BPC-157 vs TB-500: Comprehensive Comparison of Healing Peptides
A detailed comparison of BPC-157 and TB-500 (Thymosin Beta-4) covering mechanisms, research evidence, dosing, and side effects for tissue repair.
Verdict at a Glance
BPC-157 and TB-500 target tissue repair through distinct but complementary mechanisms. BPC-157 has a stronger preclinical profile for gastrointestinal and musculoskeletal healing, while TB-500 has more advanced clinical trial data, particularly for ophthalmic and dermal wound applications. Neither peptide is approved for human therapeutic use. Their combination (the "Wolverine Stack") lacks controlled combination studies.
| Best for | Pick | Why |
|---|---|---|
| Gastrointestinal Healing Research | BPC-157 | BPC-157 is derived from gastric juice and has the strongest preclinical evidence for GI protection, colitis healing, fistula closure, and anastomosis repair across numerous animal models. |
| Tendon and Ligament Injury Research | BPC-157 | Extensive preclinical evidence in MCL transection, Achilles tendon, and other musculoskeletal models with consistent improvements in biomechanical properties and functional recovery. |
| Wound Healing and Dermal Repair | TB-500 | TB-500 has Phase II clinical data for venous stasis and pressure ulcers showing healing acceleration. Its keratinocyte migration activity (2-3 fold increase) and anti-scarring properties are well characterized. |
| Corneal and Ophthalmic Applications | TB-500 | RGN-259 (0.1% Thymosin Beta-4) advanced through Phase III trials for neurotrophic keratopathy with 35.1% reduction in ocular discomfort and 59.1% reduction in corneal staining versus placebo. |
| Cardiac Protection Research | TB-500 | Tβ4 demonstrated ILK-Akt-mediated cardiomyocyte survival in Nature (2004) and can reactivate epicardial progenitor cells, though large animal translation has been inconsistent. |
| Combined Healing Protocol Research | Both (Wolverine Stack) | The distinct mechanisms (BPC-157 via VEGF/NO angiogenesis, TB-500 via actin-mediated cell migration) provide a theoretical rationale for combination, though no controlled combination studies exist. |
| Category | BPC-157 | TB-500 | Advantage |
|---|---|---|---|
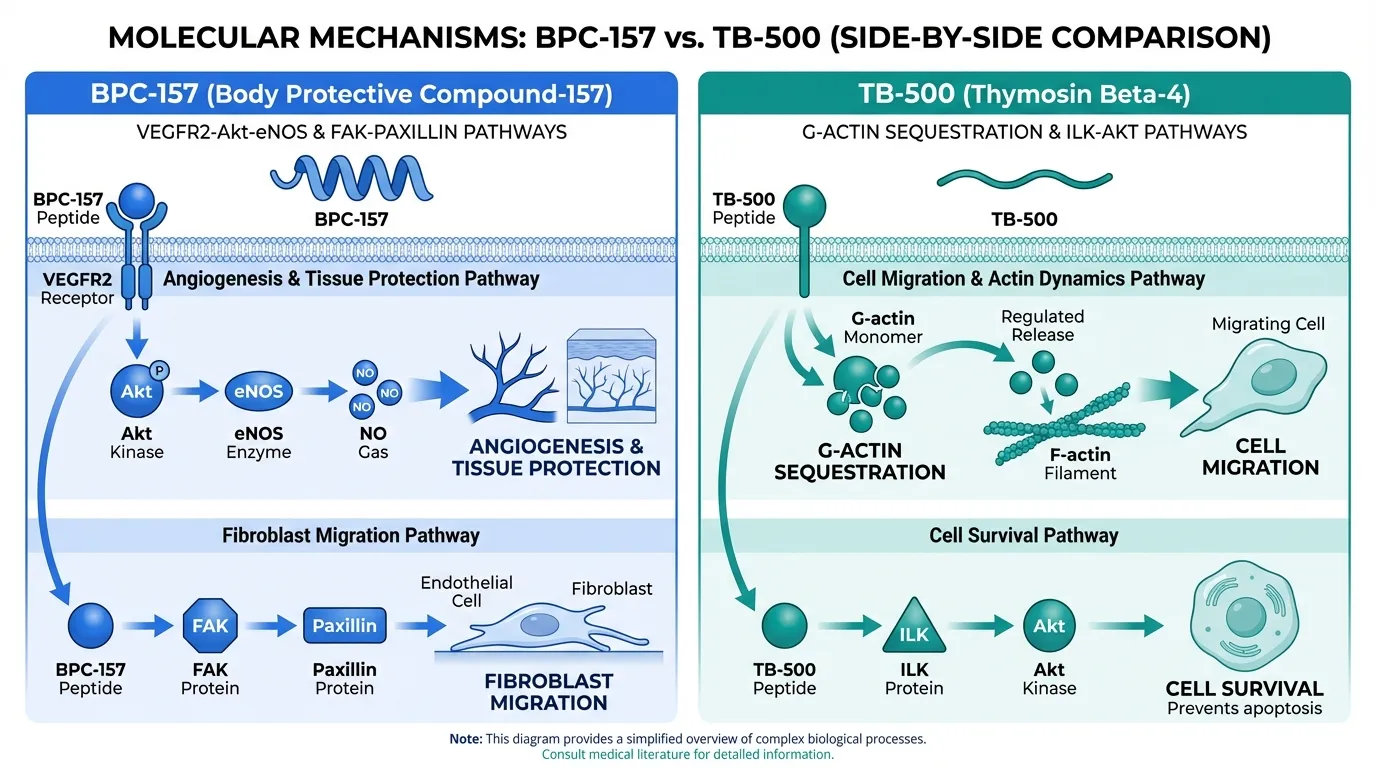
| Mechanism of Action | Acts through VEGFR2-Akt-eNOS signaling, Src-Caveolin-1-eNOS vasomotor modulation, and FAK-paxillin migration pathways. Promotes angiogenesis, normalizes NO levels, and stabilizes endothelial/epithelial barriers. | Functions primarily through G-actin sequestration, regulating cytoskeletal dynamics and cell migration. Activates integrin-linked kinase (ILK) and Akt survival signaling. Inhibits NF-kB-mediated inflammation. | Comparable |
