabolism) may address additional menopausal complaints
Limitations: No studies have specifically examined ipamorelin for menopausal sleep disruption. The sleep quality connection is inferred from GH physiology rather than direct clinical evidence. Ipamorelin is not FDA-approved. See Ipamorelin and our guide to Growth Hormone Peptides.
DSIP (Delta Sleep-Inducing Peptide)#
Evidence Level: Limited clinical data | Research Status: Investigational
DSIP is a nine-amino-acid neuropeptide first isolated from cerebral venous blood of rabbits during induced sleep. Its name reflects its original discovery context, though its actual mechanism is more complex than simply "inducing" delta sleep.
- Early clinical studies reported that DSIP administration improved sleep onset and increased the proportion of time spent in slow-wave (delta) sleep
- Research has suggested DSIP may modulate cortisol and ACTH rhythms, potentially relevant to the HPA axis changes that occur during menopause
- Some studies have explored DSIP's effects on stress response and pain perception, both of which may be altered during the menopausal transition
Limitations: DSIP research is dated and limited. Most studies were conducted in the 1980s-1990s with small sample sizes and methodological limitations. No modern clinical trials have been conducted. DSIP has a very short half-life in circulation. Its mechanism of action is not fully characterized. For a complete profile, see DSIP and our Peptides for Sleep guide.
Body Composition and Metabolic Health#
Menopause is associated with significant metabolic shifts -- increased visceral fat accumulation, reduced lean muscle mass, and declining insulin sensitivity. These changes increase cardiovascular risk and contribute to the body composition changes that many women find distressing.
CJC-1295#
Evidence Level: Phase 2 clinical data | Research Status: Investigational
CJC-1295 is a synthetic analog of growth hormone-releasing hormone (GHRH) that stimulates GH secretion from the pituitary. The age-related decline in GH -- termed somatopause -- overlaps temporally with menopause and may compound its metabolic effects.
- Clinical studies have demonstrated that CJC-1295 can significantly increase IGF-1 levels and restore more youthful GH secretion patterns
- Improved GH signaling may help counteract the shift toward visceral fat accumulation and lean mass loss that occurs during menopause
- CJC-1295 is often studied in combination with ipamorelin (the "CJC/Ipamorelin stack"), as the two peptides work through complementary mechanisms
Limitations: No studies have specifically examined CJC-1295 in menopausal or postmenopausal women. The relationship between improved GH parameters and clinical outcomes in this population is not established. CJC-1295 is not FDA-approved. For more detail, see our CJC-1295 + Ipamorelin Stack guide.
MOTS-c#
Evidence Level: Preclinical with translational data | Research Status: Investigational
MOTS-c is a mitochondrial-derived peptide (MDP) encoded in mitochondrial DNA. It functions as a metabolic regulator and has been described as an "exercise mimetic" based on its ability to activate AMPK and improve glucose utilization. Endogenous MOTS-c levels decline with age, a decline that may be accelerated by the metabolic shifts of menopause.
- MOTS-c has been shown to improve insulin sensitivity and glucose metabolism in animal models, relevant to the declining insulin sensitivity of menopause
- As an exercise mimetic, MOTS-c may help counteract the reduced physical capacity and metabolic rate that accompany menopause
- Research suggests MOTS-c levels correlate with physical fitness and metabolic health, both of which decline during the menopausal transition
Limitations: All data is preclinical. No human clinical trials have been completed. The relationship between endogenous MOTS-c decline and menopausal metabolic changes is correlational, not causal. For more on mitochondrial peptides, see Mitochondrial Peptides and Longevity.
Aging and Cellular Health#
Epitalon#
Evidence Level: Preclinical | Research Status: Category 2
Epitalon (epithalon, Ala-Glu-Asp-Gly) is a synthetic tetrapeptide studied for its effects on telomerase activation and pineal gland function. Menopause accelerates several biological aging processes, and epitalon's researched mechanisms intersect with some of these pathways.
- In vitro studies have reported that epitalon activates telomerase in human somatic cells, potentially counteracting the telomere shortening that accelerates with estrogen decline
- Research has explored epitalon's effects on melatonin synthesis through pineal gland modulation -- melatonin production declines with age and may further decrease during menopause, contributing to sleep and circadian disruption
- Animal studies have shown lifespan extension (12-13% in SHR mice) and improvements in markers associated with aging
Limitations: Research is dominated by a single group (Khavinson Institute). No clinical trials in humans, and no studies specifically in menopausal populations. Epitalon is FDA Category 2. Independent replication of key findings is limited. For a complete profile, see Epitalon and our Anti-Aging Peptides guide.
Immune Modulation#
Thymosin Alpha-1#
Evidence Level: Clinical data for immune applications | Research Status: Approved outside the US (Zadaxin)
Thymosin Alpha-1 (Ta1) is a 28-amino-acid peptide originally isolated from thymic tissue. It plays a role in T-cell maturation and immune regulation. The relevance to menopause lies in the intersection of immunosenescence (age-related immune decline) and the immunomodulatory effects of estrogen withdrawal.
