Immune-Modulating Peptides: Thymosin Alpha-1, KPV, LL-37, and Beyond

Introduction#
The immune system operates through a complex network of cells, signaling molecules, and feedback mechanisms that must balance two opposing demands: mounting effective responses against pathogens and preventing self-directed damage that leads to autoimmune disease. Peptides represent an emerging class of immune modulators that may influence this balance through more targeted mechanisms than conventional immunosuppressants or immunostimulants.
This research review examines six peptides with documented immunomodulatory properties. These range from thymosin alpha-1, which has regulatory approval in over 35 countries, to VIP, whose autoimmune applications remain preclinical. For each compound, we evaluate the mechanism of immune modulation, quality of clinical evidence, and implications for both immune enhancement and immune-mediated disease.
Important note: No peptide in this review is FDA-approved for immune modulation, autoimmune disease, or immune enhancement in the United States. Immune conditions require professional medical management. This article is for healthcare professionals and researchers seeking evidence-based summaries.
For a broader overview, see Top Immune-Boosting Peptides. For inflammation-specific applications, see Peptides for Inflammation.
The Peptide-Immune Axis: Framework for Understanding#
Immune-modulating peptides can be categorized by their primary mechanism of action within the immune system:
Immunomodulators vs. Immunostimulants vs. Immunosuppressants#
- Immunomodulators (thymosin alpha-1, KPV) -- rebalance immune function by enhancing underactive pathways or dampening overactive ones without broadly suppressing immunity
- Antimicrobial peptides (LL-37) -- directly kill pathogens while also recruiting and modulating immune cells
- Anti-inflammatory peptides (KPV, VIP) -- specifically target inflammatory signaling pathways (NF-kB, cytokine networks) without broadly suppressing immune function
- Thymic peptides (thymosin alpha-1, thymalin) -- support T cell maturation and differentiation, addressing the immune decline associated with thymic involution
- Antioxidant support (glutathione) -- maintain the redox balance required for optimal immune cell function
This categorization is simplified; most immune peptides have overlapping mechanisms. Thymosin alpha-1, for example, has immunostimulatory, immunomodulatory, and anti-inflammatory properties depending on the immunological context.
