Kisspeptin and Fertility Peptides: Research on Reproductive Hormone Regulation

Introduction#
Reproductive medicine has relied on peptide hormones since the earliest days of assisted reproduction. From the isolation of gonadotropins in the 1960s to the discovery of kisspeptin's role as the master regulator of the reproductive axis in the early 2000s, peptides have been central to understanding and treating infertility.
This review examines six peptides with established or emerging roles in fertility medicine. Three — HCG, HMG, and gonadorelin — are foundational agents in clinical reproductive medicine with decades of use. Triptorelin serves dual roles in fertility preservation and assisted reproduction protocols. Kisspeptin and its synthetic analog MVT-602 represent the newest frontier, with research exploring whether targeting the kisspeptin-GnRH pathway can improve outcomes and reduce complications in fertility treatment.
For peptides studied in sexual function rather than fertility, see Peptides for Sexual Health and Peptides for Men's Sexual Health.
The Reproductive Hormone Cascade#
Understanding fertility peptides requires a clear picture of the hypothalamic-pituitary-gonadal (HPG) axis:
- Kisspeptin neurons in the hypothalamus act as the upstream regulators, integrating metabolic, circadian, and stress signals to determine reproductive readiness
- GnRH neurons receive kisspeptin input and release gonadotropin-releasing hormone in a pulsatile pattern into the hypophyseal portal circulation
- Anterior pituitary gonadotrophs respond to GnRH pulses by secreting luteinizing hormone (LH) and follicle-stimulating hormone (FSH) into the systemic circulation
- Gonads respond to LH and FSH — in women, FSH drives follicular development and LH triggers ovulation; in men, FSH supports spermatogenesis and LH stimulates testosterone production
- Feedback loops — gonadal steroids (estradiol, progesterone, testosterone) and peptides (inhibin, activin) feed back to the hypothalamus and pituitary to modulate the axis
Each fertility peptide discussed below acts at a specific level of this cascade, and the therapeutic strategy depends on where in the cascade the dysfunction lies.
1. Kisspeptin: The Master Regulator#
Evidence Level: Clinical research studies; not approved for fertility indications Primary Mechanism: Activation of KISS1R (GPR54) on GnRH neurons FDA Status: Investigational
Role in Reproductive Physiology#
Kisspeptin is encoded by the KISS1 gene and acts through the KISS1 receptor (GPR54, now officially named KISS1R) on GnRH neurons. The discovery that loss-of-function mutations in KISS1R cause hypogonadotropic hypogonadism (failure to enter puberty and infertility) established kisspeptin as essential for reproductive function in humans.
