Peptide Interactions with Medications: What Your Doctor Needs to Know

Introduction#
As peptide therapy becomes more widespread, the question of how peptides interact with conventional medications becomes increasingly important. For healthcare professionals, understanding these interactions is essential for patient safety. For patients, knowing what to discuss with their provider can prevent adverse events and ensure optimal treatment outcomes.
This guide covers the most clinically relevant peptide-drug interactions, organized by peptide class. It distinguishes between interactions with strong clinical evidence (primarily for FDA-approved peptides) and theoretical interactions based on pharmacological mechanisms (for research-stage peptides where formal interaction studies have not been conducted).
For general peptide safety information, see the Peptide Safety Checklist and the Safety page.
GLP-1 Receptor Agonists: The Most-Studied Interaction Profile#
GLP-1 agonists including semaglutide, tirzepatide, and liraglutide have the most extensive drug interaction data of any peptide class, owing to their FDA-approved status and widespread use.
Delayed Gastric Emptying: The Central Mechanism#
The most important interaction mechanism for GLP-1 agonists is delayed gastric emptying. These peptides slow the rate at which food (and oral medications) move from the stomach into the small intestine, where most absorption occurs.
Clinical significance: This delay can alter the absorption profile of co-administered oral medications by:
- Delaying the time to peak concentration (Tmax)
- Potentially reducing the peak concentration (Cmax)
- Generally preserving total absorption (AUC) over time
The practical impact varies by medication, and formal pharmacokinetic studies have been conducted for several commonly co-prescribed drugs.
High-Priority Drug Interactions#
Oral Contraceptives#
Evidence level: Formal PK studies conducted
Semaglutide pharmacokinetic studies showed:
- Delayed Tmax for oral ethinyl estradiol and levonorgestrel by approximately 0.5-1 hour
- Overall bioavailability (AUC) was not significantly reduced
Clinical guidance: Current evidence suggests GLP-1 agonists do not meaningfully reduce oral contraceptive efficacy. However, during dose titration periods when gastric emptying effects may be most variable, some prescribers recommend backup contraception as a precaution.
Warfarin and Anticoagulants#
Evidence level: Formal PK studies and post-market monitoring
The semaglutide prescribing information notes:
- No clinically significant effect on warfarin pharmacokinetics in dedicated PK studies
- However, case reports of INR fluctuations in patients starting or titrating GLP-1 agonists exist
Clinical guidance: More frequent INR monitoring during GLP-1 initiation and dose changes is recommended. Reduced food intake on GLP-1 therapy (which decreases vitamin K consumption) may independently affect warfarin sensitivity.
Levothyroxine#
Evidence level: Clinical concern based on mechanism; limited formal PK data
Levothyroxine absorption is highly dependent on gastric pH and emptying time. Delayed gastric emptying could theoretically alter absorption kinetics.
Clinical guidance: Monitor TSH more frequently during GLP-1 initiation. Consider taking levothyroxine 30-60 minutes before the first meal on an empty stomach to minimize interaction potential. Some clinicians recommend separating levothyroxine dosing from GLP-1 injection timing by several hours.
Insulin and Sulfonylureas#
Evidence level: Strong clinical evidence from Phase 3 trials
This is the most clinically significant interaction for GLP-1 agonists. Adding a GLP-1 agonist to existing insulin or sulfonylurea therapy increases hypoglycemia risk substantially.
