Peptides for Better Sleep: DSIP, Epitalon, and Growth Hormone Peptides Explained

Introduction#
Sleep is the body's primary recovery state -- a period when growth hormone secretion peaks, tissue repair accelerates, immune surveillance intensifies, and memory consolidation occurs. The relationship between peptides and sleep is bidirectional: certain peptides can influence sleep architecture, while sleep itself provides the physiological context for many peptide-mediated recovery processes.
This guide examines six peptides with research profiles relevant to sleep and nocturnal recovery. These range from DSIP, which was discovered specifically for its sleep-inducing properties, to growth hormone secretagogues like ipamorelin whose sleep relevance stems from the intimate connection between GH release and deep sleep. For each compound, we evaluate the specific mechanism of action, quality of evidence, and important limitations.
Important note: Sleep disorders require proper medical evaluation. No peptide in this guide is FDA-approved for insomnia, sleep disorders, or recovery enhancement. This article is for educational purposes only and does not constitute medical advice.
For a ranked overview of sleep-related peptides, see 5 Best Peptides for Sleep and Recovery. For the broader connection between growth hormone and sleep, see Growth Hormone and Sleep Recovery Connection.
How Peptides Interact with Sleep Architecture#
Sleep architecture refers to the structured cycling between sleep stages that occurs throughout the night. Understanding this architecture is essential for evaluating how different peptides may influence sleep quality.
Sleep Stages and Recovery#
Human sleep cycles through four stages approximately every 90 minutes:
- Stage 1 (N1) -- light transitional sleep lasting 1-5 minutes
- Stage 2 (N2) -- deeper sleep with sleep spindles and K-complexes, comprising about 50% of total sleep
- Stage 3 (N3/slow-wave sleep) -- the deepest non-REM stage, characterized by delta waves. This is the primary recovery stage where growth hormone secretion peaks, tissue repair occurs, and immune function is most active
- REM sleep -- rapid eye movement sleep associated with dreaming, memory consolidation, and emotional processing
The peptides discussed in this guide primarily target Stage 3 (slow-wave sleep) either directly, as with DSIP, or indirectly through growth hormone amplification.
The Growth Hormone-Sleep Axis#
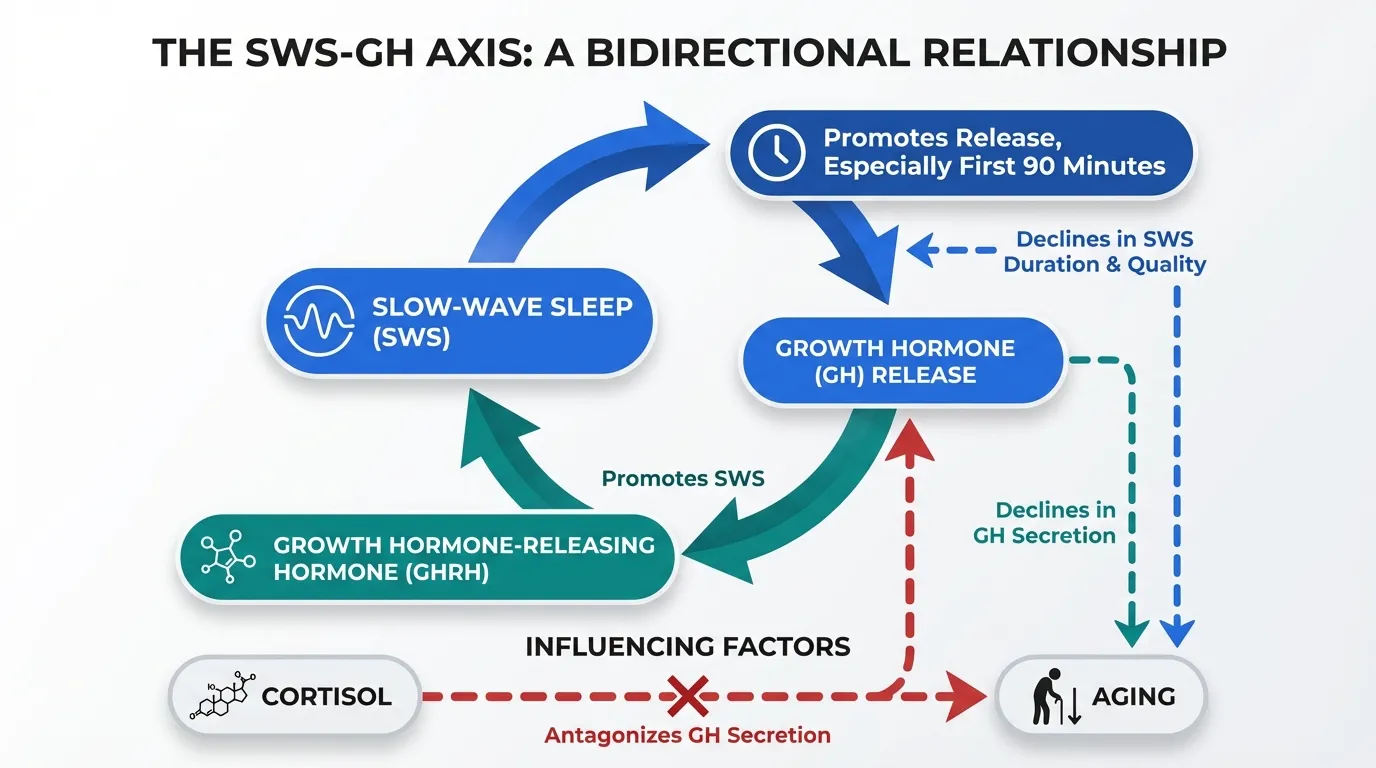
The relationship between GH and sleep is one of the best-characterized hormone-sleep interactions in endocrinology:
- Approximately 75% of daily GH secretion occurs during sleep, with the largest pulse occurring within the first 90 minutes of sleep onset during the initial slow-wave sleep period
- Growth hormone-releasing hormone (GHRH) itself promotes slow-wave sleep when administered to healthy subjects
- GH decline with aging parallels the decline in slow-wave sleep, suggesting a shared regulatory mechanism
- Cortisol, which antagonizes GH release, reaches its nadir during early sleep, creating a permissive window for GH secretion