Thymosin Alpha-1: Clinical Evidence from Hepatitis to Cancer#
Evidence Level: Phase 2/3 RCTs; approved in 35+ countries | FDA Status: Not FDA-approved; orphan drug designation
Thymosin Alpha-1 (Ta1) is a 28-amino-acid peptide originally isolated from thymic tissue (thymosin fraction 5) by Allan Goldstein at George Washington University in the 1970s. The synthetic version, marketed as Zadaxin, represents the most clinically validated immune peptide available.
Mechanism of Immune Modulation#
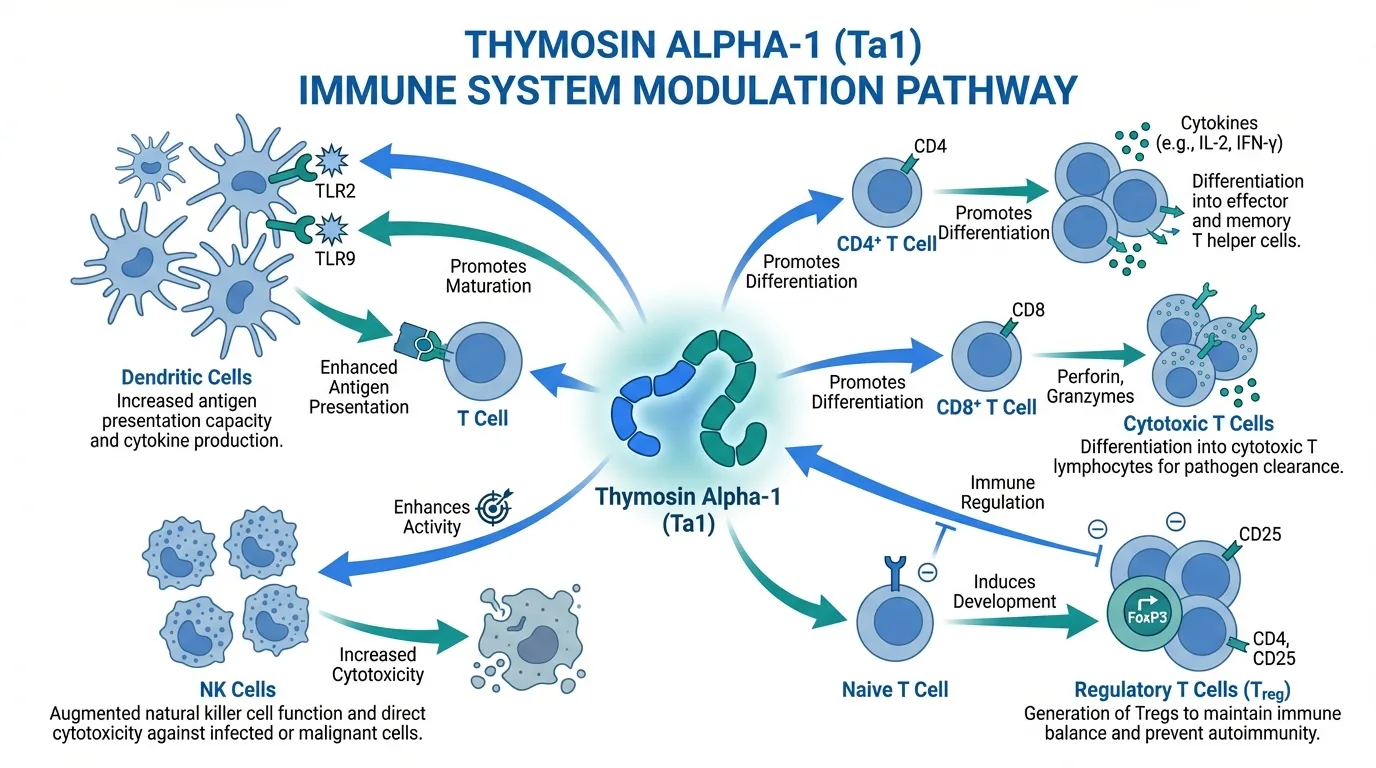
Thymosin alpha-1 modulates the immune system through multiple pathways:
- Dendritic cell maturation -- Ta1 promotes the maturation of dendritic cells, enhancing antigen presentation to T cells
- T cell differentiation -- promotes differentiation of CD4+ and CD8+ T cells, supporting both helper and cytotoxic immune responses
- Th1/Th2 balance -- shifts the T helper balance toward Th1 responses (cellular immunity) when Th2 dominance impairs pathogen clearance
- Regulatory T cell induction -- promotes regulatory T cell (Treg) development, which is critical for preventing autoimmune overactivation
- TLR signaling -- activates toll-like receptor pathways (TLR2, TLR9) in dendritic cells, bridging innate and adaptive immunity
- NK cell activation -- enhances natural killer cell activity, important for antiviral and antitumor surveillance
This multi-pathway mechanism explains why Ta1 can simultaneously enhance immune responses against pathogens (useful in hepatitis, cancer) and potentially modulate autoimmune overactivation (through Treg induction).
Clinical Evidence#
Hepatitis B. The strongest clinical evidence for Ta1 comes from chronic hepatitis B treatment. Multiple RCTs have demonstrated that Ta1 (1.6 mg subcutaneously twice weekly for 6 months) produces sustained virological responses with HBeAg seroconversion rates of approximately 25-40%, comparable to interferon-alpha monotherapy but with substantially fewer side effects. Combination therapy (Ta1 + interferon-alpha) has shown higher response rates than either agent alone in several studies.
Hepatitis C. Studies evaluating Ta1 combined with interferon-alpha and ribavirin for hepatitis C showed enhanced sustained virological response rates in some subgroups, particularly in patients who were interferon non-responders.
