The Science of Peptide Stacking: Synergies, Risks, and Evidence

Introduction#
"Peptide stacking" has become one of the most discussed topics in the peptide research community. The premise is intuitive: if one peptide helps with recovery, and another helps with growth hormone, using both should be better than either alone. But how much of this reasoning is supported by actual evidence, and how much is extrapolation?
This article examines the science behind peptide combinations -- from well-documented receptor-level synergies to theoretical stacks with no direct combination data. It categorizes stacking approaches by their evidence quality, explains the molecular mechanisms that underlie genuine synergies, identifies combinations with potential risks, and addresses the fundamental challenge of drawing conclusions from N=1 community protocols.
For a practical introduction to peptide combinations, see Complete Guide to Peptide Stacks. To check compatibility between specific peptides, use the Stack Compatibility Checker.
What "Stacking" Actually Means#
The term "stacking" in the peptide context refers to the concurrent use of two or more peptides targeting different biological pathways or receptors. The underlying assumption is that non-overlapping mechanisms will produce complementary or synergistic outcomes.
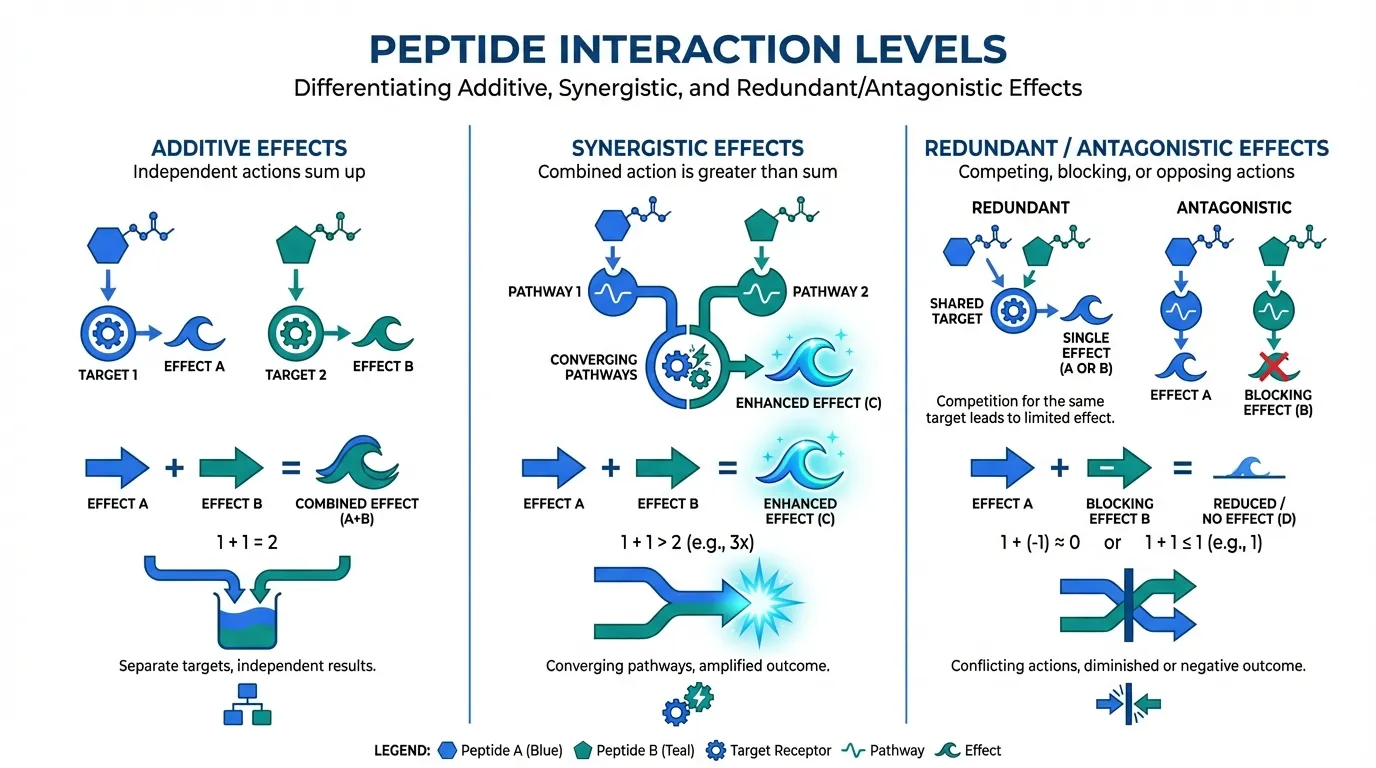
However, not all combinations qualify as true synergies. It is important to distinguish between three levels of interaction:
Additive Effects#
Two peptides produce independent effects that simply add together. Each contributes its own benefit without influencing the other's activity. Example: using a healing peptide for an injury while simultaneously using a sleep peptide for recovery -- the two targets do not interact mechanistically.
