Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?

Introduction#
If you have been researching ways to optimize growth hormone (GH) levels, you have likely encountered a growing list of peptide names -- ipamorelin, sermorelin, CJC-1295, GHRP-2, and others. The terminology can be overwhelming, especially when different sources use varying naming conventions and acronyms.
This guide is designed to cut through the complexity. It explains what growth hormone secretagogues are, how they differ from exogenous GH (HGH), and walks through each major option so you can understand which compounds align with different research goals. Whether you are exploring GH peptides for the first time or trying to understand why certain combinations are more popular than others, this article provides the foundation you need.
For a more advanced side-by-side comparison, see Top 6 Growth Hormone Secretagogues Compared.
What Are Growth Hormone Secretagogues?#
Growth hormone secretagogues (GHSs) are compounds that stimulate the pituitary gland to release its own endogenous growth hormone. This is fundamentally different from injecting synthetic HGH (recombinant human growth hormone), which bypasses the pituitary entirely.
The key distinction matters for several reasons:
- Pulsatile release: GH secretagogues preserve the body's natural pattern of GH release in pulses, rather than creating a single large spike
- Feedback preservation: The hypothalamic-pituitary axis continues to regulate GH levels, reducing the risk of supraphysiological elevation
- Endogenous production: The pituitary produces the same growth hormone your body normally makes, rather than introducing an external protein
Growth hormone itself plays roles in body composition, bone density, tissue repair, sleep quality, and metabolic function. Age-related decline in GH secretion -- sometimes called somatopause -- begins in the late 20s, with GH output dropping approximately 14% per decade.
The Two Pathways: GHRH vs. Ghrelin#
Understanding GH secretagogues requires knowing that there are two distinct receptor pathways that control growth hormone release. Every peptide in this class works through one (or both) of these pathways.
The GHRH Pathway#
The growth hormone-releasing hormone (GHRH) receptor sits on somatotroph cells in the anterior pituitary. When GHRH or a GHRH analog binds to this receptor, it directly stimulates GH synthesis and secretion.
Peptides in this class: Sermorelin, Tesamorelin, CJC-1295 (No DAC), CJC-1295 DAC
Characteristics: Clean hormonal profile (minimal cortisol/prolactin effects), physiological GH release, no appetite stimulation
The Ghrelin / GHS-R1a Pathway#
The growth hormone secretagogue receptor (GHS-R1a), also known as the ghrelin receptor, provides a separate mechanism for amplifying GH release. Peptides that activate this receptor are sometimes called GHRPs (growth hormone-releasing peptides).
Peptides in this class: Ipamorelin, GHRP-2, GHRP-6, Hexarelin
Characteristics: Vary widely in selectivity -- some cause significant cortisol, prolactin, and appetite changes while others (ipamorelin) are highly selective
Why This Matters#
The two pathways are complementary. Research demonstrates that activating both pathways simultaneously produces synergistic GH release -- meaning the combined effect is greater than the sum of each pathway activated alone. This is the scientific basis for combination protocols like CJC-1295 + Ipamorelin.
The Beginner-Friendly Options#
Ipamorelin: The Selective Choice#
Ipamorelin is a pentapeptide that activates the GHS-R1a (ghrelin) receptor with unusual selectivity. In clinical studies, it produces dose-dependent GH release without significant changes in cortisol, prolactin, FSH, LH, or TSH levels.
Why beginners favor it: Ipamorelin's clean side effect profile makes it the most forgiving ghrelin-pathway peptide. Studies comparing it directly to GHRP-2 and GHRP-6 found similar GH release but significantly less elevation of ACTH and cortisol. It also produces minimal appetite stimulation, unlike GHRP-6 and GHRP-2.
Evidence level: Phase 2 clinical trials. A study in patients recovering from abdominal surgery demonstrated improved postoperative outcomes, and multiple healthy volunteer studies confirm its GH-releasing activity and selectivity profile.
Common reported effects: Mild headache, transient flushing, injection site reactions.