Cancer immunotherapy adjuvant. Ta1 has been studied as an adjuvant to chemotherapy and other cancer treatments in hepatocellular carcinoma, melanoma, and non-small cell lung cancer. A meta-analysis of cancer studies reported improved overall survival and enhanced immune parameters (CD4/CD8 ratios, NK cell activity) when Ta1 was added to standard treatment. While individual study quality varied, the consistent direction of benefit across multiple cancer types supports an immunomodulatory effect.
Immune deficiency. Ta1 has been evaluated in immunocompromised populations, including elderly patients with impaired vaccine responses, patients undergoing bone marrow transplantation, and individuals with primary immunodeficiency. Studies generally report improved immune parameters (T cell counts, vaccine response rates) with Ta1 treatment.
Limitations#
Despite broad international approval, Ta1 has not received FDA approval in the United States. The FDA's assessment has focused on the heterogeneity of trial designs and the need for larger, more definitive confirmatory trials for specific indications. Additionally, the optimal dosing, treatment duration, and patient selection criteria remain subjects of ongoing research.
For comparison with LL-37, see LL-37 vs Thymosin Alpha-1. For comparison with thymalin, see Thymalin vs Thymosin Alpha-1.
KPV: Anti-Inflammatory Peptide Without Immunosuppression#
Evidence Level: Preclinical only; no completed human trials | FDA Status: Not FDA-approved; not FDA-evaluated
KPV is a C-terminal tripeptide (Lys-Pro-Val) fragment of alpha-melanocyte-stimulating hormone (alpha-MSH). It retains the anti-inflammatory properties of the parent molecule without its melanocortin receptor-dependent effects on pigmentation or energy balance.
Mechanism of Action#
KPV's anti-inflammatory mechanism centers on NF-kB inhibition:
- NF-kB pathway suppression -- KPV enters cells and directly inhibits NF-kB nuclear translocation, reducing transcription of pro-inflammatory genes. Notably, this occurs independently of melanocortin receptors, distinguishing KPV from full-length alpha-MSH
- Cytokine modulation -- reduces production of pro-inflammatory cytokines including IL-1beta, IL-6, and TNF-alpha in inflammatory models
- Mucosal anti-inflammation -- studies in colitis models show that KPV reduces mucosal inflammation when administered both systemically and orally, suggesting it may be active in the gastrointestinal tract
- Non-immunosuppressive -- unlike corticosteroids or TNF-alpha inhibitors, KPV does not appear to broadly suppress immune function, potentially preserving antimicrobial defense while reducing pathological inflammation
Preclinical Evidence#
Colitis models. Oral KPV administration reduced colonic inflammation in mouse models of both acute and chronic colitis. The peptide decreased pro-inflammatory cytokine levels, reduced tissue damage scores, and improved clinical colitis indices. Notably, the oral route of administration, unusual for a peptide, suggests stability in the GI tract or local action on mucosal immune cells.
Skin inflammation. KPV has shown anti-inflammatory effects in models of contact dermatitis and skin sensitization, reducing edema and immune cell infiltration.
Wound healing. Some studies suggest that KPV's anti-inflammatory properties support wound healing by modulating the inflammatory phase without preventing the immune response necessary for debris clearance.
Limitations#
All KPV evidence is preclinical. No human clinical trials for inflammatory or autoimmune conditions have been completed. The oral bioavailability, pharmacokinetics, and dose-response relationship in humans are unknown. While the NF-kB inhibition mechanism is well-characterized in cell and animal studies, the clinical relevance of these findings requires human validation.
For comparison with LL-37, see KPV vs LL-37.
LL-37: The Human Antimicrobial Peptide#
Evidence Level: Extensive basic science; limited clinical application data | FDA Status: Not FDA-approved as a therapeutic
LL-37 is the only cathelicidin antimicrobial peptide found in humans. It is a 37-amino-acid peptide produced by neutrophils, macrophages, and epithelial cells as a first-line defense against pathogens. Unlike the other peptides in this review, LL-37 is not a synthetic therapeutic compound but rather an endogenous immune effector now being explored as a potential therapeutic agent.