Synergistic Effects#
Two peptides interact at the molecular level to produce an outcome greater than the sum of their individual effects. The combined response exceeds what mathematical addition of individual effects would predict. Example: GHRH + GHRP combinations for GH release, where co-activation of both receptor pathways produces supra-additive GH output.
Redundant or Antagonistic Effects#
Two peptides target the same receptor or pathway, either competing for binding sites (redundant) or producing opposing downstream effects (antagonistic). Example: combining two ghrelin-receptor agonists like ipamorelin and GHRP-2, which compete for the same GHS-R1a receptor without meaningful synergy.
Evidence-Based Stacks: What the Research Supports#
Tier 1: GHRH + GHRP Combination (Strong Evidence)#
The most well-documented peptide synergy in the literature is the combination of a GHRH-pathway peptide with a ghrelin-pathway peptide for growth hormone release. This is not merely theoretical -- it has been demonstrated in controlled clinical studies.
The mechanism: GHRH-receptor activation (via sermorelin, CJC-1295, or tesamorelin) signals through the cAMP/PKA pathway in pituitary somatotrophs, driving GH synthesis and priming cells for release. GHS-R1a activation (via ipamorelin, GHRP-2, or hexarelin) signals through the PLC/IP3/PKC pathway, amplifying the release signal. When both pathways are activated simultaneously, the converging intracellular signals produce GH output that significantly exceeds the additive prediction.
Published evidence: Multiple clinical studies have administered GHRH analogs together with ghrelin-receptor agonists and measured the GH response. The consistent finding is supra-additive GH release -- the combination produces 2-3x more GH than the mathematical sum of individual responses would predict.
Most studied pairing: CJC-1295 (No DAC) + ipamorelin. This specific combination leverages CJC-1295's improved enzymatic resistance (vs. sermorelin) and ipamorelin's selectivity (vs. GHRP-2 or hexarelin). See CJC-1295 and Ipamorelin Stack for a detailed analysis.
Evidence grade: A -- Receptor-level mechanism confirmed. Synergy demonstrated in human studies. Well-characterized safety profiles for individual components.
Tier 2: BPC-157 + TB-500 Healing Stack (Moderate Preclinical Evidence)#
The combination of BPC-157 and TB-500 (often called the "Wolverine Stack") is the most discussed healing peptide combination. The rationale is based on complementary, non-overlapping mechanisms rather than demonstrated synergy.
BPC-157 mechanisms:
- Promotes angiogenesis through VEGF upregulation
- Modulates nitric oxide (NO) signaling pathways
- Demonstrates cytoprotective effects across multiple tissue types
- Activates the FAK-paxillin pathway involved in cell migration and adhesion
TB-500 (thymosin beta-4) mechanisms:
- Regulates actin polymerization, facilitating cell motility
- Promotes cell migration to injury sites
- Anti-inflammatory effects through reduction of pro-inflammatory cytokines
- Modulates extracellular matrix remodeling
Why the combination is plausible: BPC-157 creates the vascular infrastructure for tissue repair (new blood vessels, cytoprotection) while TB-500 facilitates the cellular migration and anti-inflammatory environment needed for tissue remodeling. These are sequential and complementary processes in wound healing.
What is missing: No published studies have evaluated BPC-157 and TB-500 in combination. The synergy hypothesis is based entirely on the non-overlapping nature of their individual mechanisms. Furthermore, BPC-157 itself lacks published human clinical trial data, meaning one half of this "evidence-based" stack has no human evidence at all.
Evidence grade: C+ -- Individual mechanisms well-characterized (mostly preclinical). Complementary mechanism rationale is sound. No combination studies exist. No human clinical trial data for BPC-157.
For a detailed analysis, see BPC-157 and TB-500 Blend and BPC-157 vs TB-500.
Tier 3: Selank + Semax Nootropic Stack (Limited Evidence)#
The combination of selank and semax is discussed in nootropic communities based on their different mechanisms of cognitive enhancement.
