CJC-1295 + Ipamorelin Stack: Growth Hormone Secretagogue Research Guide

Introduction#
The CJC-1295 and ipamorelin combination is one of the most commonly discussed peptide stacks in growth hormone optimization research. The stack pairs two peptides that stimulate growth hormone (GH) release through different receptor pathways: CJC-1295 (a GHRH analog) acts on the growth hormone-releasing hormone receptor, while ipamorelin (a ghrelin mimetic) acts on the growth hormone secretagogue receptor (GHS-R).
This guide reviews the clinical and preclinical evidence for each peptide, explains the pharmacological rationale for their combination, and identifies the significant gaps in the evidence base that researchers should consider.
Important Regulatory Note: Neither CJC-1295 nor ipamorelin is FDA-approved for any indication. CJC-1295 development was discontinued after a Phase 2 trial death. Both peptides were included in FDA review processes for compounding consideration in 2024.
Understanding the Growth Hormone Axis#
Before examining the individual peptides, it is essential to understand the two-signal system that regulates GH release from the pituitary gland.
The GHRH-GHS Dual Pathway#
Growth hormone release is controlled by two stimulatory inputs and one inhibitory input:
-
GHRH (Growth Hormone-Releasing Hormone): Released from the hypothalamus, GHRH binds to GHRH receptors on pituitary somatotrophs and initiates GH synthesis and release through cAMP-PKA signaling.
-
Ghrelin / GHS: Ghrelin and synthetic growth hormone secretagogues bind to GHS-R1a receptors on somatotrophs, amplifying GH release through IP3-PKC signaling. This pathway acts synergistically with GHRH signaling.
-
Somatostatin (Inhibitory): Released in pulses from the hypothalamus, somatostatin suppresses GH release. The natural GH pulse pattern results from the interplay between GHRH stimulation and somatostatin inhibition.
The CJC-1295 + ipamorelin stack targets both stimulatory pathways simultaneously, which is the core pharmacological rationale for the combination.
Component 1: CJC-1295 (Modified GRF 1-29)#
What It Is#
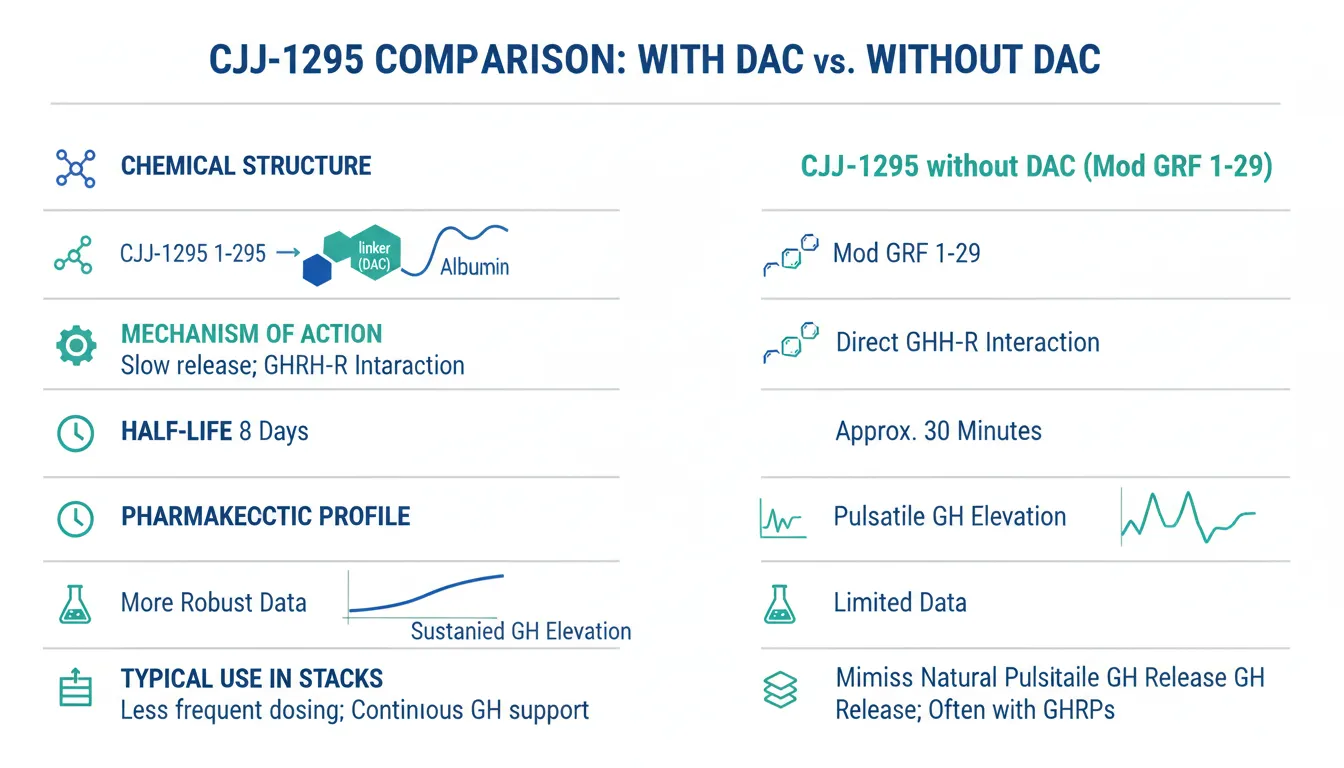
CJC-1295 exists in two forms that are frequently confused:
- CJC-1295 with DAC (Drug Affinity Complex): A modified GHRH analog with a maleimidopropionic acid linker that binds to serum albumin, extending its half-life to approximately 8 days. This is the form used in most published clinical trials.
- CJC-1295 without DAC (Mod GRF 1-29): A tetra-substituted 29-amino-acid GHRH analog with amino acid modifications at positions 2, 8, 15, and 27 to resist enzymatic degradation. Its half-life is approximately 30 minutes, much shorter than the DAC version.