Dual Antimicrobial and Immunomodulatory Functions#
Direct antimicrobial activity. LL-37 kills bacteria, fungi, and enveloped viruses through membrane disruption. Its cationic, amphipathic structure allows it to insert into negatively charged microbial membranes, forming pores that lead to cell death. This mechanism of action provides broad-spectrum activity and may be less susceptible to bacterial resistance development compared to conventional antibiotics, because resistance would require fundamental changes to membrane structure.
Immunomodulatory functions. Beyond direct pathogen killing, LL-37 modulates the immune response through:
- Chemotaxis -- recruits neutrophils, monocytes, and T cells to sites of infection
- Dendritic cell activation -- promotes dendritic cell differentiation and antigen presentation
- Inflammatory modulation -- while pro-inflammatory at infection sites, LL-37 can also neutralize lipopolysaccharide (LPS), reducing sepsis-associated inflammation
- Wound healing promotion -- stimulates keratinocyte migration and proliferation, promoting epithelial repair
- Biofilm disruption -- can penetrate and disrupt bacterial biofilms, a significant advantage over many conventional antibiotics
Research Applications#
Infections. LL-37 has been studied for topical and systemic infections, including burn wound infections, diabetic ulcers, and chronic wound infections. Its combination of antimicrobial and wound healing properties makes it particularly relevant for infected wound applications.
Inflammatory conditions. LL-37 deficiency has been associated with increased susceptibility to infections, while LL-37 overexpression has been implicated in some inflammatory conditions (rosacea, psoriasis). This dual role illustrates the complexity of immune modulation -- the same peptide can be beneficial or detrimental depending on context.
Cancer. Some studies suggest LL-37 has immunomodulatory effects relevant to cancer immunity, including enhancement of antitumor immune responses. However, LL-37 has also been reported to promote tumor growth in certain cancer types through its angiogenic properties, highlighting the need for context-specific evaluation.
Limitations#
LL-37 as a therapeutic faces challenges: it can be degraded by proteases in vivo, its production at scale is expensive, and its effects are context-dependent (pro-inflammatory in some settings, anti-inflammatory in others). Clinical development has focused on topical applications where local concentrations can be controlled.
For comparison with antimicrobial approaches, see Antimicrobial Peptides: LL-37, KPV Research.
Thymalin: Thymic Restoration and the Russian Clinical Tradition#
Evidence Level: Russian clinical studies; limited Western validation | FDA Status: Not FDA-approved; not FDA-evaluated
Thymalin is a peptide extract derived from bovine thymus gland tissue, developed by Khavinson and Morozov in the 1970s as part of the Russian bioregulator peptide program. It is proposed to restore thymic function in aging individuals, addressing the immune decline (immunosenescence) that accompanies thymic involution.
Mechanism of Action#
- Thymic function restoration -- thymalin is proposed to stimulate the remaining thymic epithelial tissue, promoting T cell maturation even in the context of age-related thymic involution
- T cell repertoire diversification -- by supporting thymic output, thymalin may help maintain T cell receptor diversity, which declines with age and impairs the ability to respond to novel pathogens
- Cytokine regulation -- studies report normalization of cytokine profiles in elderly subjects, shifting from the pro-inflammatory state ("inflammaging") toward a more balanced immune profile
- Bioregulator framework -- within the Khavinson model, thymalin is theorized to interact with thymic cell DNA to regulate gene expression involved in T cell production
Clinical Evidence#
Russian clinical studies spanning several decades report:
- Elderly immune restoration -- studies in elderly populations reported improvements in T cell counts, CD4/CD8 ratios, and immune functional assays following thymalin administration
- Longevity observations -- the Khavinson group published observational data suggesting that elderly individuals treated with thymalin and epitalon (pineal bioregulator) had reduced mortality over multi-year follow-up periods compared to untreated controls
- Infection susceptibility -- some studies reported reduced rates of respiratory and other infections in elderly subjects receiving thymalin
Limitations#
Thymalin research is concentrated in Russian-language literature from the Khavinson group, with minimal independent Western replication. Study designs often lack the rigor of modern RCTs (inadequate blinding, small sample sizes, observational endpoints). As a tissue extract rather than a defined peptide, batch-to-batch variability is a concern. The mechanism by which crude thymic peptide extracts specifically restore thymic function has not been convincingly demonstrated through Western pharmacological standards.