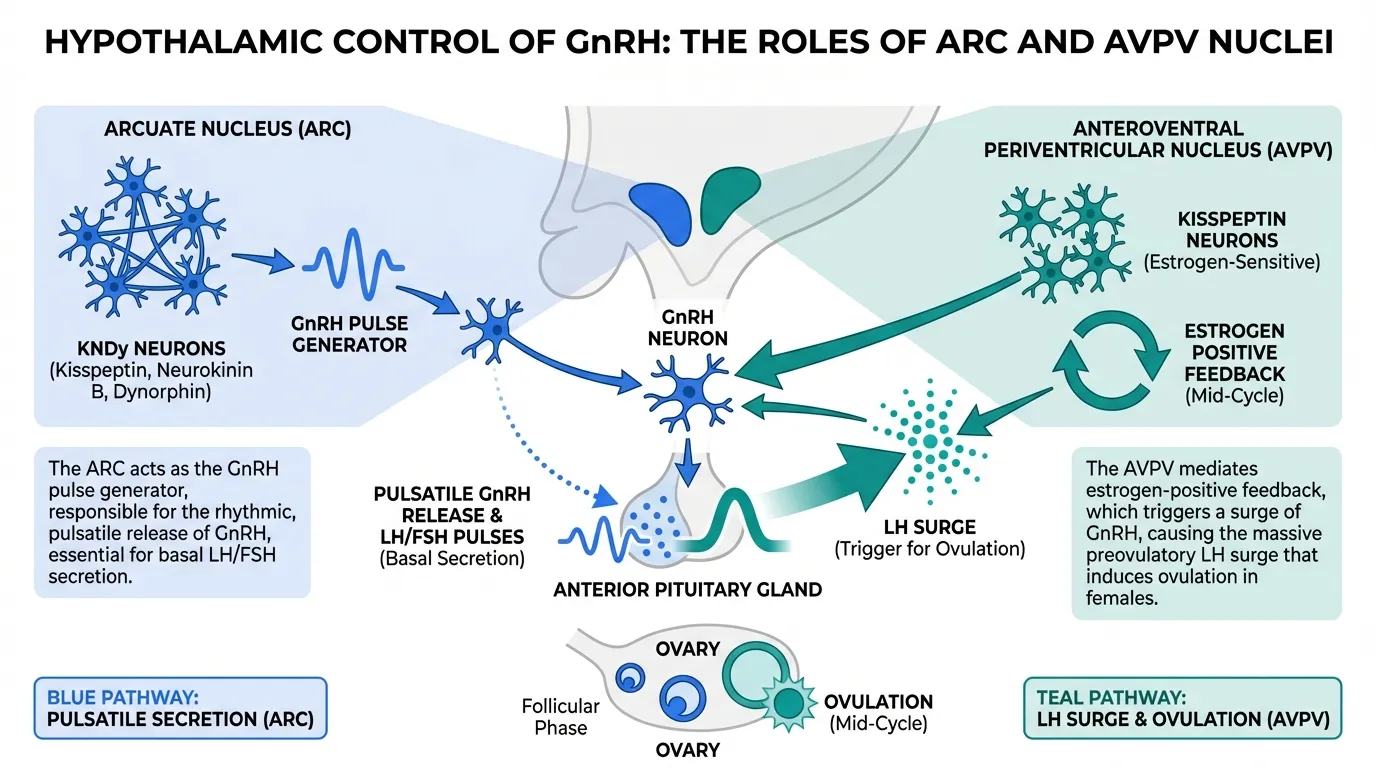
Kisspeptin neurons are concentrated in two hypothalamic nuclei with distinct roles:
- Arcuate nucleus (ARC) — kisspeptin neurons here co-express neurokinin B and dynorphin (the "KNDy" neurons) and function as the GnRH pulse generator. They are responsible for the pulsatile pattern of GnRH release that is essential for gonadotropin secretion
- Anteroventral periventricular nucleus (AVPV) — kisspeptin neurons in this region mediate the estrogen-positive feedback that triggers the LH surge and ovulation in females. This population is sexually dimorphic, being larger in females
Clinical Research in Fertility#
Kisspeptin's potential in fertility medicine has been explored primarily through work at Imperial College London and other academic centers:
- Ovulation trigger — kisspeptin-54 administration can trigger an LH surge sufficient for oocyte maturation in women undergoing IVF. In a proof-of-concept study, subcutaneous kisspeptin-54 (6.4 nmol/kg) triggered oocyte maturation with a 90% mature oocyte rate and no cases of ovarian hyperstimulation syndrome (OHSS)
- OHSS risk reduction — the physiological nature of kisspeptin-triggered LH surges (they are shorter and more closely resemble natural surges than HCG-triggered surges) may inherently reduce OHSS risk. This is kisspeptin's most compelling clinical advantage, since OHSS remains a serious complication of assisted reproduction
- Dose-response characterization — studies have explored multiple kisspeptin-54 doses for ovulation triggering, establishing that higher doses produce more robust LH surges and higher oocyte yields, with an apparent therapeutic window that balances efficacy and physiological response
- Male reproductive function — kisspeptin administration in men produces acute increases in LH and testosterone, supporting potential applications in male hypogonadotropic hypogonadism
Limitations#
Native kisspeptin-54 has a circulating half-life of approximately 28 minutes, requiring careful timing relative to oocyte retrieval. The short duration of the kisspeptin-induced LH surge may be insufficient for adequate luteal phase support, potentially requiring supplemental progesterone. Large randomized controlled trials comparing kisspeptin trigger to standard HCG or GnRH agonist triggers have not been completed. The clinical research remains at the proof-of-concept stage, with small sample sizes limiting definitive conclusions about efficacy relative to established triggers.