| Research Evidence | Extensive preclinical evidence (100+ animal studies) across GI, tendon, ligament, muscle, CNS, and ocular models. Limited human data from small Phase I and a 53-patient UC enema trial. Most studies from a small number of research groups. | Strong preclinical evidence across wound healing, cardiac, corneal, and stroke models. Two Phase I human safety studies (Western and Chinese populations). Phase II/III clinical trials for ophthalmic indications with RGN-259 formulation. | TB-500 |
| Side Effect Profile | Generally well tolerated in animal studies. No adverse events reported in small human studies (0/2 IV, 0/12 intravesical, 0/16 intra-articular). LD50 >2000 mg/kg in mice. Theoretical concerns about angiogenesis and NO-pathway modulation. | Well tolerated in Phase I trials at IV doses up to 1260 mg with no dose-limiting toxicities. Mild side effects include injection site reactions, headache, and nausea. Theoretical concern about tumor angiogenesis due to pro-migratory properties. | Comparable |
| Dosing Complexity | Typically dosed at 200-500 mcg subcutaneously 1-2 times daily. Can be injected near injury site for localized effect. Also studied orally due to gastric juice stability. Reconstitution from 5 mg vials is standard. | Research protocols commonly reference 2-5 mg subcutaneously 2-3 times per week during loading, then weekly maintenance. Clinical trials used IV doses of 42-1260 mg and topical 0.03-0.1% formulations. | BPC-157 |
| Clinical Applications | Studied for GI protection and healing, tendon/ligament repair, muscle healing, spinal cord injury, ocular protection, and wound healing. Strongest preclinical signal in GI and musculoskeletal indications. | Studied for dermal wound healing, corneal repair (Phase II/III trials), cardiac protection after MI, stroke recovery, and anti-fibrotic applications. Strongest signal in ophthalmic and wound healing. | Comparable |

Introduction#
BPC-157 and TB-500 are the two most widely discussed healing peptides in regenerative research, and their combination -- commonly known as the "Wolverine Stack" -- has generated significant interest among researchers studying tissue repair. While both peptides promote healing, they do so through fundamentally different molecular mechanisms, making their comparison both scientifically interesting and practically relevant.
BPC-157 (Body Protection Compound-157) is a synthetic 15-amino-acid peptide derived from a protective protein found in human gastric juice. It acts primarily through the VEGFR2-Akt-eNOS signaling axis to promote angiogenesis, normalize nitric oxide levels, and stabilize tissue barriers. TB-500, on the other hand, is a synthetic version of Thymosin Beta-4, a naturally occurring 43-amino-acid peptide that functions as the principal G-actin sequestering protein in mammalian cells. It promotes healing through cytoskeletal regulation, cell migration, and ILK-Akt survival signaling.