Sermorelin: The Established Option#
Sermorelin is a synthetic analog of the first 29 amino acids of endogenous GHRH. It was previously FDA-approved (as Geref) for diagnostic evaluation and treatment of GH deficiency in children, though it was voluntarily withdrawn from the market for commercial reasons -- not safety concerns.
Why beginners favor it: Sermorelin has one of the longest clinical track records of any GH secretagogue. Because it works through the GHRH receptor, the resulting GH release follows the body's natural pulsatile pattern with intact negative feedback. A 1997 study demonstrated increased GH secretion in elderly subjects, suggesting partial reversal of age-related decline.
Evidence level: Extensive clinical data from its period as an FDA-approved drug.
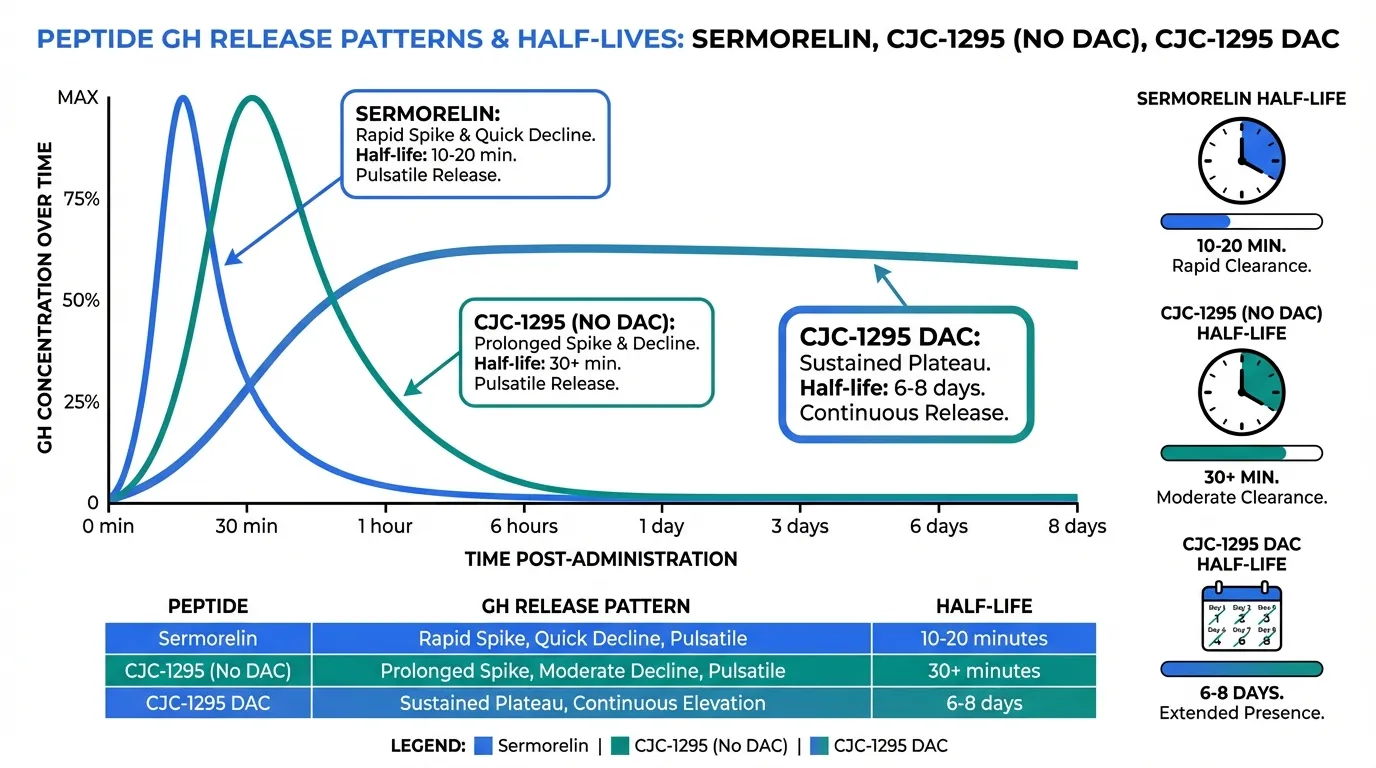
Limitation: Short half-life (approximately 10-20 minutes), which has led many researchers to favor longer-acting GHRH analogs like CJC-1295.