2. MVT-602: A Kisspeptin Receptor Agonist#
Evidence Level: Phase 2 clinical trials Primary Mechanism: KISS1R agonist with extended duration of action FDA Status: Investigational (Myovant Sciences)
Rationale and Development#
MVT-602 was developed to overcome kisspeptin-54's pharmacokinetic limitations. As a synthetic kisspeptin receptor agonist, MVT-602 retains the ability to stimulate GnRH release through the physiological KISS1R pathway but with a longer duration of action that could make kisspeptin-based therapies clinically practical.
Clinical Evidence#
- Phase 1 study — MVT-602 demonstrated dose-dependent stimulation of LH and FSH in healthy women, with the LH response peaking later and lasting longer than that produced by native kisspeptin-54. The duration of LH elevation was considered potentially suitable for an ovulation trigger in IVF
- Phase 2 IVF trigger study — MVT-602 was evaluated as an ovulation trigger in women undergoing IVF. Results demonstrated successful oocyte maturation, though the complete dataset has not been fully published as of the latest available reports
- Safety profile — MVT-602 was generally well-tolerated in early clinical studies, with injection site reactions and transient hot flushes among the reported adverse events. No OHSS cases were reported in initial studies, consistent with the expected physiological advantage of kisspeptin pathway stimulation
Potential Advantages Over Current Triggers#
If MVT-602 confirms its early promise, it could offer several advantages over existing ovulation triggers: a more physiological LH surge profile compared to HCG, reduced OHSS risk compared to HCG (the standard trigger), longer duration of action than native kisspeptin-54, and a simpler single-injection protocol compared to GnRH agonist triggers that require prior GnRH antagonist co-treatment.
3. Gonadorelin: The GnRH Standard#
Evidence Level: FDA-approved for diagnostic use; established therapeutic use Primary Mechanism: GnRH receptor agonist; pulsatile administration stimulates gonadotropin release FDA Status: Approved for diagnostic testing (Factrel)
Role in Fertility Medicine#
Gonadorelin is a synthetic decapeptide identical to endogenous GnRH. Its fertility applications span both diagnostic and therapeutic roles:
Diagnostic Applications#
- GnRH stimulation test — a single bolus of gonadorelin followed by serial LH and FSH measurements distinguishes hypothalamic from pituitary causes of hypogonadotropic hypogonadism. A normal LH rise indicates intact pituitary function with hypothalamic dysfunction; a blunted response suggests pituitary pathology
- Pubertal assessment — the GnRH stimulation test helps evaluate delayed puberty and precocious puberty by assessing pituitary gonadotroph maturity
Therapeutic Applications#
- Hypothalamic amenorrhea — pulsatile GnRH therapy via programmable pump is the most physiological treatment for hypothalamic amenorrhea (functional or organic). By delivering GnRH every 60-120 minutes, the pump mimics natural pulsatile secretion, restoring normal gonadotropin patterns, follicular development, and ovulation. Ovulation rates exceed 90% with cumulative pregnancy rates comparable to gonadotropin therapy, but with lower rates of multiple pregnancy
- Male hypogonadotropic hypogonadism — pulsatile GnRH restores testosterone production and spermatogenesis in men with hypothalamic GnRH deficiency, including Kallmann syndrome. This approach preserves fertility, unlike exogenous testosterone replacement
- Ovulation induction — in women with WHO Group I anovulation (hypogonadotropic hypogonadism), pulsatile GnRH produces mono-follicular ovulation in most cycles, significantly reducing the risk of multiple pregnancy compared to gonadotropin stimulation
Key Pharmacological Principle#
The critical distinction with gonadorelin is between pulsatile and continuous administration. Pulsatile delivery (every 60-120 minutes) stimulates the reproductive axis. Continuous or high-dose administration causes GnRH receptor downregulation and desensitization, suppressing gonadotropin secretion — the same principle exploited by GnRH agonists like triptorelin for indications requiring hormonal suppression.