This comparison examines the evidence base for each peptide across mechanisms, dosing, side effects, and clinical applications to help researchers understand when each may be more relevant to their area of investigation.
Regulatory Note: BPC-157 was placed in FDA Category 2 (restricted from compounding) in 2024, and TB-500 is not FDA-approved for any indication. Both are prohibited by WADA. Neither peptide is approved for human therapeutic use.
Mechanism of Action Comparison#
BPC-157#
BPC-157 operates through a pleiotropic cytoprotective mechanism centered on endothelial and vascular signaling. Its primary pathway involves upregulation of VEGF-A and VEGFR2 with rapid receptor phosphorylation and internalization, leading to downstream AKT phosphorylation and eNOS activation. This VEGFR2-Akt-eNOS axis is central to its angiogenic and tissue-protective effects.
A second key pathway involves Src-Caveolin-1-eNOS signaling, through which BPC-157 modulates vasomotor tone and promotes collateral vessel recruitment. This mechanism enables rapid bypass of vascular occlusions and has been demonstrated in multiple ischemia models. BPC-157 also exhibits bidirectional NO-system normalization, counteracting both NOS inhibition (L-NAME) and NOS overstimulation (L-arginine), which distinguishes it from agents that simply increase or decrease NO.
At the cellular level, BPC-157 activates the FAK-paxillin pathway to promote fibroblast migration and tissue outgrowth, and it upregulates growth hormone receptor (GHR) expression in tendon fibroblasts, enhancing responsiveness to endogenous growth hormone. Notably, a broad receptor binding screen found no direct pharmacological affinity for classical neurotransmitter receptor families, suggesting an upstream modulatory mode of action rather than direct receptor agonism.
TB-500#
TB-500's mechanism is anchored by its role as the principal actin-sequestering protein in eukaryotic cells. Approximately 50% of cellular actin exists as monomeric G-actin, and Thymosin Beta-4 binds most of this pool in a 1:1 stoichiometric complex through its conserved LKKTET motif (residues 17-22). When cells receive migration signals, G-actin is released from the Tβ4 complex, enabling rapid actin polymerization at the leading edge. This controlled actin release is fundamental to wound healing, immune cell trafficking, and tissue repair.
Beyond cytoskeletal regulation, TB-500 activates integrin-linked kinase (ILK), which in turn activates the Akt/protein kinase B survival pathway. This ILK-Akt axis was demonstrated in the landmark 2004 Nature study by Bock-Marquette and colleagues, showing cardiomyocyte survival after ischemic injury. TB-500 also inhibits TNF-alpha-stimulated NF-kB binding activity through its interaction with PINCH-1 and ILK signaling partners, providing anti-inflammatory effects that are independent of its actin-sequestering function.
The peptide also demonstrates significant anti-fibrotic properties by reducing myofibroblast numbers in healing tissues, resulting in decreased scar formation. Its N-terminal metabolite Ac-SDKP has independent anti-fibrotic activity and is degraded by angiotensin-converting enzyme (ACE), creating a pharmacologically relevant interaction with ACE inhibitors.