The "stack" typically refers to CJC-1295 without DAC, as its shorter half-life allows for pulsatile GH release that more closely mimics natural physiology. However, the most robust clinical data exists for the DAC version.
Clinical Research (CJC-1295 with DAC)#
The landmark clinical study by Teichman et al. (2006) remains the most cited evidence for CJC-1295's efficacy 1:
- Design: Randomized, placebo-controlled, ascending dose study in 21 healthy adults
- Results: Single subcutaneous injections produced dose-dependent increases in mean plasma GH concentrations by 2-fold to 10-fold for 6 or more days
- IGF-1 response: Mean plasma IGF-I concentrations increased by 1.5-fold to 3-fold for 9-11 days
- GH pulsatility: Importantly, CJC-1295 increased trough and mean GH secretion while preserving the natural pulsatile pattern of GH release 2
A follow-up study confirmed that pulsatile GH secretion persists during continuous stimulation by CJC-1295, with approximately 7.5-fold increase in GH pulse amplitude relative to placebo 2.
Clinical Research (CJC-1295 without DAC / Mod GRF 1-29)#
Published clinical data specifically for the no-DAC variant is more limited. The pharmacological modifications (substitutions at positions 2, 8, 15, 27) increase resistance to enzymatic degradation compared to native GRF(1-29), but the shorter half-life means effects are measured in hours rather than days.
Safety and Discontinuation#
CJC-1295 development was discontinued following the death of a participant during Phase 2 clinical trials. While the specific circumstances are not fully detailed in published literature, this event halted further clinical development of the compound.
Component 2: Ipamorelin#
What It Is#
Ipamorelin is a synthetic pentapeptide (Aib-His-D-2-Nal-D-Phe-Lys-NH2) that acts as a selective growth hormone secretagogue through the ghrelin receptor (GHS-R1a). First described by Raun et al. in 1998, it was identified as the first GHS with selectivity for GH release comparable to that of GHRH itself 3.
Selectivity: The Key Differentiator#
Ipamorelin's primary advantage over other ghrelin mimetics (such as GHRP-2, GHRP-6, and hexarelin) is its selectivity. In clinical research:
- No significant ACTH or cortisol release: Unlike GHRP-2 and GHRP-6, ipamorelin did not stimulate ACTH or cortisol release at doses more than 200-fold higher than the effective dose for GH stimulation 3.
- No significant prolactin elevation: Ipamorelin does not meaningfully increase prolactin levels, which is a concern with less selective secretagogues.
- Dose-dependent GH release: The GH response is proportional to dose, allowing more predictable titration.
This selectivity profile means ipamorelin stimulates GH release without activating the hypothalamic-pituitary-adrenal (HPA) axis, a significant advantage for research applications where cortisol confounding is undesirable.