Common reported effects: Injection site reactions, facial flushing, occasional headache.
For a direct comparison of these two, see Ipamorelin vs Sermorelin.
The GHRH Amplifiers: CJC-1295#
CJC-1295 exists in two distinct forms, and understanding the difference is important.
CJC-1295 (No DAC) / Modified GRF 1-29#
CJC-1295 (No DAC) is a modified version of sermorelin with four amino acid substitutions that improve resistance to enzymatic breakdown. This gives it a longer effective half-life (approximately 30+ minutes vs. 10-20 minutes for sermorelin) while still preserving pulsatile GH release.
Best used as: The GHRH component in combination protocols. The most popular research combination pairs CJC-1295 (No DAC) with ipamorelin -- one activating the GHRH receptor, the other the ghrelin receptor.
For more on this combination, see CJC-1295 and Ipamorelin Stack.
CJC-1295 with DAC#
CJC-1295 DAC includes a Drug Affinity Complex that binds to albumin in the bloodstream, extending its half-life to approximately 6-8 days. This creates sustained, continuous GH elevation rather than pulsatile release.
Important distinction: Most research protocols favor the No DAC version because maintaining pulsatile GH release is considered more physiologically appropriate. The DAC version's sustained elevation may downregulate GH receptors over time and does not mimic the body's natural secretion pattern.
The Potent Options: GHRP-2, Hexarelin, and GHRP-6#
These ghrelin-pathway peptides produce stronger GH release than ipamorelin but come with broader hormonal effects. They are generally considered more suitable for experienced researchers who understand the trade-offs.
GHRP-2#
GHRP-2 is one of the most potent GH secretagogues, producing robust and reproducible GH release across numerous clinical studies. It has been studied in aging populations where it partially restored the blunted GH response associated with aging.
Trade-offs: Moderate increases in cortisol and prolactin at higher doses. Appetite stimulation through the ghrelin receptor. Less selective than ipamorelin overall.
Hexarelin#
Hexarelin produces the strongest acute GH release of any peptide in this class. Research has also identified cardioprotective properties through binding to cardiac CD36 receptors -- an effect independent of GH release.
Trade-offs: Significant cortisol and prolactin elevation. Most prone to tachyphylaxis (reduced response with repeated dosing) among all secretagogues -- studies show desensitization within weeks of continuous use.
GHRP-6#
GHRP-6 was one of the earliest ghrelin-pathway peptides developed. It produces reliable GH release but is most notable for its pronounced appetite stimulation -- more so than any other secretagogue.
Trade-offs: Strong hunger response that can be a significant side effect for some research goals. Moderate cortisol and prolactin elevation similar to GHRP-2.
The FDA-Approved Option: Tesamorelin#
Tesamorelin deserves special mention as the only FDA-approved GH secretagogue currently on the market. Sold under the brand name Egrifta, it is approved specifically for HIV-associated lipodystrophy.
Clinical trials demonstrated approximately 15-18% reduction in visceral adipose tissue over 26 weeks. Additional research has explored effects on liver fat, cognitive function in aging adults, and body composition in broader populations. A study in older adults showed improvements in verbal memory and executive function.
For researchers who prioritize clinical validation, tesamorelin offers the most rigorous evidence base in this class.