Selank: A synthetic analog of the immunomodulatory peptide tuftsin. Acts primarily through GABA and serotonin system modulation, with anxiolytic effects being its most characterized property. Also influences BDNF expression.
Semax: A synthetic analog of ACTH(4-10). Acts primarily through BDNF and NGF upregulation, with cognitive enhancement and neuroprotective effects being its primary research focus. Also modulates dopaminergic and serotonergic systems.
Combination rationale: Selank provides anxiolytic and mood-stabilizing effects through GABAergic modulation, while semax provides cognitive activation through neurotrophin upregulation. The non-overlapping primary mechanisms suggest complementary effects -- stress reduction from selank paired with cognitive enhancement from semax.
What is missing: No combination studies exist. Both compounds have been studied individually in Russian clinical trials with reported cognitive and anxiolytic benefits, but the quality and accessibility of these studies varies. The combination rationale is entirely mechanistic.
Evidence grade: C -- Individual effects supported by limited clinical data. Non-overlapping mechanisms provide rationale. No combination data. See Selank vs Semax for the individual comparison.
Theoretical Stacks: Plausible but Unproven#
The following combinations are discussed in the peptide community based on mechanistic reasoning. While the rationale may be sound, no published research has evaluated these specific combinations. They represent hypothesis-level stacking, not evidence-based practice.
Multi-System Recovery Stack#
Proposed combination: BPC-157 + GH secretagogue (e.g., ipamorelin or CJC-1295 + ipamorelin)
Rationale: BPC-157 addresses local tissue repair while GH secretagogues support systemic recovery through enhanced growth hormone, which drives IGF-1 production, protein synthesis, and collagen formation. The mechanisms are entirely non-overlapping -- BPC-157 acts locally on tissue while GH secretagogues act centrally on the pituitary.
Unknown factors: How locally-administered BPC-157 interacts with systemically elevated GH/IGF-1 levels. Whether the combination alters the safety profile of either component. Whether timing matters for the interaction.
Evidence grade: D -- Sound mechanistic rationale. No combination data. One component (BPC-157) lacks human clinical trial data.
Immune Modulation Stack#
Proposed combination: KPV + thymosin alpha-1 or GHK-Cu
Rationale: KPV is an anti-inflammatory tripeptide (derived from alpha-MSH) that reduces NF-kB signaling. Thymosin alpha-1 modulates T-cell function and immune surveillance. GHK-Cu has anti-inflammatory gene expression effects. Combining anti-inflammatory and immunomodulatory peptides could theoretically support balanced immune function.
Unknown factors: Immunological cross-talk between anti-inflammatory and immunostimulatory peptides is complex. The interplay between NF-kB suppression (KPV) and T-cell activation (thymosin alpha-1) could have unpredictable results depending on the underlying immune state.
Evidence grade: D -- Mechanistically plausible. Complex immune interplay raises safety questions. No combination data.
Anti-Aging Multi-Target Stack#
Proposed combination: GHK-Cu + epitalon + GH secretagogue
Rationale: Each component targets a different hallmark of aging -- GHK-Cu addresses gene expression and tissue remodeling, epitalon targets telomere maintenance via telomerase activation, and GH secretagogues address somatopause (age-related GH decline). Non-overlapping targets suggest additive rather than synergistic effects.
Unknown factors: Long-term safety of simultaneously modulating multiple aging pathways. Whether telomerase activation and GH elevation in combination create unanticipated risks (both have theoretical implications for cell proliferation).
Evidence grade: D -- Multi-target rationale. Individual evidence varies (GH secretagogues: clinical; epitalon: limited clinical; GHK-Cu: moderate clinical). No combination data.