This bidirectional relationship means that peptides enhancing GH release may indirectly support deep sleep, while peptides improving sleep architecture may enhance the natural GH pulse.
Melatonin and the Circadian Framework#
Melatonin, synthesized by the pineal gland, serves as the body's primary circadian timing signal. It does not directly induce sleep but signals the biological night, preparing the body for sleep onset. Two peptides in this guide -- epitalon and pinealon -- are proposed to influence melatonin synthesis, targeting the hormonal framework that governs when sleep occurs rather than sleep architecture itself.
DSIP: The Delta Sleep-Inducing Peptide#
Evidence Level: Mixed clinical data, primarily older studies (1970s-1990s) | FDA Status: Not approved; not FDA-evaluated
DSIP is a 9-amino-acid nonapeptide (Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu) first isolated in 1977 by Schoenenberger and Monnier from the blood of rabbits during electrically induced sleep. Its discovery specifically in the context of sleep promotion makes it unique among the peptides discussed here.
Mechanism of Action#
DSIP's mechanism of action remains incompletely characterized despite decades of research. Proposed pathways include:
- Delta wave promotion -- DSIP was named for its ability to increase delta wave activity (0.5-4 Hz EEG frequencies) in animal models, the characteristic brainwave pattern of deep slow-wave sleep
- Stress hormone modulation -- some studies report normalization of cortisol and ACTH rhythms, which could create more favorable conditions for sleep onset and GH release
- Endorphin system interaction -- DSIP has been reported to interact with opioid systems, potentially contributing to its analgesic and sleep-modulating properties
- LH and GH modulation -- DSIP may influence the release of luteinizing hormone and growth hormone, linking it to broader endocrine regulation during sleep
Clinical Evidence#
Human studies on DSIP span several decades but present a mixed picture:
- A 1986 study by Schneider-Helmert and Schoenenberger investigated DSIP in chronic insomnia patients and reported improvements in sleep onset and sleep efficiency in a subset of subjects
- Studies in narcolepsy patients showed some effects on sleep organization, though results were inconsistent
- Research in healthy volunteers has produced variable results, with some studies showing increased slow-wave sleep and others finding no significant effect
- Several studies reported improvements in subjective sleep quality, even when objective polysomnographic measures did not consistently change
Limitations#
DSIP research faces significant challenges. Most clinical studies are from the 1980s and 1990s, predating modern sleep research methodology and standards. The peptide degrades rapidly in solution, creating practical difficulties for research and standardization. No specific high-affinity receptor for DSIP has been identified, making it difficult to establish a clear pharmacological mechanism. Results across studies are notably inconsistent, and no modern randomized controlled trials have been conducted.
For a comparison of DSIP with another sleep-related peptide, see Cortistatin vs DSIP.