For a detailed comparison, see Thymalin vs Thymosin Alpha-1.
VIP: Vasoactive Intestinal Peptide in Autoimmunity#
Evidence Level: Extensive preclinical; early-stage clinical exploration | FDA Status: Not FDA-approved for immune conditions
VIP (vasoactive intestinal peptide) is a 28-amino-acid neuropeptide that acts as a potent anti-inflammatory and immunoregulatory molecule. Originally discovered in the gut, VIP is now recognized as a broadly expressed neuropeptide with significant immune functions.
Mechanism of Immune Modulation#
VIP's immunomodulatory effects are mediated through VPAC1 and VPAC2 receptors expressed on immune cells:
- Th1/Th2 balance -- VIP shifts T helper cell differentiation away from pro-inflammatory Th1 and Th17 responses toward Th2 and regulatory T cell (Treg) phenotypes
- Regulatory T cell induction -- VIP promotes Treg development and function, a critical mechanism for preventing autoimmune tissue damage
- Macrophage modulation -- VIP inhibits macrophage production of TNF-alpha, IL-6, and IL-12 while promoting anti-inflammatory IL-10 production
- Dendritic cell tolerogenesis -- VIP promotes tolerogenic dendritic cells that induce immune tolerance rather than immune activation
- NF-kB suppression -- like KPV, VIP inhibits NF-kB signaling, reducing transcription of pro-inflammatory genes
Autoimmune Research#
Preclinical studies have demonstrated VIP's efficacy in multiple autoimmune disease models:
- Rheumatoid arthritis -- VIP reduced joint inflammation, cartilage destruction, and bone erosion in collagen-induced arthritis models in mice
- Multiple sclerosis -- VIP treatment improved outcomes in experimental autoimmune encephalomyelitis (EAE), the standard animal model for MS
- Inflammatory bowel disease -- VIP reduced mucosal inflammation in colitis models, with effects on both immune cell infiltration and cytokine profiles
- Type 1 diabetes -- VIP delayed or prevented disease onset in NOD mouse models of autoimmune diabetes
Limitations#
Despite compelling preclinical data, VIP faces significant therapeutic challenges. It has a very short half-life (approximately 1-2 minutes in plasma), requiring either continuous infusion or modified delivery strategies. VIP's broad receptor distribution means it also affects blood pressure, heart rate, and gastrointestinal motility, creating potential for side effects. Clinical translation has been slow, with early-phase human studies in sarcoidosis and pulmonary hypertension but no completed RCTs in autoimmune conditions.
Glutathione: The Antioxidant Foundation for Immune Function#
Evidence Level: Extensive basic science; moderate clinical data for immune support | FDA Status: Available as supplement; not approved for immune conditions
Glutathione (GSH) is a tripeptide (gamma-glutamylcysteinylglycine) synthesized endogenously in every cell. While not traditionally classified alongside the other immune peptides in this review, glutathione plays a foundational role in immune cell function that warrants inclusion.
