GHRH vs GHRP: Two Pathways to Growth Hormone Release Explained

Introduction#
Growth hormone (GH) secretion from the anterior pituitary is governed by two primary stimulatory pathways that act through distinct receptors, distinct signaling cascades, and distinct physiological mechanisms. Understanding these two pathways is the single most important concept for anyone evaluating growth hormone-releasing peptides.
The first pathway operates through the growth hormone-releasing hormone (GHRH) receptor. Peptides in this class — including Sermorelin, CJC-1295 DAC, and CJC-1295 (No DAC) — mimic or enhance the body's own GHRH signal that tells pituitary somatotrophs to synthesize and release growth hormone.
The second pathway operates through the growth hormone secretagogue receptor (GHS-R1a), also known as the ghrelin receptor. Peptides in this class — including Ipamorelin, GHRP-6, GHRP-2, and Hexarelin — activate the same receptor as the endogenous hunger hormone ghrelin, amplifying GH release through a parallel mechanism.
These two pathways are not redundant. They converge on the same cell type but through different intracellular signaling routes, producing a synergistic effect when activated together that is greater than the sum of either pathway alone. This synergy forms the scientific basis for combination protocols that pair a GHRH analog with a GHRP.
This guide explains each pathway in detail, compares their key differences, and explores how they interact to shape the pulsatile pattern of growth hormone secretion.
The GHRH Pathway: Amplifying the Natural Signal#
How GHRH Works#
Growth hormone-releasing hormone is a 44-amino acid peptide produced by the arcuate nucleus of the hypothalamus. It is released in a pulsatile fashion into the hypophyseal portal vasculature, traveling a short distance to the anterior pituitary where it binds to the GHRH receptor (GHRH-R) on somatotroph cells.
The GHRH receptor is a G protein-coupled receptor that signals primarily through the Gs-cAMP-PKA cascade. When GHRH binds, it activates adenylate cyclase, increasing intracellular cyclic AMP (cAMP), which activates protein kinase A (PKA). This cascade has two primary effects:
- Acute GH release — PKA phosphorylates ion channels and exocytotic machinery, triggering the release of pre-formed GH granules from somatotroph storage vesicles
- GH gene transcription — PKA activates the transcription factor Pit-1, driving new GH mRNA synthesis and long-term maintenance of pituitary GH stores