Clinical Research#
Postoperative ileus studies: Ipamorelin was evaluated in Phase 2 clinical trials for postoperative ileus (delayed return of bowel function after abdominal surgery). At 0.03 mg/kg twice daily for up to 7 days, ipamorelin was well tolerated 4.
Growth hormone deficiency context: A 2017 review of growth hormone secretagogues noted that ipamorelin and other GHS compounds appear safe, with few studies observing serious adverse events, though safety data remain limited due to short study durations and small sample sizes 5.
Body composition research: A 2020 review examined the role of growth hormone secretagogues in body composition management, noting that compounds like ipamorelin can significantly influence adiposity and lean mass through GH-mediated pathways 6.
The Rationale for Combining CJC-1295 and Ipamorelin#
Dual-Receptor Synergism#
The primary pharmacological rationale is based on well-established endocrinology. GHRH and ghrelin act through separate receptor systems that converge on somatotroph cells:
| Feature | CJC-1295 (GHRH Analog) | Ipamorelin (GHS Agonist) |
|---|---|---|
| Target receptor | GHRH-R | GHS-R1a (ghrelin receptor) |
| Signaling pathway | cAMP-PKA | IP3-PKC |
| Primary effect | GH synthesis + release | GH release amplification |
| Duration | Sustained (with DAC) / Pulsatile (no DAC) | Acute pulse |
| HPA axis effects | Minimal | None at therapeutic doses |
When both pathways are activated simultaneously, the resulting GH pulse is typically greater than the additive effect of either alone -- this is genuine pharmacological synergism based on convergent intracellular signaling in somatotrophs 5.
The "Pulse + Sustain" Model#
The no-DAC version of CJC-1295 is preferred for this stack because:
- CJC-1295 (no DAC) provides a moderate, sustained increase in baseline GH signaling (lasting approximately 30-60 minutes)
- Ipamorelin adds a sharp, selective GH pulse on top of that elevated baseline
- The combination mimics the natural GH secretion pattern more closely than either peptide alone
This is analogous to how endogenous GHRH and ghrelin work together: GHRH primes the somatotrophs while ghrelin amplifies the pulse.
Evidence for the Combination#
While the dual-receptor synergism between GHRH and ghrelin pathways is well-established in endocrinology, specific clinical data for CJC-1295 + ipamorelin as a combined protocol is limited:
- No published randomized controlled trials have tested the specific CJC-1295 + ipamorelin combination
- The synergism data comes from studies using native GHRH and ghrelin, or from other GHRH/GHS combinations
- Dosing ratios and timing protocols for the specific combination have not been optimized in clinical settings
Potential Applications in Research#
Body Composition#
Growth hormone influences body composition through multiple pathways: promotion of lipolysis (fat breakdown), preservation of lean mass, and regulation of protein synthesis. Clinical data from GH-deficient populations shows that GH replacement improves body composition parameters, but extrapolation to GH-sufficient adults is not straightforward 6.
Age-Related GH Decline#
GH secretion declines approximately 14% per decade after age 30, a phenomenon termed somatopause. The CJC-1295 + ipamorelin stack is sometimes discussed in the context of age-related GH decline, though no clinical trials have specifically evaluated this combination for anti-aging endpoints.
Recovery and Sleep#
GH is released primarily during slow-wave sleep, and GH secretagogues may influence sleep architecture. However, clinical data on the CJC-1295 + ipamorelin combination's effects on sleep quality or recovery are absent from the published literature.