Role in Immune Function#
- Lymphocyte proliferation -- T cell activation and proliferation require adequate intracellular glutathione levels. GSH-depleted lymphocytes show impaired proliferative responses to antigens
- NK cell activity -- natural killer cell cytotoxicity is dependent on glutathione status. Supplementation in GSH-depleted individuals has been shown to restore NK cell function
- Oxidative burst regulation -- neutrophils and macrophages use reactive oxygen species (oxidative burst) to kill engulfed pathogens. Glutathione is essential for protecting the immune cells themselves from oxidative damage during this process
- Cytokine production -- GSH levels influence the balance between Th1 and Th2 cytokine production, with depletion favoring Th2 responses and repletion supporting Th1 cellular immunity
Clinical Relevance#
Glutathione depletion is associated with immune dysfunction in multiple contexts:
- Aging -- GSH levels decline with age, paralleling the decline in immune function (immunosenescence)
- HIV/AIDS -- severely depleted glutathione levels correlate with disease progression and impaired T cell function
- Chronic illness -- many chronic conditions are associated with oxidative stress and GSH depletion
- Supplementation studies -- oral liposomal glutathione and N-acetylcysteine (NAC, a GSH precursor) have been shown to improve immune parameters in elderly subjects and in HIV-positive individuals
Limitations#
Oral glutathione bioavailability remains debated. The tripeptide is hydrolyzed by intestinal enzymes, and how much intact GSH reaches systemic circulation varies by formulation. Liposomal and sublingual formulations may improve bioavailability compared to standard oral capsules, but standardized dosing guidelines are lacking. NAC as a precursor may be more reliable for raising intracellular GSH levels.
Clinical Evidence Comparison Table#
| Peptide | Highest Evidence Level | Key Indications Studied | Immune Mechanism | Administration |
|---|---|---|---|---|
| Thymosin Alpha-1 | Phase 3 RCTs | Hepatitis B/C, cancer adjuvant | T cell maturation, DC activation, Treg induction | SC injection |
| KPV | Preclinical | Colitis, skin inflammation | NF-kB inhibition, cytokine modulation | Oral (animal), SC |
| LL-37 | Early clinical | Wound infections, biofilm | Antimicrobial, chemotaxis, wound healing | Topical, SC |
| Thymalin | Russian clinical | Immunosenescence, infection prevention | Thymic restoration, T cell support | IM injection |
| VIP | Early clinical | Autoimmune models, sarcoidosis | Treg induction, Th1/Th2 shift | IV infusion, SC |
| Glutathione | Supplementation trials | Immune support, oxidative stress | Antioxidant, lymphocyte function | Oral, IV, liposomal |
Implications for Autoimmune Conditions#
The potential application of immune-modulating peptides in autoimmune disease is one of the most promising but least clinically validated areas of peptide research.
Theoretical Framework#
Autoimmune diseases result from a failure of immune tolerance -- the immune system attacks self-tissues. Peptides that promote regulatory T cell development (thymosin alpha-1, VIP) or reduce NF-kB-mediated inflammation (KPV, VIP) could theoretically address this dysfunction at a mechanistic level. Unlike broad immunosuppressants (corticosteroids, methotrexate, biologics), these peptides may rebalance immune function without increasing infection risk.
Evidence Status#
This theoretical promise remains largely unvalidated in human autoimmune patients. VIP has the strongest preclinical autoimmune data but faces pharmacokinetic challenges. KPV's oral bioavailability and GI-specific anti-inflammatory effects make it theoretically attractive for IBD but human data is absent. Thymosin alpha-1's Treg-promoting properties could be relevant to autoimmunity, but its clinical development has focused on immune enhancement (hepatitis, cancer) rather than immune modulation in autoimmune contexts.
Critical Cautions#
Immune modulation in autoimmune disease is inherently complex. Enhancing some immune pathways while suppressing others carries the risk of unpredictable outcomes. Patients with autoimmune conditions should not self-administer immune peptides without medical supervision, as even "immune-balancing" compounds could theoretically worsen disease through unintended pathway activation.
Key Takeaways#
-
Thymosin alpha-1 is the most clinically validated immune peptide, with regulatory approval in 35+ countries for hepatitis B and supporting data in cancer immunotherapy. Its multi-pathway mechanism (T cell maturation, Treg induction, DC activation) makes it the benchmark for immune peptide therapy.