- STEP 2 trial (semaglutide in T2D): Hypoglycemia was more common in patients on concurrent sulfonylurea therapy
- SURMOUNT trials (tirzepatide): Insulin dose reductions of 20% were recommended at initiation in patients on basal insulin
Clinical guidance:
- Reduce insulin dose by 20% when initiating a GLP-1 agonist, then titrate based on glucose monitoring
- Consider reducing sulfonylurea dose proactively
- Increase glucose monitoring frequency during titration
Other Oral Medications#
| Medication | Interaction Concern | Evidence | Recommendation |
|---|---|---|---|
| Metformin | Delayed absorption | Formal PK study: minimal clinical impact | No adjustment typically needed |
| NSAIDs (ibuprofen, naproxen) | Delayed absorption | Limited formal data | May have delayed onset of action |
| Acetaminophen | Delayed Tmax | Used as PK probe in studies | Clinical significance minimal |
| Statins | Delayed absorption | Limited data | Monitor lipid levels on schedule |
| ACE inhibitors/ARBs | Delayed absorption | Limited data | Monitor blood pressure |
| SSRIs/SNRIs | Delayed absorption | Limited data | Monitor for symptom changes |
| Antibiotics (oral) | Delayed absorption | Theoretical concern | Consider timing separation for time-sensitive infections |
GLP-1 Agonist Interaction Summary for Prescribers#
Always check:
- Is the patient on insulin or sulfonylureas? (Reduce dose proactively)
- Is the patient on warfarin? (Increase INR monitoring)
- Is the patient on levothyroxine? (Monitor TSH, advise timing)
- Is the patient on oral contraceptives? (Reassure but consider backup during titration)
- Does the patient take narrow-therapeutic-index drugs? (Consider timing separation)
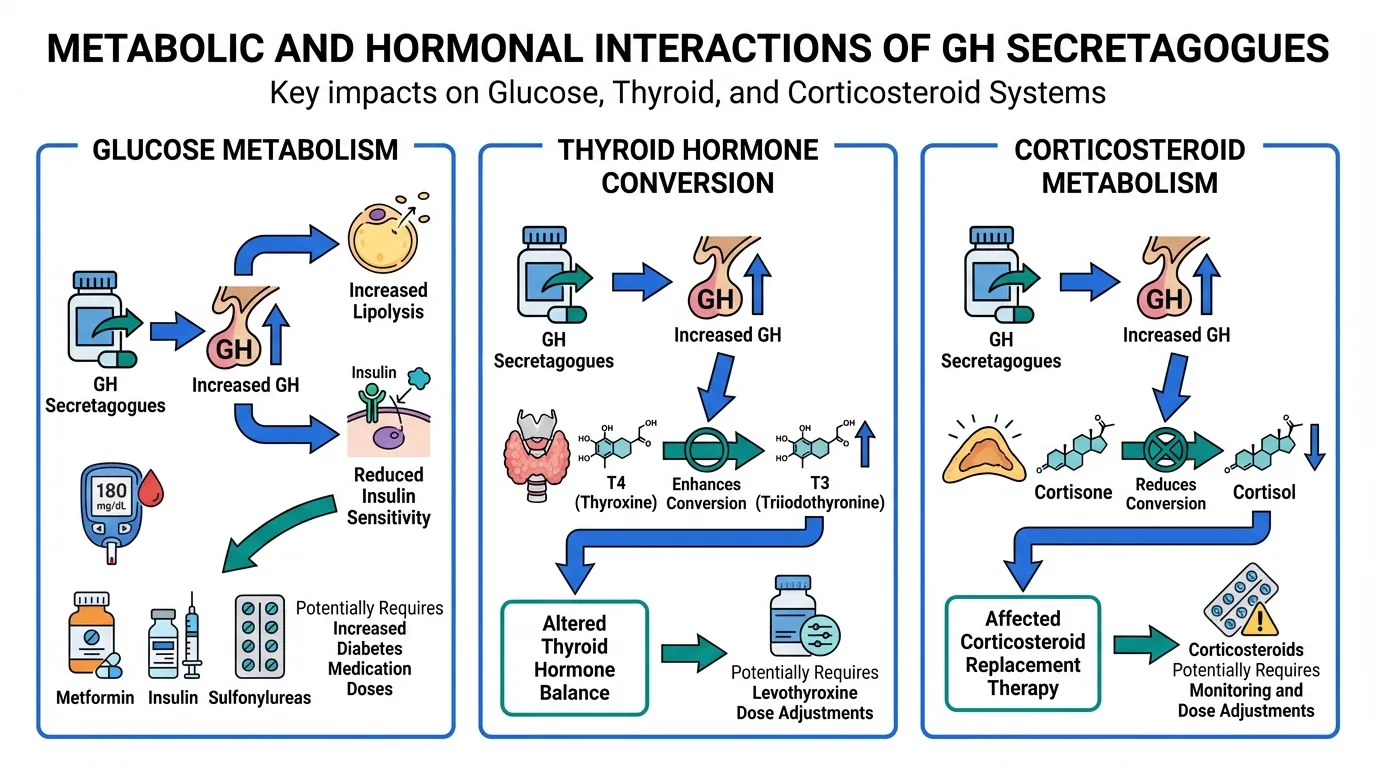
Growth Hormone Secretagogues: Metabolic and Hormonal Interactions#
GH secretagogues including ipamorelin, sermorelin, CJC-1295, and hexarelin raise growth hormone levels, which has downstream effects on multiple metabolic systems.