Contraindicated and Risky Combinations#
Same-Receptor Redundancy#
Combining multiple peptides that target the same receptor is generally counterproductive:
| Redundant Combination | Why It Is Problematic |
|---|---|
| Ipamorelin + GHRP-2 | Both compete for GHS-R1a binding. The less selective peptide (GHRP-2) adds side effects without meaningful synergy. |
| Ipamorelin + MK-677 | Same receptor target. MK-677's 24-hour half-life means sustained occupancy that leaves little room for ipamorelin to add benefit. |
| Sermorelin + CJC-1295 (No DAC) | Both target GHRH-R. Using both is redundant since CJC-1295 is essentially an improved sermorelin. |
| GHRP-2 + GHRP-6 + hexarelin | All three compete for GHS-R1a. Stacking ghrelin agonists compounds cortisol and prolactin effects without proportional GH benefit. |
Cumulative Side Effect Risk#
Combinations where individual side effects may compound:
| Combination Risk | Concern |
|---|---|
| Multiple GH-elevating agents | Cumulative GH/IGF-1 elevation increases risk of insulin resistance, joint issues, water retention. More is not always better. |
| Multiple appetite-stimulating compounds | GHRP-6 + MK-677 would produce severe appetite stimulation from dual ghrelin-receptor activation. |
| Immune stimulation + immunosuppressants | Combining thymosin alpha-1 (immune activator) with prescribed immunosuppressive therapy could create dangerous immune dysregulation. |
| Multiple cortisol-elevating peptides | GHRP-2 + hexarelin compounds cortisol elevation, potentially undermining recovery goals. |
Unknown Interaction Risks#
For the vast majority of peptide combinations, no safety data exists for the specific pairing. This is the most important risk factor in peptide stacking: the absence of evidence is not evidence of safety. Each additional compound in a stack multiplies the number of potential interactions without corresponding safety data.
The N=1 Problem: Community Protocols and Scientific Rigor#
Why Community Reports Are Insufficient#
The peptide community frequently shares "what works for me" reports involving multi-peptide stacks. While these reports provide anecdotal data points, they cannot establish causation, synergy, or safety for several reasons:
- No controls: Without a control group (or at minimum, a period using each peptide individually), there is no way to attribute effects to the combination rather than individual components
- Confirmation bias: People who invest time and money in a multi-peptide protocol are psychologically motivated to perceive positive results
- Confounding variables: Changes in training, diet, sleep, stress, and other supplements make it impossible to isolate peptide effects
- Survivorship bias: People who experience negative effects or no effects are less likely to post about their experience
- Dosing variability: Peptide sourcing, purity, reconstitution accuracy, and injection technique vary dramatically between individuals
What Community Data Can Tell Us#
Despite these limitations, large-scale community reporting can provide useful signal:
- Safety red flags: If multiple independent users report similar adverse effects from a combination, this warrants attention even without controlled data
- Plausibility confirmation: If users consistently report effects consistent with the predicted mechanism, it strengthens (but does not prove) the hypothesis
- Protocol refinement: Community experience can identify practical considerations (timing, dosing, cycling) that may not emerge from the limited clinical data available
How to Evaluate Stack Claims#
When evaluating claims about peptide stacking, apply this framework:
- Does a documented receptor-level synergy exist? (Only true for GHRH + GHRP combinations)
- Are the individual mechanisms well-characterized? (BPC-157, GH peptides: yes. Many others: partially)
- Do the mechanisms actually complement each other, or just not conflict? (Non-conflicting is not the same as synergistic)
- Has the specific combination been studied? (Almost always: no)
- Are there theoretical safety concerns from combining these mechanisms? (Consider cumulative receptor activation, opposing immune effects, metabolic interactions)
Timing and Administration Considerations#
Even when the scientific rationale for a combination is sound, practical implementation introduces additional variables.