Mechanistic Comparison#
| Feature | BPC-157 | TB-500 |
|---|---|---|
| Primary pathway | VEGFR2-Akt-eNOS angiogenesis | G-actin sequestration and cell migration |
| Size | 15 amino acids (1,419 Da) | 43 amino acids (4,963 Da) |
| Origin | Synthetic fragment of gastric protein | Synthetic full-length Thymosin Beta-4 |
| Endogenous presence | Derived from gastric juice protein | Present in virtually all mammalian cells |
| Anti-inflammatory mechanism | NO-system normalization | NF-kB inhibition via PINCH-1/ILK |
| Pro-angiogenic mechanism | VEGF-A/VEGFR2 upregulation | Endothelial cell migration and tubule formation |
| Cell migration pathway | FAK-paxillin activation | Actin monomer release for polymerization |
| Direct receptor binding | None identified at classical receptors | LKKTET motif binds G-actin |
Dosing Comparison#
BPC-157 Dosing#
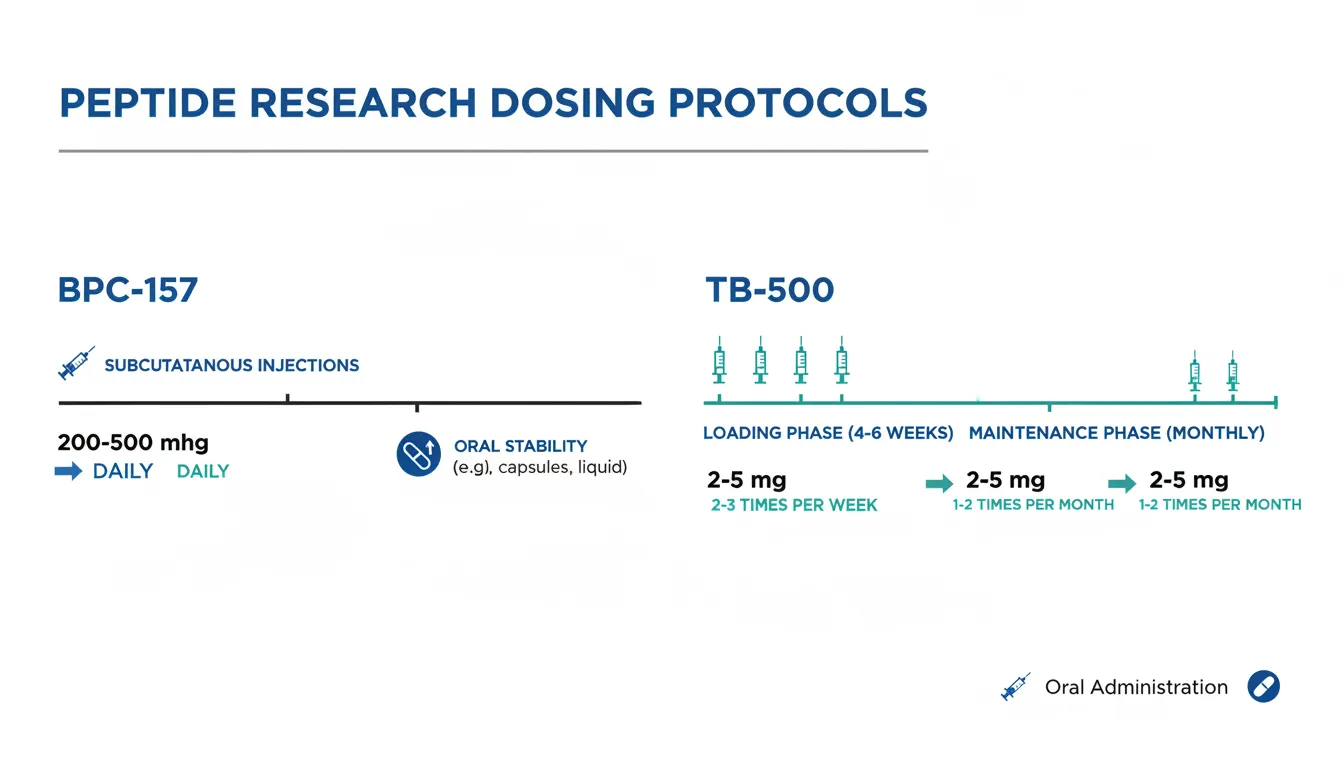
Research protocols for BPC-157 typically involve subcutaneous injections at doses of 200-500 mcg, administered 1-2 times daily. Common protocols use 250 mcg once daily injected near the target tissue for localized application, or 500 mcg once daily for systemic research protocols. Treatment durations in preclinical studies range from 4 to 12 weeks.
BPC-157 has a notable advantage in route flexibility. The peptide is reported to be stable in human gastric juice, and preclinical studies have demonstrated efficacy with oral dosing (typically in drinking water at 0.16 mcg/mL). However, quantitative oral bioavailability in humans has not been established, and plasma levels after oral and rectal dosing are frequently below the limit of quantification.
For intramuscular administration in animals, bioavailability is approximately 14-19% in rats and 45-51% in dogs, with very rapid absorption (Tmax of approximately 3 minutes) and short parent half-life under 30 minutes. Reconstitution typically uses 1-2 mL of bacteriostatic water per 5 mg vial.