-
KPV offers a unique anti-inflammatory mechanism through NF-kB inhibition without broad immunosuppression, with promising preclinical colitis data. All evidence remains preclinical.
-
LL-37 bridges antimicrobial and immunomodulatory functions as the body's endogenous defense peptide. Therapeutic development faces challenges with stability and context-dependent effects.
-
Thymalin represents the Russian bioregulator approach to immune aging, with decades of clinical observations but limited Western validation.
-
VIP has the strongest preclinical autoimmune data but faces pharmacokinetic challenges (very short half-life) that have slowed clinical translation.
-
Glutathione provides the antioxidant foundation for immune cell function, with the most accessible supplementation pathway but debated oral bioavailability.
-
No immune peptide is FDA-approved in the United States, and autoimmune applications remain largely preclinical despite strong theoretical rationale.
This article is for educational and informational purposes only. It does not constitute medical advice. Immune conditions require professional medical management. Always consult a qualified healthcare provider before considering any peptide therapy.
Related Reading#

{kind=link}
Frequently Asked Questions About Immune-Modulating Peptides: Thymosin Alpha-1, KPV, LL-37, and Beyond
What is the most clinically proven immune peptide?
Thymosin alpha-1 (Zadaxin) has the most extensive clinical evidence among immune peptides. It is approved in over 35 countries for hepatitis B treatment and has been studied as an immunotherapy adjuvant in cancer, with published Phase 2 and Phase 3 trial data. It is not FDA-approved in the United States.
How do immune-modulating peptides differ from immunosuppressants?
Traditional immunosuppressants broadly dampen immune function, which controls autoimmune activity but increases infection risk. Immune- modulating peptides like thymosin alpha-1 and KPV aim to rebalance immune function rather than suppress it. For example, thymosin alpha-1 enhances both Th1 and regulatory T cell activity, while KPV inhibits the NF-kB inflammatory pathway without suppressing antimicrobial immune responses. This distinction is important but largely theoretical for most peptides, as rigorous head-to-head comparisons with immunosuppressants are lacking.
Can KPV help with inflammatory bowel disease?
KPV has shown anti-inflammatory effects in preclinical models of colitis, including oral administration studies in mice that demonstrated reduced mucosal inflammation. However, no human clinical trials for IBD or any inflammatory condition have been completed. The preclinical results are promising but cannot be extrapolated to clinical efficacy in humans.
Is LL-37 an antibiotic?
LL-37 is an endogenous antimicrobial peptide produced by the human immune system, not a conventional antibiotic. It kills pathogens through direct membrane disruption and also modulates the immune response by recruiting immune cells and promoting wound healing. Unlike conventional antibiotics, bacteria appear less likely to develop resistance to LL-37 due to its membrane-targeting mechanism, though this resistance potential requires further study.
Are immune peptides safe for people with autoimmune conditions?
This is a critical question without a simple answer. Immune-modulating peptides that enhance immune function (like thymosin alpha-1) could theoretically worsen autoimmune conditions by stimulating the immune system. Conversely, peptides that promote regulatory T cells or anti-inflammatory pathways (KPV, VIP) might be beneficial. No immune peptide has been approved for autoimmune conditions, and individuals with autoimmune diseases should discuss any peptide use with their treating physician.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Can Peptides Help with Inflammation? A Research-Based Guide
Anti-inflammatory peptides — KPV, BPC-157, LL-37, thymosin alpha-1, VIP, and glutathione — with mechanisms and clinical evidence.

Top Immune-Boosting Peptides: Research Overview
Top immune-boosting peptides including Thymosin Alpha-1, Thymalin, LL-37, KPV, and Glutathione — evidence levels and mechanisms reviewed.

Antimicrobial Peptides: LL-37 and KPV in Infection and Inflammation Research
LL-37 and KPV antimicrobial peptide research reviewed — mechanisms of action, infection defense, gut immunity, and anti-inflammatory pathways.
You Might Also Like
Related content you may find interesting