Timing Interactions#
- GHRH + GHRP: Should be administered simultaneously for synergistic effect, as the synergy depends on concurrent receptor activation
- BPC-157 + TB-500: No established timing relationship. Some community protocols administer them at different times of day, but no data supports one timing over another
- GH secretagogues: Typically administered on an empty stomach, as food (particularly fats and carbohydrates) can blunt the GH response
- Sleep peptides (DSIP) + GH secretagogues: Evening co-administration is logical since both target the sleep-associated recovery window
Injection Site Considerations#
- Different peptides administered at the same time should generally use different injection sites
- Local-acting peptides (BPC-157 for a specific injury) may require administration near the target tissue
- Systemic peptides (GH secretagogues) can be administered at any subcutaneous site
Evidence Quality Summary#
| Stack | Synergy Type | Evidence Grade | Combination Data | Notes |
|---|---|---|---|---|
| CJC-1295 + Ipamorelin | Receptor-level synergy | A | Yes (GHRH+GHRP studies) | Best-documented peptide synergy |
| GHRH analog + any GHRP | Receptor-level synergy | A | Yes (multiple studies) | Class-wide effect, not compound-specific |
| BPC-157 + TB-500 | Complementary mechanisms | C+ | No | Sound rationale, no combination data |
| Selank + Semax | Complementary mechanisms | C | No | Limited individual clinical data |
| BPC-157 + GH secretagogue | Non-overlapping targets | D | No | BPC-157 lacks human trials |
| KPV + Thymosin Alpha-1 | Complementary immune targets | D | No | Complex immune interplay concerns |
| Multi-peptide anti-aging | Multi-target additive | D | No | Unknown long-term safety of combined effects |
| Same-receptor stacking | Redundant | N/A | N/A | Counterproductive; avoid |
Key Takeaways#
- The only well-documented peptide synergy with clinical evidence is the GHRH + GHRP combination for growth hormone release, where simultaneous activation of both receptor pathways produces supra-additive GH output
- The BPC-157 + TB-500 ("Wolverine Stack") combination has plausible mechanistic rationale based on complementary healing pathways, but no published combination studies exist
- Most popular peptide stacks lack direct combination research. Their rationale is based on non-overlapping individual mechanisms, which provides plausibility but not proof of synergy
- Combining peptides that target the same receptor (e.g., multiple ghrelin agonists) is redundant and typically compounds side effects without proportional benefit
- Unknown interactions represent the primary risk in peptide stacking. Each additional compound multiplies potential interactions without corresponding safety data
- Community protocol reports provide anecdotal signal but cannot establish synergy, causation, or safety due to lack of controls, confounding variables, and reporting biases
- A conservative evidence-based approach limits stacking to combinations where individual safety profiles are well-characterized, mechanisms are clearly non-overlapping, and the number of concurrent compounds is minimized
- The gap between what the research supports and what the community practices is substantial -- bridging this gap requires more combination studies, not more anecdotal reports
This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. The peptides discussed are investigational compounds and should only be used under appropriate medical supervision. The absence of combination safety data means that multi-peptide protocols carry unknown risks. Always consult a qualified healthcare provider before making decisions about peptide therapy.
Related Resources#

{kind=link}
Frequently Asked Questions About The Science of Peptide Stacking: Synergies, Risks, and Evidence
What does peptide stacking mean?
Peptide stacking refers to the concurrent use of two or more peptides with the goal of achieving synergistic or complementary effects. The term originates from the idea that certain peptides target different receptors or biological pathways, so combining them may produce outcomes greater than either alone. The concept ranges from well-documented receptor-level synergies (like GHRH + GHRP for growth hormone release) to entirely theoretical combinations based on non-overlapping mechanisms without direct combination studies.
Is there scientific evidence for peptide stacking?
The evidence varies dramatically by combination. The GHRH + GHRP synergy for growth hormone release is well-documented in clinical studies showing that simultaneous activation of both pathways produces GH output significantly greater than the sum of individual effects. However, most other popular stacks (BPC-157 + TB-500, selank + semax, multi-peptide healing protocols) lack direct combination studies. Their rationale is based on complementary individual mechanisms rather than proven synergy.
Are there dangerous peptide combinations to avoid?
Certain combinations carry theoretical risks. Stacking multiple ghrelin-receptor agonists (e.g., ipamorelin + GHRP-2 + MK-677) is redundant and may compound side effects without additional benefit. Combining immune-stimulating peptides with immunosuppressive therapies could create unpredictable interactions. Any combination involving peptides that affect blood pressure, blood glucose, or coagulation requires careful consideration of cumulative effects. The lack of combination safety data for most peptide pairings means unknown risks exist.
What is the most scientifically supported peptide stack?
The CJC-1295 (No DAC) + ipamorelin combination is the most scientifically supported peptide stack. The synergistic mechanism is well-characterized at the receptor level, with GHRH-receptor and GHS-R1a activation producing synergistic GH release through converging but distinct intracellular signaling cascades (cAMP/PKA and PLC/IP3/PKC pathways respectively). Multiple studies on GHRH + GHRP combinations confirm the synergy principle.
How many peptides can you safely stack at once?
There is no established safe maximum. The peptide community commonly discusses protocols involving 2-4 concurrent peptides, but no clinical trials have evaluated multi-peptide combinations beyond dual GHRH + GHRP protocols. Each additional compound introduces potential for unknown interactions, compounding side effects, and increased complexity. A conservative evidence-based approach would limit stacking to combinations where at least the individual safety profiles are well-characterized and the mechanisms do not overlap in ways that could amplify adverse effects.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.
You Might Also Like
Related content you may find interesting