4. HCG: The Ovulation Trigger#
Evidence Level: FDA-approved; decades of clinical use in assisted reproduction Primary Mechanism: LH/CG receptor agonist with prolonged action FDA Status: Approved for multiple reproductive indications
Role in Fertility Medicine#
HCG is a glycoprotein hormone naturally produced by the placenta. Its alpha subunit is structurally identical to LH, FSH, and TSH, while its unique beta subunit confers LH receptor specificity with significantly longer half-life than native LH (approximately 24-36 hours vs. 20 minutes for LH).
Clinical Applications#
HCG is arguably the most widely used peptide in reproductive medicine:
- Ovulation trigger in IVF — HCG has been the standard ovulation trigger in IVF for decades. A single injection of HCG (typically 5,000-10,000 IU of urinary HCG or 250 mcg of recombinant HCG/choriogonadotropin alfa) mimics the natural LH surge, triggering final oocyte maturation approximately 36 hours before scheduled oocyte retrieval
- Ovulation induction — in non-IVF fertility treatment (timed intercourse or intrauterine insemination), HCG is administered when follicle monitoring confirms a mature follicle, providing a predictable ovulation window
- Luteal phase support — HCG's long half-life provides sustained LH receptor stimulation that supports the corpus luteum during the early luteal phase, maintaining progesterone production until placental steroidogenesis takes over
- Male fertility — HCG stimulates Leydig cell testosterone production, supporting spermatogenesis in men with hypogonadotropic hypogonadism. It is often combined with FSH (or HMG) for optimal sperm production
- Cryptorchidism — HCG is FDA-approved for promoting testicular descent in prepubertal boys with cryptorchidism, though surgical orchiopexy is generally preferred
OHSS Risk#
The principal limitation of HCG as an ovulation trigger is its association with OHSS. HCG's prolonged LH receptor stimulation (due to its long half-life) can sustain and amplify the vasoactive mediator release from hyperstimulated ovaries that underlies OHSS. This risk is the primary driver behind the development of alternative triggers including GnRH agonists and kisspeptin. Risk factors for OHSS include polycystic ovary syndrome, high antral follicle count, elevated estradiol levels, and previous OHSS episodes.
5. HMG: Combined Gonadotropin Therapy#
Evidence Level: FDA-approved; established standard of care Primary Mechanism: Combined FSH and LH activity for ovarian stimulation FDA Status: Approved (Menopur, Repronex)
Composition and Mechanism#
HMG (human menopausal gonadotropin) is extracted from the urine of postmenopausal women and contains both FSH and LH activity in an approximately 1:1 ratio. The LH activity in modern highly purified HMG preparations (such as Menopur) is derived primarily from HCG co-purified with FSH, rather than from LH itself. This distinction is clinically relevant because HCG has a longer half-life than LH, providing more sustained LH receptor stimulation.
Clinical Applications#
- Ovarian stimulation for IVF — HMG is used as part of controlled ovarian hyperstimulation protocols, either alone or in combination with recombinant FSH. The LH activity in HMG may be particularly beneficial for women with profound LH suppression from GnRH antagonist protocols or those over 35, where some LH activity appears to improve follicular steroidogenesis and oocyte quality
- Ovulation induction — in women with WHO Group II anovulation (most commonly PCOS), HMG can be used in low-dose step-up protocols for ovulation induction with timed intercourse or IUI
- Male infertility — HMG provides both FSH (for Sertoli cell function and spermatogenesis) and LH activity (for testosterone production), making it a single-agent option for men with hypogonadotropic hypogonadism, though it is often used in combination with HCG
HMG vs. Recombinant FSH#
The clinical choice between HMG and recombinant FSH (follitropin alfa or beta) has been extensively debated. Meta-analyses have shown comparable live birth rates, though some studies suggest HMG may produce modestly higher implantation rates and lower OHSS risk in certain populations. The endogenous LH activity in HMG may provide a more physiological hormonal milieu during follicular development compared to pure FSH preparations.