GH Peptides and Diabetes Medications#
Mechanism: Growth hormone is a counter-regulatory hormone to insulin. Elevated GH levels promote lipolysis and reduce insulin sensitivity. Chronically elevated GH (as occurs with sustained GH secretagogue use) can worsen insulin resistance.
Affected medications:
- Metformin -- May need dose increase to compensate for worsened insulin resistance
- Insulin -- May require dose adjustment; monitor fasting glucose closely
- Sulfonylureas -- Reduced efficacy possible; increased glucose monitoring needed
- SGLT2 inhibitors -- Additive effects on ketone production (theoretical; monitor in type 1 diabetes)
- GLP-1 agonists -- Opposing effects on glucose metabolism; clinical significance unclear for combination use
Monitoring recommendation: Fasting glucose, fasting insulin, and HbA1c at baseline and every 3 months when starting GH peptides in patients with diabetes or prediabetes.
GH Peptides and Thyroid Medications#
Mechanism: Growth hormone increases the conversion of T4 to T3 through enhanced peripheral deiodination. In patients on levothyroxine (T4 replacement), this can unmask or worsen central hypothyroidism or alter the T4/T3 balance.
Clinical significance: Patients on thyroid replacement who start GH peptides may experience:
- Apparent improvement in hypothyroid symptoms (due to increased T3 conversion)
- Changes in TSH, free T4, and free T3 levels
- Potential need for levothyroxine dose adjustment
Monitoring recommendation: Thyroid function panel (TSH, free T4, free T3) at baseline and 6-8 weeks after initiating GH peptides.
GH Peptides and Corticosteroids#
Mechanism: Growth hormone and cortisol have complex reciprocal interactions. GH can reduce the conversion of cortisone to cortisol (via 11-beta-HSD1), potentially reducing the effectiveness of replacement corticosteroids in patients with adrenal insufficiency.
Clinical significance: Patients on hydrocortisone or other corticosteroid replacement should be monitored for symptoms of adrenal insufficiency when starting GH-stimulating peptides.
GH Peptides and Anti-Cancer Therapies#
Theoretical concern: Since growth hormone promotes cell proliferation through the IGF-1 axis, there is a theoretical concern about GH secretagogues in patients with active cancer or a history of cancer.
Current evidence: The relationship between GH/IGF-1 levels and cancer risk is complex and not definitively resolved. However:
- Most oncologists advise against GH-stimulating therapy during active cancer treatment
- The risk profile in cancer survivors is debated
- This represents a contraindication rather than a drug interaction per se
Guidance: GH secretagogue use should be discussed with an oncologist for any patient with a cancer history.
Immune-Modulating Peptides: Immunosuppressant Interactions#
Immune peptides including thymosin alpha-1, KPV, LL-37, and VIP present unique interaction concerns related to their immune-modulating activity.
Thymosin Alpha-1 and Immunosuppressants#
Mechanism: Thymosin alpha-1 enhances T-cell function, dendritic cell maturation, and Th1/Th2 balance. This immune-stimulating activity directly opposes the mechanisms of immunosuppressive drugs.
High-risk interactions:
| Immunosuppressant | Interaction Concern | Risk Level |
|---|---|---|
| Cyclosporine | Thymosin alpha-1 may counteract T-cell suppression | High |
| Tacrolimus | Same mechanism as cyclosporine | High |
| Mycophenolate | Opposing effects on lymphocyte function | Moderate-High |
| Azathioprine | Opposing effects on immune cell proliferation | Moderate |
| Prednisone (high-dose) | Partially opposing immunomodulation | Moderate |
Clinical guidance: Thymosin alpha-1 should generally not be combined with immunosuppressive therapy used for organ transplant rejection prevention or severe autoimmune disease without specialist supervision. The risk of graft rejection or autoimmune flare is significant.
Immune Peptides and Autoimmune Disease Medications#
For patients with autoimmune conditions, immune-stimulating peptides carry the risk of exacerbating disease activity:
- Biologics (TNF inhibitors, IL-6 blockers): Immune peptides may partially counteract their immunosuppressive effects
- DMARDs (methotrexate, hydroxychloroquine): Immune stimulation could increase autoimmune activity despite DMARD therapy
- JAK inhibitors: Potential for complex immune pathway interactions
Paradox with KPV and VIP: Unlike thymosin alpha-1, KPV and VIP have anti-inflammatory rather than immune-stimulating properties. These may theoretically be less problematic with immunosuppressants, but no formal human interaction studies exist.