Safety Profile#
Ipamorelin Safety#
- Well tolerated in Phase 2 clinical trials at 0.03 mg/kg twice daily 4
- No significant cortisol, ACTH, or prolactin elevation at therapeutic doses 3
- Adverse effects reported as rare and similar to those seen with sermorelin 5
CJC-1295 Safety#
- The DAC version demonstrated dose-dependent increases in GH and IGF-1 that were generally well tolerated 1
- One death during Phase 2 clinical trials led to discontinuation of development
- Injection site reactions (redness, swelling) were the most common reported adverse effects
Combination Safety Concerns#
- No published safety data exists specifically for the CJC-1295 + ipamorelin combination
- Theoretical risk of excessive GH elevation with dual-pathway stimulation
- Chronic GH elevation above physiological levels carries known risks including insulin resistance, joint pain, fluid retention, and potential effects on cancer biology
- The effect of long-term secretagogue use on pituitary somatotroph function and potential for desensitization has not been studied
- Quality control of research peptides varies significantly across sources
Comparison with Other GH Secretagogue Approaches#
| Approach | GH Selectivity | Duration | Human Clinical Data | Key Limitation |
|---|---|---|---|---|
| CJC-1295 + Ipamorelin | High (ipamorelin) | Hours (no DAC) | Limited for combination | No combination trials |
| Sermorelin | Moderate | 30-60 min | FDA-approved (discontinued) | Discontinued commercially |
| GHRP-2 + GHRH | Lower | Hours | Moderate | Cortisol/prolactin elevation |
| GHRP-6 + GHRH | Lower | Hours | Moderate | Appetite stimulation, cortisol |
| Hexarelin | Low | Hours | Moderate | Rapid tachyphylaxis |
| Tesamorelin | Moderate | Hours | FDA-approved (HIV lipodystrophy) | Approved for specific indication only |
| MK-677 (oral) | Moderate | 24+ hours | Phase 2 data | Appetite stimulation, insulin resistance |
Key Takeaways for Researchers#
-
The dual-receptor rationale is pharmacologically sound. GHRH and ghrelin pathway co-activation produces synergistic GH release through well-characterized intracellular mechanisms. This is established endocrinology, not speculation.
-
The specific combination lacks clinical validation. While the pathways are well understood, no published clinical trial has tested CJC-1295 + ipamorelin together. Efficacy claims for the specific combination are extrapolations.
-
Ipamorelin's selectivity is its key advantage. Unlike older ghrelin mimetics, ipamorelin does not significantly elevate cortisol, ACTH, or prolactin, making it a cleaner research tool for studying GH-specific effects.
-
CJC-1295's clinical history includes a safety signal. The death during Phase 2 trials led to program discontinuation. This should be weighed in any risk-benefit assessment.
-
DAC vs. no-DAC distinction matters. Most published CJC-1295 clinical data is for the DAC version, which has fundamentally different pharmacokinetics than the no-DAC variant used in this stack.
-
Long-term effects are unknown. Chronic elevation of GH above physiological levels carries theoretical risks including insulin resistance and effects on cancer biology. No long-term studies exist for this combination.
-
Neither peptide is FDA-approved for growth hormone optimization, body composition, anti-aging, or any other indication in the general population.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
Footnotes#
-
Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. PMID: 16352683. 2006. ↩ ↩2
-
Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. PMID: 17018654. 2006. ↩ ↩2
-
Ipamorelin, the first selective growth hormone secretagogue. PMID: 9849822. 1998. ↩ ↩2 ↩3
-
Growth hormone secretagogues: history, mechanism of action, and clinical development. DOI: 10.1002/rco2.9. 2020. ↩ ↩2
-
The Safety and Efficacy of Growth Hormone Secretagogues. PMC: 5632578. 2017. ↩ ↩2 ↩3
-
Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. PMC: 7108996. 2020. ↩ ↩2

{kind=link}
Frequently Asked Questions About CJC-1295 + Ipamorelin Stack: Growth Hormone Secretagogue Research Guide
What does this article cover?
An evidence-based review of the CJC-1295 (no DAC) and ipamorelin peptide stack, examining clinical research on growth hormone stimulation, the rationale for combining GHRH and GHRP pathways, and key limitations. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Ipamorelin. Key context: Ipamorelin (Primary stack component - selective GH secretagogue acting through ghrelin receptor pathway). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "CJC-1295 + Ipamorelin Stack: Growth Hormone Secretagogue Research Guide." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What is Ipamorelin and why is it significant?
Ipamorelin is a peptide discussed in this article because: Primary stack component - selective GH secretagogue acting through ghrelin receptor pathway. For a complete profile of Ipamorelin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?
A beginner-friendly guide to growth hormone secretagogues including ipamorelin, sermorelin, CJC-1295, and more. Learn how GH peptides work, compare options, and understand which secretagogue may fit your research goals.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.

Top 6 Growth Hormone Secretagogues Compared
Compare 6 growth hormone secretagogues — ipamorelin, sermorelin, GHRP-2, hexarelin, tesamorelin, and CJC-1295 — by mechanism and side effects.
You Might Also Like
Related content you may find interesting