6. Triptorelin: GnRH Agonist in Fertility#
Evidence Level: FDA-approved for other indications; extensive fertility data Primary Mechanism: GnRH agonist; initial flare followed by receptor downregulation and suppression FDA Status: Approved for prostate cancer (Trelstar); fertility uses are off-label
Dual Role in Fertility Medicine#
Triptorelin is a synthetic GnRH agonist with a potency approximately 100 times that of native GnRH. In fertility medicine, triptorelin serves two distinct and seemingly contradictory roles, depending on the clinical context:
Role 1: Ovulation Trigger (GnRH Agonist Trigger)#
When administered as a single bolus in women who have been pre-treated with a GnRH antagonist (which prevents premature LH surges during ovarian stimulation), triptorelin produces an acute "flare" of LH and FSH release. This flare mimics the natural LH surge and can trigger oocyte maturation. The advantages of the GnRH agonist trigger include:
- Reduced OHSS risk — the LH surge from a GnRH agonist trigger is shorter in duration than the prolonged stimulation from HCG, resulting in faster resolution of ovarian hyperstimulation. This approach has virtually eliminated severe OHSS in high-risk patients
- Physiological LH and FSH surge — unlike HCG (which provides only LH activity), the GnRH agonist trigger produces both LH and FSH, more closely mimicking the natural midcycle surge
- Luteal phase deficit — the rapid decline in LH after a GnRH agonist trigger leads to inadequate corpus luteum support, requiring aggressive luteal phase supplementation with progesterone and estradiol, or a "dual trigger" approach combining low-dose HCG with the GnRH agonist
Role 2: Fertility Preservation During Chemotherapy#
GnRH agonists including triptorelin have been studied for ovarian protection during gonadotoxic chemotherapy:
- POEMS/OPTION trials — randomized controlled trials demonstrated that GnRH agonist co-treatment during chemotherapy reduced the rate of premature ovarian insufficiency (POI) and preserved ovarian reserve in premenopausal women with breast cancer
- PROMISE-GIM6 trial — this randomized trial showed that triptorelin administered before and during chemotherapy for early breast cancer reduced the incidence of chemotherapy-induced POI from 25.9% in controls to 8.9% in the triptorelin group
- Mechanism — the proposed mechanisms include reducing ovarian blood flow (decreasing chemotherapy exposure), maintaining follicles in a quiescent gonadotropin-independent state, and upregulating anti-apoptotic factors
Side Effects in Fertility Context#
In the fertility setting, triptorelin's side effects differ from its long-term use in prostate cancer. For single-dose ovulation trigger, side effects are minimal and transient. For fertility preservation during chemotherapy, the main effects are those of reversible menopause (hot flushes, mood changes, vaginal dryness, decreased bone density) during the treatment period, which resolve after discontinuation.
How These Peptides Fit Together in Clinical Practice#
In a typical IVF cycle, multiple fertility peptides may be used sequentially:
- Suppression phase — GnRH antagonist (or agonist in long protocols) prevents premature ovulation
- Stimulation phase — HMG or recombinant FSH stimulates multiple follicular development
- Trigger phase — HCG, GnRH agonist (triptorelin), or potentially kisspeptin/MVT-602 triggers final oocyte maturation
- Luteal support — progesterone (and sometimes HCG) supports the corpus luteum for embryo implantation
Understanding each peptide's role in this cascade clarifies why no single agent is sufficient and why the sequencing and timing of administration is critical.