Epitalon: Melatonin Regulation and Circadian Rhythm#
Evidence Level: Limited clinical data from Russian research groups | FDA Status: Not approved; not FDA-evaluated
Epitalon (also spelled Epithalon) is a synthetic tetrapeptide (Ala-Glu-Asp-Gly) developed by Professor Vladimir Khavinson at the Saint Petersburg Institute of Bioregulation and Gerontology. While primarily studied for its anti-aging properties through telomerase activation, epitalon's sleep relevance stems from its proposed effects on the pineal gland and melatonin production.
Mechanism of Action#
Epitalon's sleep-related mechanism centers on the pineal gland:
- Melatonin synthesis regulation -- epitalon is proposed to stimulate melatonin production by the pineal gland, particularly in aging individuals where melatonin output declines
- Pineal gland bioregulation -- within the Khavinson bioregulator framework, epitalon is theorized to restore age-related functional decline in pinealocytes (melatonin-producing cells)
- Telomerase activation -- epitalon has been reported to activate telomerase in human cell cultures, which has implications for cellular aging but also potentially for maintaining pineal gland function over time
- Circadian rhythm normalization -- by supporting melatonin production, epitalon may help normalize the circadian rhythm disruptions common in aging
Sleep-Relevant Research#
Epitalon's sleep evidence is largely indirect:
- Studies in elderly subjects from the Khavinson research group reported restoration of nighttime melatonin peaks toward levels seen in younger adults
- Animal studies demonstrated that epitalon administration restored circadian cortisol rhythms in aging primates
- Research on pinealocyte cultures showed that epitalon could increase melatonin synthesis in vitro
- Clinical observations in aging cohorts reported subjective improvements in sleep quality alongside melatonin normalization
Limitations#
Epitalon research comes predominantly from a single research group, limiting independent validation. The mechanism by which a four-amino-acid peptide specifically targets pineal gland gene expression has not been convincingly demonstrated through Western research standards. No placebo-controlled trials focused specifically on sleep outcomes (polysomnography, actigraphy) have been published. The bioregulator peptide framework itself remains outside mainstream pharmacological science.
For more on epitalon's broader profile, see Epitalon Overview. For its anti-aging mechanisms, see Hallmarks of Aging and Peptide Interventions.
Growth Hormone Secretagogues and Slow-Wave Sleep#
The growth hormone secretagogues represent the most pharmacologically characterized peptides in this guide. Their sleep relevance is indirect but grounded in well-established GH-sleep physiology.
Ipamorelin: The Selective Secretagogue#
Evidence Level: Clinical data for GH release; indirect sleep evidence | FDA Status: Not approved; investigational
Ipamorelin is a pentapeptide GH secretagogue that binds the ghrelin receptor (GHS-R1a) with high selectivity. Its relevance to sleep centers on two properties:
Selective GH release without cortisol elevation. Unlike older GH secretagogues such as GHRP-6 or hexarelin, ipamorelin stimulates growth hormone without significantly increasing cortisol or prolactin. Since cortisol is a potent sleep disruptor, this selectivity makes ipamorelin particularly suitable for pre-sleep administration. GHRP-2 and hexarelin, by contrast, can elevate cortisol, which may paradoxically interfere with sleep quality even while boosting GH.
Nocturnal GH pulse amplification. When administered 30-60 minutes before sleep, ipamorelin amplifies the natural sleep-onset GH pulse -- the largest single GH secretion event of the day. This augmented GH pulse supports the tissue repair, immune function, and metabolic processes that constitute "recovery" during sleep.
Clinical studies have confirmed ipamorelin's ability to dose-dependently increase GH levels with minimal effects on other pituitary hormones. However, no studies have specifically measured sleep outcomes (polysomnography, sleep latency, sleep efficiency) in ipamorelin-treated subjects.
Sermorelin: The GHRH Analog#
Evidence Level: Clinical data for GH stimulation; some sleep-related GHRH data | FDA Status: Previously FDA-approved (discontinued commercial production)
Sermorelin is the first 29 amino acids of endogenous GHRH, preserving full biological activity at the GHRH receptor. Its sleep-recovery profile has a stronger evidence base than ipamorelin because GHRH itself has been directly studied for sleep effects.
GHRH promotes slow-wave sleep. Multiple studies have demonstrated that intravenous GHRH administration increases slow-wave sleep duration in healthy men. A study by Steiger et al. showed that GHRH injected during early sleep significantly increased time in Stage 3/4 (deep) sleep. As a GHRH analog, sermorelin may share this property, though sermorelin-specific sleep studies are limited.