TB-500 Dosing#
TB-500 dosing in research contexts commonly follows a loading and maintenance pattern. During the loading phase, doses of 2-5 mg are administered subcutaneously 2-3 times per week for 4-6 weeks. This is followed by a maintenance phase of 2-5 mg once or twice per month.
In clinical trials, intravenous doses ranged from 42 to 1260 mg daily for up to 14 days, with dose-proportional pharmacokinetics and no dose-limiting toxicities at any level. Topical formulations have been used in wound healing trials (0.03% gel) and ophthalmic trials (0.1% solution).
TB-500 is endogenously present in serum at approximately 12-18 ng/mL in healthy individuals, with levels increasing at injury sites due to platelet degranulation. Subcutaneous bioavailability has not been formally characterized, which represents a significant evidence gap.
Dosing Comparison Table#
| Parameter | BPC-157 | TB-500 |
|---|---|---|
| Typical research dose | 200-500 mcg/day | 2-5 mg, 2-3x/week (loading) |
| Administration frequency | 1-2 times daily | 2-3 times weekly, then monthly |
| Common route | Subcutaneous (near injury site) | Subcutaneous |
| Oral feasibility | Stable in gastric juice; studied orally | Not established for oral use |
| Half-life (animal data) | Under 30 minutes (parent peptide) | Increases with dose; longer than BPC-157 |
| Clinical trial doses (IV) | Phase I registered but data limited | 42-1260 mg IV (well tolerated) |
| Reconstitution | 1-2 mL bacteriostatic water per 5 mg vial | 1-2 mL bacteriostatic water per 5 mg vial |
Side Effects Comparison#
BPC-157 Side Effects#
The safety profile of BPC-157 in humans is based on very limited data. In small human studies, no adverse events were reported: 0/2 in an IV pilot, 0/12 in intravesical treatment, and 0/16 in intra-articular injections. A 53-patient enema trial for ulcerative colitis reported tolerability comparable to placebo. Animal toxicology studies report an LD50 greater than 2,000 mg/kg in mice, negative genotoxicity batteries, and no teratogenic effects in rat reproductive studies.
Common anecdotal reports include mild injection site reactions and occasional nausea, though these are not systematically documented. Theoretical concerns include stimulation of angiogenesis (relevant for individuals with active malignancy), NO-pathway modulation (potential interactions with vasodilatory drugs), and effects on hemostasis (relevant for those on anticoagulant therapy).
No formal human contraindications have been established. Precautionary contraindications based on mechanism include active cancer, pregnancy, concurrent use of NO-modulating drugs, and bleeding disorders.
TB-500 Side Effects#
TB-500 has more robust human safety data from two Phase I clinical trials. In the 40-volunteer Western population study, IV Tβ4 at 42-1260 mg was well tolerated with no dose-limiting toxicities, no serious adverse events, and no evidence of immunogenicity. A subsequent Phase I study in Chinese volunteers confirmed these findings.
Reported side effects from clinical trials include mild injection site reactions (common), headache (uncommon), nausea (uncommon), dizziness (rare), transient fatigue (uncommon), and flu-like symptoms during initial doses (rare). All reported adverse events were mild to moderate in intensity.
The primary theoretical safety concern is Tβ4's role in tumor biology. The peptide is overexpressed in some tumor types, and its promotion of angiogenesis and cell migration could theoretically support tumor growth. However, no clinical evidence directly links exogenous Tβ4 administration to cancer development. Precautionary contraindications include active malignancy, pregnancy, and concurrent immunosuppressive therapy.
A notable pharmacological interaction exists with ACE inhibitors, as the Tβ4 metabolite Ac-SDKP is normally degraded by ACE. Concurrent TB-500 use could elevate Ac-SDKP levels and potentiate anti-fibrotic effects.
Safety Comparison Summary#
| Aspect | BPC-157 | TB-500 |
|---|---|---|
| Human safety trials | Limited (small pilots, one 53-patient trial) | Two Phase I trials (40 and ~30 volunteers) |
| Highest tested human dose | 20 mg IV (pilot, n=2) | 1,260 mg IV (Phase I, 14 days) |
| Serious adverse events | None reported | None reported |
| Animal LD50 | >2,000 mg/kg (mice) | Not reached in standard protocols |
| Cancer concern | Theoretical (VEGF upregulation) | Theoretical (cell migration, Tβ4 overexpression in some tumors) |
| Key drug interaction | NO-modulating drugs, anticoagulants | ACE inhibitors (Ac-SDKP metabolism) |
| WADA status | Prohibited | Prohibited |
Research Evidence Comparison#
BPC-157 Research#
BPC-157 has an extensive preclinical literature spanning hundreds of animal studies across multiple therapeutic areas. Key evidence includes consistent improvements in tendon, ligament, and muscle healing in rat transection models, with biomechanical recovery toward normal values. Gastrointestinal studies demonstrate mucosal healing, fistula closure, and anastomotic repair. Spinal cord injury models showed functional recovery with reduced histological damage. Skin wound healing studies demonstrated accelerated closure (77-82% by day 18 versus 60% for controls) with enhanced VEGF-A expression.