Healing Peptides: The Information Gap#
BPC-157 Interaction Concerns#
BPC-157 has no formal human drug interaction studies. All interaction concerns are theoretical, based on its known preclinical mechanisms:
Angiogenesis promotion:
- BPC-157 promotes blood vessel formation through VEGF upregulation in animal models
- Theoretical concern with anti-angiogenic cancer therapies (bevacizumab, ramucirumab)
- Theoretical concern with bleeding risk when combined with anticoagulants (warfarin, DOACs)
Nitric oxide pathway modulation:
- BPC-157 modulates the NO system in preclinical models
- Theoretical interactions with nitrate medications (nitroglycerin, isosorbide)
- Theoretical interactions with PDE5 inhibitors (sildenafil, tadalafil) -- both affect NO-mediated vasodilation
- Theoretical interaction with blood pressure medications
Dopamine system effects:
- Animal studies suggest BPC-157 modulates dopaminergic pathways
- Theoretical interactions with dopamine agonists/antagonists (levodopa, antipsychotics)
Critical caveat: None of these interactions have been confirmed in humans. However, the absence of data is not evidence of safety. Patients using BPC-157 alongside any of these medication classes should inform their healthcare provider.
TB-500 (Thymosin Beta-4)#
TB-500, like BPC-157, promotes angiogenesis and tissue remodeling in preclinical models. The same theoretical concerns regarding anticoagulants and anti-angiogenic therapies apply.
What We Do Not Know: The Information Gap#
For most peptides outside the FDA-approved category, formal drug interaction studies have not been conducted. This creates a significant knowledge gap.
Why Formal Interaction Data Is Missing#
- Cost: Pharmacokinetic drug interaction studies cost millions of dollars
- Regulatory incentive: Only FDA-approved drugs require formal interaction studies
- Preclinical focus: Most peptide research focuses on efficacy mechanisms, not drug-drug interactions
- Ethical barriers: It is difficult to design ethical studies combining unapproved peptides with patient medications
What This Means for Patients and Providers#
When no formal interaction data exists:
- Assume interactions are possible until evidence suggests otherwise
- Use pharmacological reasoning -- if a peptide's mechanism overlaps with a medication's target, an interaction is plausible
- Monitor actively -- more frequent lab work and symptom assessment during combined use
- Report adverse events -- case reports and adverse event data gradually build the interaction knowledge base
- Default to caution -- when in doubt, consult with a pharmacist or clinical pharmacologist
Questions for Patients to Discuss with Their Prescriber#
When bringing up peptide use with your healthcare provider, prepare to discuss:
-
"I am using [specific peptide] at [dose] and [frequency]. Can you help me evaluate potential interactions with my current medications?"
-
"My current medications include [list all]. Are there any mechanisms that might conflict with this peptide?"
-
"What lab work should we monitor more frequently given that I am using this peptide?"
-
"Are there any medications I should take at a different time of day to minimize interaction risk?"
-
"What symptoms should prompt me to stop the peptide and contact you?"
-
"I understand this peptide does not have formal interaction studies. What is the most conservative approach to combined use?"
If your provider is unfamiliar with a specific peptide: Offer to share the peptide's profile page from this site, which includes mechanism of action, known side effects, and research status. Most providers appreciate patients who bring organized information.
Quick Reference: Common Medication Classes and Peptide Interactions#
| Medication Class | GLP-1 Agonists | GH Secretagogues | Immune Peptides | Healing Peptides |
|---|---|---|---|---|
| Insulin | Hypoglycemia risk (reduce dose) | May worsen insulin resistance | No known interaction | No known interaction |
| Sulfonylureas | Hypoglycemia risk | May reduce efficacy | No known interaction | No known interaction |
| Metformin | Delayed absorption (minimal impact) | May need dose increase | No known interaction | No known interaction |
| Warfarin | Monitor INR more frequently | No established interaction | No known interaction | Theoretical bleeding risk (angiogenesis) |
| Levothyroxine | Monitor TSH, timing separation | May alter T4/T3 conversion | No known interaction | No known interaction |
| Oral contraceptives | Delayed absorption (likely minimal impact) | No established interaction | No known interaction | No known interaction |
| Immunosuppressants | No known interaction | No known interaction | May counteract effect (high risk) | No known interaction |
| Antihypertensives | No established interaction | No established interaction | No known interaction | Theoretical NO pathway overlap |
| Antipsychotics | No established interaction | No established interaction | No known interaction | Theoretical dopamine interaction (BPC-157) |
| NSAIDs | Delayed absorption | No established interaction | No known interaction | No known interaction |
"No known interaction" = no formal interaction data exists, not that interactions are impossible.