Estrogen has well-documented effects on immune function -- it enhances humoral immunity, modulates T-cell responses, and influences cytokine production. The decline in estrogen during menopause contributes to immune dysregulation, increased susceptibility to infections, and altered autoimmune risk profiles.
Research Findings#
- Thymosin Alpha-1 has been shown to enhance T-cell function, increase natural killer cell activity, and modulate dendritic cell maturation
- It is approved in over 35 countries (as Zadaxin) for hepatitis B and C, and as an immune adjuvant
- Research suggests Ta1 may help counteract thymic involution -- the shrinking of the thymus gland that accelerates with aging and may be compounded by estrogen decline
- Its anti-inflammatory properties may be relevant to the low-grade chronic inflammation that characterizes both aging and the post-menopausal state
Limitations: No studies have specifically examined thymosin alpha-1 in the context of menopausal immune changes. The connection between Ta1 and menopause-related immune decline is theoretical. Ta1 is not FDA-approved in the United States. See Thymosin Alpha-1 and our Immune-Modulating Peptides guide.
Safety Considerations#
Peptide research for menopause symptoms comes with important caveats:
Regulatory status: Of the peptides discussed, only abaloparatide and PT-141 have FDA approvals for indications related to this article. Several others (BPC-157, GHK-Cu injectable, epitalon) are FDA Category 2, meaning they are banned from compounding pharmacies.
Interaction with HRT: The safety of combining research peptides with hormone replacement therapy has not been studied. Women on HRT should discuss any additional therapies with their healthcare provider.
Reproductive considerations: Women in perimenopause may still be fertile. The effects of most research peptides on fertility, pregnancy, and lactation have not been studied. Appropriate contraception should be maintained as applicable.
Cancer risk: Some peptides that promote cell growth (growth hormone secretagogues, anabolic peptides) require careful consideration in populations with elevated cancer risk. Estrogen-receptor-positive breast cancer history is a particular concern, as some of these pathways may theoretically interact with estrogen-sensitive tissues.
Limited female-specific data: Many peptide studies have been conducted primarily in male animal models or mixed-sex human populations without adequate sex-stratified analysis. The pharmacokinetics, efficacy, and safety profile of peptides may differ between sexes.
Research Limitations and Future Directions#
The field of peptide research for menopause symptoms is still early-stage for most compounds discussed here. Key limitations include:
- Lack of menopause-specific trials -- most evidence is extrapolated from general peptide research or from studies in non-menopausal populations
- Preclinical bias -- several peptides (BPC-157, MOTS-c, epitalon) have predominantly animal data with limited or no human clinical evidence
- Single-group research -- some compounds have research concentrated within a single institution, limiting independent validation
- Short study durations -- menopause is a decades-long state, but most peptide studies span weeks to months
Future directions in this field may include:
- Targeted clinical trials in perimenopausal and postmenopausal populations
- Combination approaches studying peptides alongside HRT or other established therapies
- Biomarker-guided treatment using peptide-specific biomarkers to personalize therapy
- Sex-stratified analysis of existing clinical trial data to better understand female-specific responses
Consult Your Healthcare Provider#
Menopause management should be guided by a qualified healthcare provider who understands your individual health history, risk factors, and symptom profile. The peptides discussed in this guide represent areas of active research interest, not established menopause treatments.
Hormone replacement therapy, lifestyle modifications (exercise, nutrition, sleep hygiene), and FDA-approved non-hormonal treatments (such as fezolinetant for hot flashes) remain the evidence-based foundation for menopause symptom management. Any consideration of peptide-based approaches should occur in consultation with a healthcare provider and should complement -- not replace -- established treatments.
For more on peptide safety, see our Peptide Safety Guide and Peptide Drug Interactions Guide.

{kind=link}
Frequently Asked Questions About Best Peptides for Menopause Symptoms: 2026 Research Guide
What does this article cover?
A research-based overview of peptides being studied for menopause-related symptoms including hormonal regulation, bone density loss, skin aging, sleep disruption, sexual health, and metabolic changes. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Kisspeptin, PT-141 (Bremelanotide), GHK-Cu, BPC-157, Epitalon, CJC-1295, Ipamorelin, Thymosin Alpha-1, Abaloparatide, DSIP, and MOTS-c. Each is examined for its potential relevance to specific menopause symptoms based on available research.
Are any of these peptides FDA-approved for menopause?
Abaloparatide (Tymlos) is FDA-approved for postmenopausal osteoporosis. PT-141 (Vyleesi) is FDA-approved for hypoactive sexual desire disorder in premenopausal women. The other peptides discussed are investigational or used off-label, and none are specifically approved for menopause symptoms.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of peptides relevant to menopause. It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.

How to Choose Your First Peptide: A Decision Framework by Goal
A comprehensive decision framework to help beginners identify the right peptide for their goals. Maps 10 health categories to specific peptide recommendations with evidence levels, administration routes, and regulatory context.
Best Peptides to Stack with Retatrutide (2026 Research Guide)
A 2026 research-focused review of the peptides most often discussed alongside retatrutide for GI side effects, lean-mass preservation, hair and skin changes, sleep, and adjunct fat loss — what the literature does and does not support.
You Might Also Like
Related content you may find interesting