However, the evidence base has notable limitations. A 2025 systematic review of musculoskeletal applications found 36 studies (35 preclinical, 1 small retrospective clinical), concluding that clinical efficacy and safety remain unestablished. Most preclinical findings originate from a small number of research groups, raising concerns about independent replication. The sole registered Phase I trial (NCT02637284) has unclear status, and human pharmacokinetics show plasma levels frequently below the assay's limit of quantification after oral and rectal dosing.
Evidence level: Low -- predominantly preclinical with minimal human data.
TB-500 Research#
TB-500's evidence base includes both extensive preclinical work and a more developed clinical trial portfolio. The foundational 1999 Malinda study demonstrated 42% increased re-epithelialization at day 4 and 61% at day 7 in rat wounds. The seminal 2004 Bock-Marquette Nature publication established ILK-Akt-mediated cardioprotection, leading to further cardiac research. Corneal healing studies advanced to clinical trials, with RGN-259 completing Phase II and III studies.
The clinical development program includes two Phase I safety studies confirming tolerability at IV doses up to 1260 mg, Phase II trials for venous stasis ulcers showing healing acceleration of approximately one month in responders, and Phase III results in neurotrophic keratopathy demonstrating improved healing and comfort versus placebo.
Important limitations include the failure to replicate rodent cardiac findings in a pig model (Stark et al., 2016), limited long-term safety data beyond 14 days of human dosing, and the absence of large-scale Phase III trials for systemic indications.
Evidence level: Moderate -- preclinical evidence supported by Phase I/II/III clinical data for ophthalmic indications.
Evidence Comparison Table#
| Metric | BPC-157 | TB-500 |
|---|---|---|
| Preclinical studies | 100+ across multiple tissue types | Extensive across wound, cardiac, corneal, stroke |
| Human Phase I | 1 registered (status unclear) | 2 completed (Western and Chinese populations) |
| Human Phase II | 1 small UC trial (53 patients, enema) | Venous stasis ulcers, dry eye disease |
| Human Phase III | None | Neurotrophic keratopathy (RGN-259) |
| Publication in high-impact journals | Primarily specialty journals | Nature (2004), JACI, JID, IJMS |
| Independent replication | Limited (small number of research groups) | Broader (multiple independent labs) |
| Systematic reviews | 1 (2025, musculoskeletal) | Limited |
Key Differences Summary#
- Molecular origin: BPC-157 is a synthetic fragment of a gastric protein; TB-500 is a synthetic copy of the endogenous Thymosin Beta-4 found in all cells.
- Primary mechanism: BPC-157 acts through VEGF/NO-mediated angiogenesis and barrier stabilization; TB-500 acts through actin-mediated cell migration and ILK-Akt survival signaling.
- Clinical advancement: TB-500 has progressed further in clinical trials, with completed Phase I-III studies, while BPC-157 remains largely preclinical.
- Dosing pattern: BPC-157 is typically dosed daily at microgram levels; TB-500 uses milligram doses 2-3 times weekly.
- Route flexibility: BPC-157 has demonstrated oral stability and preclinical efficacy via oral routes; TB-500 has been studied primarily via injection and topical application.
- GI specificity: BPC-157 has a strong profile for gastrointestinal healing given its gastric origin; TB-500 has no specific GI evidence.
- Cardiac research: TB-500 has a well-characterized cardioprotective mechanism (ILK-Akt) published in Nature; BPC-157's cardiac evidence is limited to preclinical isoprenaline MI models.
- Combination evidence: No controlled studies have evaluated the BPC-157/TB-500 combination ("Wolverine Stack"); the rationale for combining them is based on complementary mechanisms rather than direct evidence.