Key Takeaways#
-
GLP-1 agonists have the most documented interactions -- primarily through delayed gastric emptying affecting oral medication absorption, and through enhanced hypoglycemia risk with insulin and sulfonylureas. See our GLP-1 side effects comparison for a deeper look at GLP-1 tolerability.
-
GH secretagogues interact with metabolic medications -- their anti-insulin effects can worsen glucose control, and they can alter thyroid hormone conversion and corticosteroid metabolism.
-
Immune peptides can conflict with immunosuppressants -- thymosin alpha-1 and other immune-stimulating peptides may counteract drugs used to prevent transplant rejection or control autoimmune diseases.
-
Most research peptides lack formal interaction data -- the absence of studies does not mean interactions do not exist. Use pharmacological reasoning and monitor actively. For guidance on combining peptides safely, see the science of peptide stacking.
-
Always disclose peptide use to your healthcare provider -- even for research compounds, your provider needs complete information to prescribe safely and interpret lab results correctly.
-
Timing matters -- for oral medications taken with GLP-1 agonists, strategic timing separation can minimize absorption concerns. Discuss specific timing with your pharmacist.
This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Drug interactions are complex and individual. The information provided here is a general reference and may not cover all possible interactions. Always consult a qualified healthcare provider or clinical pharmacist for interaction screening specific to your medication regimen. For comprehensive safety information, see the Safety page and the Peptide Safety Guide.

{kind=link}
Frequently Asked Questions About Peptide Interactions with Medications: What Your Doctor Needs to Know
Does semaglutide interact with other medications?
Yes. Semaglutide slows gastric emptying, which can delay the absorption of oral medications taken at the same time. This is particularly relevant for medications with narrow therapeutic windows such as warfarin, levothyroxine, and some antibiotics. While clinical studies show these effects are generally modest, patients on multiple oral medications should discuss timing strategies with their prescriber. Semaglutide may also enhance the glucose-lowering effects of insulin and sulfonylureas, increasing hypoglycemia risk.
Can I take BPC-157 with my current medications?
There are no formal human drug interaction studies for BPC-157. The peptide has only been studied in animal models, so interactions with human medications are theoretical. Based on its known mechanisms (angiogenesis promotion, nitric oxide modulation), theoretical concerns include interactions with blood thinners, blood pressure medications, and drugs affecting the NO pathway. Consult your healthcare provider and disclose all supplements and research compounds you are using.
Should I tell my doctor about peptides I am using?
Yes, always. Even if your provider is unfamiliar with a specific peptide, they need to know about all substances you are using to monitor for interactions, interpret lab results correctly, and provide appropriate care. Bring the peptide name, dose, frequency, and source to your appointment. This information is protected by patient confidentiality.
Do growth hormone peptides interact with diabetes medications?
Yes. Growth hormone has well-established anti-insulin effects. GH secretagogues like ipamorelin that elevate growth hormone levels may worsen insulin resistance and counteract the effects of diabetes medications including metformin, insulin, and sulfonylureas. Patients with diabetes or prediabetes who use GH peptides should monitor fasting glucose and HbA1c closely and may need medication adjustments.
Are there peptides that should never be combined with certain drugs?
The strongest evidence for problematic interactions involves GLP-1 agonists with insulin or sulfonylureas (hypoglycemia risk requiring dose reduction). Immune-stimulating peptides like thymosin alpha-1 should not be combined with immunosuppressants used for organ transplant rejection prevention without specialist oversight. For most research peptides, the honest answer is that formal interaction studies have not been conducted, making definitive guidance impossible.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Core Peptides Review 2026: COAs, Finnrick Controversy, and Whether the Score Holds Up
An honest 2026 review of Core Peptides covering product range, payment flexibility, shipping, COA transparency, and how the Finnrick Analytics controversy should change how you read vendor ratings. Includes 8-dimension scoring.
Understanding Peptide Side Effects: A Comprehensive Safety Guide
A thorough, evidence-based guide to peptide side effects by category — covering GLP-1 agonists, GH secretagogues, tissue repair peptides, and melanocortins — with serious risk flags, drug interactions, monitoring recommendations, and guidance on when to stop.
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.
You Might Also Like
Related content you may find interesting