Quick Comparison Table#
| Feature | Ipamorelin | Sermorelin | CJC-1295 (No DAC) | GHRP-2 | Hexarelin | GHRP-6 | Tesamorelin |
|---|---|---|---|---|---|---|---|
| Pathway | Ghrelin | GHRH | GHRH | Ghrelin | Ghrelin | Ghrelin | GHRH |
| GH Potency | Moderate | Moderate | Moderate | High | Very High | Moderate-High | Moderate-High |
| Selectivity | Very High | High | High | Moderate | Low | Low-Moderate | High |
| Cortisol Impact | Minimal | Minimal | Minimal | Moderate | Significant | Moderate | Minimal |
| Appetite Effect | Low | None | None | Moderate | High | Very High | None |
| Half-Life | ~2 hours | ~10-20 min | ~30+ min | ~15-30 min | ~20-30 min | ~15-30 min | ~26 min |
| Tachyphylaxis | Low | Low | Low | Moderate | High | Moderate | Low |
| FDA Status | Not approved | Previously approved | Not approved | Not approved | Not approved | Not approved | Approved |
| Beginner Suitability | Excellent | Excellent | Good (in combos) | Intermediate | Advanced | Intermediate | Rx only |
Which Secretagogue for Which Goal?#
Anti-Aging and General Wellness Research#
For research focused on age-related GH decline, the most commonly studied approach is a GHRH + GHRP combination -- typically CJC-1295 (No DAC) + ipamorelin. This pairing leverages synergistic GH release while maintaining ipamorelin's clean side effect profile. Sermorelin alone is also studied in this context, supported by research showing partial reversal of somatopause.
Body Composition and Muscle Research#
Researchers interested in body composition effects often look at the more potent secretagogues. GHRP-2 provides strong GH release that supports lean mass and fat metabolism research, though the cortisol and appetite effects must be accounted for. Tesamorelin has the most robust clinical data showing visceral fat reduction.
Sleep and Recovery Research#
GH secretion is naturally highest during slow-wave sleep. GHRH-pathway peptides administered in the evening are studied for their potential to enhance the natural GH pulse during sleep. Sermorelin and CJC-1295 (No DAC) are the most commonly studied in this context, as they do not cause the appetite stimulation that ghrelin-pathway peptides can produce at bedtime.
For more on this connection, see Growth Hormone, Sleep, and Recovery.
Side Effect Profiles Compared#
All GH secretagogues share some potential class effects related to elevated growth hormone, including water retention, joint stiffness, and transient numbness or tingling. However, the off-target hormonal effects vary dramatically between compounds:
- Cleanest profile: Ipamorelin and sermorelin -- minimal impact on cortisol, prolactin, and appetite
- Moderate effects: GHRP-2 and GHRP-6 -- dose-dependent cortisol and prolactin elevation, appetite stimulation
- Broadest effects: Hexarelin -- significant cortisol and prolactin increases, strong appetite stimulation, highest tachyphylaxis risk
The GHRH-pathway peptides (sermorelin, CJC-1295, tesamorelin) generally carry the cleanest profiles because they work through a different receptor system that does not interact with cortisol or appetite regulation.
Combination Protocols: The Synergy Principle#
The most studied approach to GH secretagogue use is not single-peptide protocols but combinations pairing one GHRH-pathway peptide with one ghrelin-pathway peptide. The scientific basis for this is well-established:
- GHRH receptor activation primes somatotroph cells for GH synthesis and release
- GHS-R1a activation amplifies the release signal through a separate intracellular pathway
- Combined activation produces GH output that exceeds the additive effect of either pathway alone
The most commonly studied combination is CJC-1295 (No DAC) + Ipamorelin, which pairs the improved stability of CJC-1295 with ipamorelin's selectivity. For a detailed analysis of this stack, see CJC-1295 and Ipamorelin Stack.
For a broader discussion of how GHRH and GHRP pathways interact, see GHRH vs GHRP: Growth Hormone Explained.
Regulatory Considerations#
It is important to understand the regulatory landscape:
- Tesamorelin (Egrifta) is FDA-approved but only for HIV-associated lipodystrophy
- Sermorelin was previously FDA-approved but has been withdrawn from the market
- All other secretagogues in this guide remain investigational compounds not approved for any therapeutic indication
- CJC-1295 (both forms) was placed under increased regulatory scrutiny following 2024 FDA compounding restrictions
For the latest information on peptide regulation, see FDA Peptide Regulation 2026.