Age-related decline. Both GH secretion and slow-wave sleep decline in parallel with aging. Sermorelin has been specifically studied in elderly populations for GH restoration, and the overlap between these two age-related declines creates a rationale for sermorelin to address both simultaneously.
Clinical precedent. Sermorelin was previously FDA-approved for GH-deficient children (marketed as Geref), providing a clinical safety track record. Commercial production was discontinued for business reasons, not safety concerns.
For a direct comparison, see Ipamorelin vs Sermorelin.
CJC-1295 (no DAC): The Extended GHRH Analog#
Evidence Level: Clinical Phase 2 data for GH elevation | FDA Status: Not approved; investigational
CJC-1295 (no DAC), also known as Modified GRF (1-29), is a modified sermorelin analog with amino acid substitutions that improve stability and extend its half-life from approximately 10 minutes (sermorelin) to 30 minutes. It is frequently combined with ipamorelin in a GHRH + GHRP protocol that targets both arms of the GH release pathway.
The rationale for combining CJC-1295 (no DAC) with ipamorelin for sleep-related recovery is synergistic: CJC-1295 provides the GHRH signal (which itself may promote slow-wave sleep based on GHRH data) while ipamorelin amplifies the ghrelin-receptor pathway, producing a larger and more sustained GH pulse than either peptide alone. For more on this combination, see CJC-1295 and Ipamorelin Stack.
Pinealon: The Pineal Bioregulator#
Evidence Level: Very limited; single research group | FDA Status: Not approved; not FDA-evaluated
Pinealon is a synthetic tripeptide (Glu-Asp-Arg) from the Khavinson bioregulator framework, proposed to specifically target the pineal gland. Like epitalon, its sleep relevance derives from the pineal gland's role in melatonin production.
Proposed Mechanism#
Pinealon is theorized to regulate gene expression in pinealocytes, supporting melatonin synthesis. The bioregulator hypothesis suggests that short peptides (2-4 amino acids) can interact with specific DNA sequences to modulate transcription in targeted tissues. For the pineal gland, this would theoretically restore age-related declines in melatonin output.
Research Status#
Pinealon's evidence base is extremely thin. Research comes almost exclusively from the Khavinson group. In vitro studies on pinealocyte cultures suggest some effects on melatonin-related gene expression, and animal studies report neuroprotective properties. However, no human clinical trials for sleep outcomes have been published, the mechanism by which a tripeptide achieves tissue-specific gene regulation has not been validated by independent researchers, and the bioregulator framework itself remains outside the mainstream of peptide pharmacology.
Pinealon should be considered highly experimental with insufficient evidence to evaluate its sleep-related claims.
How Sleep Peptides Compare#
| Feature | DSIP | Epitalon | Ipamorelin | Sermorelin | CJC-1295 (no DAC) | Pinealon |
|---|---|---|---|---|---|---|
| Sleep Mechanism | Direct delta wave promotion | Melatonin/circadian regulation | GH amplification | GHRH-mediated GH + possible SWS | Extended GHRH signaling | Proposed melatonin support |
| Sleep-Specific Evidence | Yes (inconsistent) | Indirect (melatonin) | No | Indirect (GHRH-sleep data) | No | Theoretical |
| Clinical Trial Data | Older studies (1980s-90s) | Limited (Russian) | Yes (for GH) | Yes (for GH) | Yes (for GH) | None |
| FDA Status | Not evaluated | Not evaluated | Not approved | Previously approved | Not approved | Not evaluated |
| Cortisol Effect | May normalize | Indirect regulation | No elevation | No significant effect | No significant effect | Unknown |
| Evidence Quality | Low-moderate | Low | Moderate (for GH) | Moderate (for GH) | Moderate (for GH) | Very low |
Timing and the Sleep-Recovery Window#
For peptides targeting the sleep-recovery window, administration timing is a critical consideration:
Pre-Sleep Administration#
Growth hormone secretagogues (ipamorelin, sermorelin, CJC-1295) are typically administered 30-60 minutes before sleep to coincide with the natural sleep-onset GH pulse. This timing leverages two factors: the physiological nadir of cortisol (which opposes GH release) and the onset of slow-wave sleep (which is the natural trigger for the nocturnal GH pulse). Administering GH secretagogues at other times of day still produces GH release but does not synchronize with the sleep-recovery window.
DSIP is similarly administered pre-sleep, consistent with its proposed role in promoting delta wave activity during sleep onset.
Circadian Considerations#
Epitalon and pinealon, which target the melatonin/circadian system, operate on a different timescale. Melatonin production follows a circadian pattern with peak synthesis in darkness. The timing of these peptides would theoretically align with supporting the endogenous melatonin rise that occurs in the evening hours, though specific timing protocols for these peptides have not been established in clinical research.