Conclusion#
BPC-157 and TB-500 represent two distinct approaches to peptide-mediated tissue repair. BPC-157 excels in preclinical models of gastrointestinal healing and musculoskeletal repair, acting through vascular and cytoprotective mechanisms. TB-500 has a more advanced clinical development program, particularly for ophthalmic and dermal wound healing applications, operating through cytoskeletal regulation and cell survival pathways.
For researchers focused on gut healing, tendon repair, or musculoskeletal applications, BPC-157 has the larger preclinical evidence base. For those interested in wound healing, corneal repair, or cardiac protection, TB-500 offers more advanced clinical data and a clearer regulatory pathway.
The combination of both peptides is widely discussed but lacks controlled evidence. While the complementary mechanisms -- BPC-157's angiogenic and endothelial effects paired with TB-500's cell migration and anti-fibrotic properties -- provide a logical theoretical framework, researchers should recognize that synergistic or additive effects have not been demonstrated in formal studies. Both peptides remain investigational, are prohibited by WADA, and are not approved for human therapeutic use by any regulatory agency.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Gastrointestinal Healing Research
BPC-157
BPC-157 is derived from gastric juice and has the strongest preclinical evidence for GI protection, colitis healing, fistula closure, and anastomosis repair across numerous animal models.
Tendon and Ligament Injury Research
BPC-157
Extensive preclinical evidence in MCL transection, Achilles tendon, and other musculoskeletal models with consistent improvements in biomechanical properties and functional recovery.
Wound Healing and Dermal Repair
TB-500
TB-500 has Phase II clinical data for venous stasis and pressure ulcers showing healing acceleration. Its keratinocyte migration activity (2-3 fold increase) and anti-scarring properties are well characterized.
Corneal and Ophthalmic Applications
TB-500
RGN-259 (0.1% Thymosin Beta-4) advanced through Phase III trials for neurotrophic keratopathy with 35.1% reduction in ocular discomfort and 59.1% reduction in corneal staining versus placebo.
Cardiac Protection Research
TB-500
Tβ4 demonstrated ILK-Akt-mediated cardiomyocyte survival in Nature (2004) and can reactivate epicardial progenitor cells, though large animal translation has been inconsistent.
Combined Healing Protocol Research
Both (Wolverine Stack)
The distinct mechanisms (BPC-157 via VEGF/NO angiogenesis, TB-500 via actin-mediated cell migration) provide a theoretical rationale for combination, though no controlled combination studies exist.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About BPC-157 vs TB-500: Comprehensive Comparison of Healing Peptides
Which is better, BPC-157 or TB-500?
BPC-157 and TB-500 target tissue repair through distinct but complementary mechanisms. BPC-157 has a stronger preclinical profile for gastrointestinal and musculoskeletal healing, while TB-500 has more advanced clinical trial data, particularly for ophthalmic and dermal wound applications. Neither peptide is approved for human therapeutic use. Their combination (the "Wolverine Stack") lacks controlled combination studies. Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between BPC-157 and TB-500?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to TB-500; Side Effect Profile: advantage goes to neither (tie). 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider BPC-157 over TB-500?
For the scenario of "Gastrointestinal Healing Research," research data suggests BPC-157 may be more relevant. BPC-157 is derived from gastric juice and has the strongest preclinical evidence for GI protection, colitis healing, fistula closure, and anastomosis repair across numerous animal models.. This is based on currently available evidence and individual circumstances may differ.
How do BPC-157 and TB-500 differ in their mechanisms of action?
BPC-157: Acts through VEGFR2-Akt-eNOS signaling, Src-Caveolin-1-eNOS vasomotor modulation, and FAK-paxillin migration pathways. Promotes angiogenesis, normalizes NO levels, and stabilizes endothelial/epithe.... TB-500: Functions primarily through G-actin sequestration, regulating cytoskeletal dynamics and cell migration. Activates integrin-linked kinase (ILK) and Akt survival signaling. Inhibits NF-kB-mediated in....
Which has fewer side effects, BPC-157 or TB-500?
In terms of side effects and tolerability, the advantage goes to neither (comparable). BPC-157: Generally well tolerated in animal studies. No adverse events reported in small human studies (0/2 IV, 0/12 intravesical, 0/16 intra-articular). LD.... TB-500: Well tolerated in Phase I trials at IV doses up to 1260 mg with no dose-limiting toxicities. Mild side effects include injection site reactions, he....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.