Key Takeaways#
- Growth hormone secretagogues stimulate your pituitary to release endogenous GH, unlike exogenous HGH which bypasses the pituitary entirely
- Two pathways control GH release: the GHRH receptor and the ghrelin receptor (GHS-R1a). Peptides from each class work differently and can be combined for synergistic effects
- Ipamorelin and sermorelin are the most commonly recommended starting points due to their favorable selectivity and side effect profiles
- CJC-1295 (No DAC) is the preferred GHRH analog for combination protocols, offering improved stability over sermorelin
- More potent options (GHRP-2, hexarelin, GHRP-6) produce stronger GH release but with broader hormonal effects including cortisol elevation and appetite stimulation
- Tesamorelin is the only FDA-approved GH secretagogue, offering the highest level of clinical evidence
- Combination protocols pairing GHRH + GHRP pathways produce synergistic effects and represent the most studied approach
This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Growth hormone secretagogues are investigational compounds (except tesamorelin for its approved indication) and should only be used under appropriate medical supervision. Always consult a qualified healthcare provider before making any decisions about peptide therapy.
Related Resources#

{kind=link}
Frequently Asked Questions About Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?
What is the best growth hormone peptide for beginners?
Ipamorelin is widely considered the most beginner-friendly GH secretagogue due to its selective mechanism that stimulates growth hormone release with minimal effects on cortisol, prolactin, and appetite. Sermorelin is another common starting point, particularly because it has a long clinical track record and was previously FDA-approved. The choice depends on individual research goals and whether GHRH-pathway or ghrelin-pathway activation is preferred.
What is the difference between GHRH peptides and GHRP peptides?
GHRH (growth hormone-releasing hormone) peptides like sermorelin and CJC-1295 work by stimulating the GHRH receptor on pituitary cells to trigger GH synthesis and release. GHRP (growth hormone-releasing peptide) compounds like ipamorelin, GHRP-2, and hexarelin activate the ghrelin receptor (GHS-R1a) to amplify GH secretion through a separate pathway. The two pathways are complementary, which is why combination protocols pairing one from each class are commonly studied.
Are growth hormone peptides the same as taking HGH?
No. Exogenous HGH directly introduces synthetic growth hormone into the body, bypassing the pituitary gland entirely. GH secretagogues instead stimulate your own pituitary to produce and release endogenous growth hormone. This preserves the natural pulsatile release pattern and hypothalamic feedback mechanisms, which may result in a more physiological GH profile with potentially fewer side effects than exogenous HGH.
Can you combine different GH peptides together?
Yes, combining a GHRH-pathway peptide with a ghrelin-pathway peptide is the most studied combination approach. The most common pairing is CJC-1295 (No DAC) with ipamorelin. Research suggests this combination produces synergistic GH release greater than either peptide alone, because the two receptor pathways amplify each other's signaling when activated simultaneously.
Is tesamorelin available as a prescription?
Tesamorelin is FDA-approved under the brand name Egrifta specifically for the treatment of HIV-associated lipodystrophy (excess abdominal fat). It is the only GH secretagogue with full FDA approval for a therapeutic indication. All other secretagogues discussed in this guide remain investigational compounds not approved for clinical use.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Best Growth Hormone Peptides Ranked: 2026 Evidence-Based Guide
A ranked comparison of 8 growth hormone secretagogues and related peptides — from FDA-approved tesamorelin to IGF-1 LR3 — evaluating each on mechanism of action, clinical evidence strength, key advantages, and known drawbacks.

Top 6 Growth Hormone Secretagogues Compared
Compare 6 growth hormone secretagogues — ipamorelin, sermorelin, GHRP-2, hexarelin, tesamorelin, and CJC-1295 — by mechanism and side effects.

CJC-1295 + Ipamorelin Stack: Growth Hormone Secretagogue Research Guide
An evidence-based review of the CJC-1295 (no DAC) and ipamorelin peptide stack, examining clinical research on growth hormone stimulation, the rationale for combining GHRH and GHRP pathways, and key limitations.
You Might Also Like
Related content you may find interesting