Fasting Considerations#
Growth hormone release is blunted by elevated insulin and blood glucose. For GH secretagogues, administration on an empty stomach (at least 2 hours after eating) is generally recommended to maximize the GH response. This aligns naturally with pre-sleep administration when dinner has been consumed several hours earlier.
For a comprehensive guide to peptide timing, see Peptide Timing and Circadian Rhythm.
Research Gaps and Future Directions#
The sleep-peptide field has notable research gaps:
- No modern RCTs for DSIP -- the most direct sleep peptide lacks contemporary clinical trials using current polysomnographic methodology
- No sleep-specific studies for GH secretagogues -- while the GH-sleep connection is well-established, no study has specifically measured sleep outcomes (rather than GH levels) for ipamorelin, sermorelin, or CJC-1295
- Limited independent validation for bioregulators -- epitalon and pinealon research remains concentrated in the Khavinson group, with minimal independent replication
- No head-to-head comparisons -- no study has compared any of these peptides against each other or against established sleep interventions
- Sleep architecture vs. subjective quality -- most available data reports subjective sleep quality rather than objective polysomnographic measures
Key Takeaways#
-
DSIP is the only peptide with direct sleep promotion data, but the evidence is inconsistent and largely outdated. It remains the most sleep-specific peptide available for research.
-
Growth hormone secretagogues (ipamorelin, sermorelin, CJC-1295) have the strongest pharmacological evidence for GH release but have not been specifically studied for sleep outcomes. Their sleep relevance relies on the well-established GH-sleep connection.
-
Epitalon targets the circadian framework through melatonin regulation rather than sleep architecture directly. Its evidence comes primarily from a single research group.
-
Pinealon has insufficient evidence to evaluate its sleep-related claims and should be considered highly experimental.
-
No peptide in this guide is FDA-approved for sleep, and none should be considered a replacement for evidence-based sleep interventions. Sleep hygiene, CBT-I, and medical evaluation for sleep disorders remain the standard of care.
-
Timing matters -- for GH secretagogues, pre-sleep administration on an empty stomach aligns with the natural nocturnal GH pulse and the cortisol nadir.
This article is for educational and informational purposes only. It does not constitute medical advice. Always consult a qualified healthcare provider before making decisions about peptide therapy or sleep treatment.
Related Reading#

{kind=link}
Frequently Asked Questions About Peptides for Better Sleep: DSIP, Epitalon, and Growth Hormone Peptides Explained
Which peptide has the most direct evidence for improving sleep?
DSIP (delta sleep-inducing peptide) is the only peptide in this guide with direct clinical studies on sleep outcomes. However, the evidence is inconsistent and largely from older studies conducted in the 1980s and 1990s. No peptide in this guide is FDA-approved for sleep disorders.
How do growth hormone peptides affect sleep?
Growth hormone secretagogues like ipamorelin and sermorelin amplify the natural nocturnal GH pulse that occurs during slow-wave (deep) sleep. Approximately 75% of daily GH secretion occurs during sleep. While these peptides enhance recovery processes that occur during sleep, they have not been directly studied for sleep quality outcomes.
What is the difference between DSIP and epitalon for sleep?
DSIP is proposed to directly modulate sleep architecture by promoting delta wave (slow-wave) sleep. Epitalon works indirectly by regulating the pineal gland and melatonin synthesis, potentially normalizing circadian rhythms. DSIP targets sleep directly while epitalon influences the hormonal framework that governs the sleep-wake cycle.
Are sleep peptides safe to use?
No peptide discussed in this guide is FDA-approved for sleep disorders or insomnia. DSIP, epitalon, and pinealon have not undergone rigorous Phase 3 safety trials. Growth hormone secretagogues like ipamorelin have more clinical safety data but have not been specifically studied for sleep applications. Always consult a healthcare provider before considering any peptide therapy.
Can peptides replace melatonin or sleep medications?
No. Peptides discussed in this guide are research compounds, not established sleep treatments. They should not be considered replacements for evidence-based sleep interventions including sleep hygiene, cognitive behavioral therapy for insomnia (CBT-I), or medications prescribed by a healthcare provider.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.

Best Peptides for Menopause Symptoms: 2026 Research Guide
Research guide covering peptides studied for menopause symptoms including hot flashes, bone loss, cognitive changes, skin aging, sleep disruption, and hormonal regulation.
You Might Also Like
Related content you may find interesting