Emerging Directions#
Several developments may reshape fertility peptide therapy:
- Kisspeptin-based triggers — if kisspeptin or MVT-602 can replicate the efficacy of HCG triggers while eliminating OHSS risk, they could become the preferred trigger for high-risk patients or potentially all IVF cycles
- Oral GnRH antagonists — oral formulations could simplify suppression protocols by eliminating daily injections
- Personalized gonadotropin dosing — pharmacogenomic approaches to individualize FSH/LH dosing based on receptor polymorphisms and metabolic markers
- KNDy neuron-targeted therapies — understanding the kisspeptin/neurokinin B/dynorphin (KNDy) system could yield new therapeutic targets for anovulatory infertility
- Male fertility optimization — kisspeptin analogs could provide a more physiological approach to stimulating testosterone and spermatogenesis in men with hypothalamic hypogonadism compared to HCG
Conclusion#
Fertility medicine relies on a well-characterized cascade of peptide hormones, from kisspeptin at the top of the axis to gonadotropins acting directly on the gonads. Gonadorelin remains the gold standard for pulsatile GnRH replacement in hypothalamic amenorrhea. HCG and HMG are foundational agents in assisted reproduction with decades of clinical data supporting their use. Triptorelin serves specialized roles in OHSS prevention and fertility preservation during chemotherapy.
The emergence of kisspeptin and MVT-602 represents a potential paradigm shift — moving the point of intervention upstream to the kisspeptin-GnRH interface, where the natural physiological cascade can be recruited rather than bypassed. If clinical development confirms the early promise of reduced OHSS risk with maintained efficacy, kisspeptin-based therapies could fundamentally alter how ovulation is triggered in assisted reproduction.
For related content, see Peptides for Sexual Health, Peptides for Men's Sexual Health, and the Alprostadil vs PT-141 comparison. For dosing tools, visit the Dosing Calculator.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Gonadorelin Overview and Research Guide
- Gonadorelin Dosing Protocols
- Gonadorelin Side Effects and Safety
- HCG Overview and Research Guide
- HCG Dosing Protocols
- HCG Side Effects and Safety
- HMG Overview and Research Guide
- HMG Dosing Protocols
- HMG Side Effects and Safety
- MVT-602 Overview and Research Guide
- MVT-602 Dosing Protocols
- MVT-602 Side Effects and Safety
- Triptorelin Overview and Research Guide
- Triptorelin Dosing Protocols
- Triptorelin Side Effects and Safety

{kind=link}
Frequently Asked Questions About Kisspeptin and Fertility Peptides: Research on Reproductive Hormone Regulation
What does this article cover?
Review of kisspeptin, gonadorelin, HCG, HMG, triptorelin, and MVT-602 in fertility medicine covering reproductive hormone regulation and clinical data. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Gonadorelin, HCG, HMG, MVT-602, Triptorelin. Key context: Gonadorelin (Synthetic GnRH used diagnostically and therapeutically for fertility including pulsatile GnRH the...); HCG (LH analog essential for triggering ovulation in assisted reproduction and supporting luteal phase...); HMG (Combined FSH and LH preparation used for ovarian stimulation in IVF and ovulation induction proto...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Synthetic GnRH used diagnostically and therapeutically for fertility including pulsatile GnRH the.... LH analog essential for triggering ovulation in assisted reproduction and supporting luteal phase.... Combined FSH and LH preparation used for ovarian stimulation in IVF and ovulation induction proto.... These takeaways are based on the research data available at the time of publication.
What is Gonadorelin and why is it significant?
Gonadorelin is a peptide discussed in this article because: Synthetic GnRH used diagnostically and therapeutically for fertility including pulsatile GnRH therapy for hypothalamic amenorrhea. For a complete profile of Gonadorelin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Reproductive Health Peptides: A Research Roundup
Peptides for reproductive health — kisspeptin, gonadorelin, HCG, HMG, triptorelin, and PT-141 — with evidence levels and clinical status.

Peptides for Men's Sexual Health: PT-141, Kisspeptin, and Emerging Options
Guide to peptides researched for male sexual health including PT-141, kisspeptin, gonadorelin, HCG, alprostadil, and oxytocin with evidence levels.

What Peptides Are FDA Approved? The Complete List (2026)
Complete list of FDA-approved peptide drugs with brand names, indications, and approval dates. Updated March 2026 with the RFK Jr. Category 1 reclassification of 14 peptides for compounding pharmacy access.
You Might Also Like
Related content you may find interesting