This dual function means that GHRH pathway activation not only releases existing GH but also replenishes the pituitary's capacity to produce more — a critical distinction from the ghrelin pathway.
GHRH Analog Peptides#
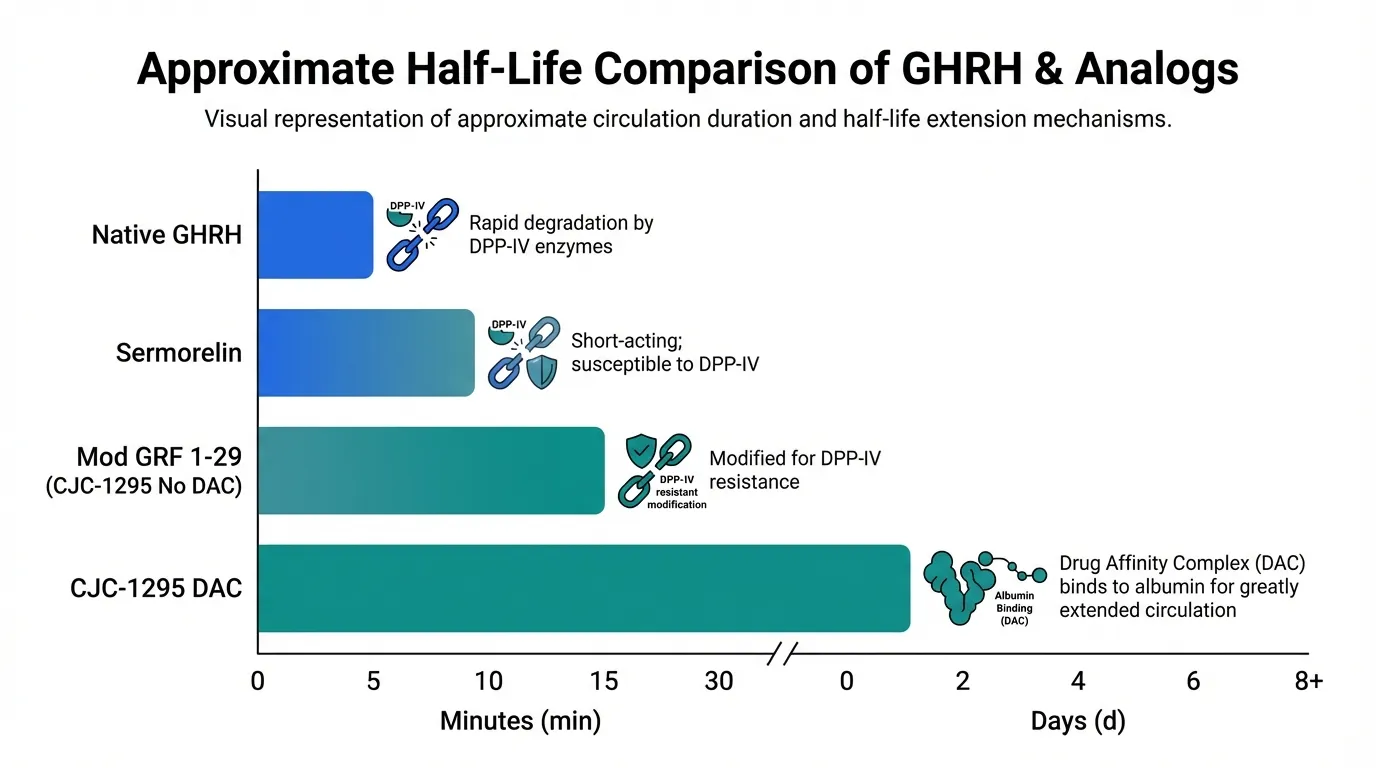
GHRH analogs are synthetic peptides designed to mimic or improve upon the native GHRH molecule. The key challenge with native GHRH is its extremely short half-life in circulation — it is rapidly degraded by the enzyme dipeptidyl peptidase IV (DPP-IV), which cleaves the N-terminal dipeptide within minutes.
Sermorelin is the first 29 amino acids of native GHRH (GRF 1-29), retaining full biological activity at the GHRH receptor. It was previously FDA-approved for diagnostic use and for GH deficiency in children. Its half-life is approximately 10-20 minutes — longer than native GHRH but still brief. Sermorelin produces a GH pulse that mimics the natural physiological pattern, and its effects are gated by somatostatin (the GH-inhibiting hormone), meaning the pituitary's own negative feedback loop remains intact.
CJC-1295 (No DAC), also called Modified GRF 1-29 (Mod GRF 1-29), improves on sermorelin by incorporating four amino acid substitutions at positions 2, 8, 15, and 27 that protect against DPP-IV degradation and improve receptor binding. This extends the effective half-life to approximately 30 minutes or longer while preserving pulsatile GH release. It is the most commonly used GHRH analog in combination protocols with GHRPs.
CJC-1295 DAC adds a Drug Affinity Complex — a maleimidopropionic acid linker that covalently binds to serum albumin after injection. This extends the half-life to approximately 6-8 days, creating a fundamentally different pharmacokinetic profile. Rather than producing a discrete GH pulse, DAC-conjugated CJC-1295 creates sustained elevation of GHRH receptor stimulation, resulting in elevated baseline GH and IGF-1 levels. This is a trade-off: convenience of less frequent dosing versus loss of the pulsatile release pattern that characterizes physiological GH secretion.
Characteristics of the GHRH Pathway#
The GHRH pathway has several defining features:
- Somatostatin sensitivity — GH release through the GHRH receptor is inhibited by somatostatin. If somatostatin tone is high (as it naturally is between GH pulses), GHRH analogs produce a blunted response. This is a safety feature that prevents supraphysiological GH levels but also means GHRH analogs are less effective during somatostatin-dominant periods.
- GH synthesis upregulation — Unlike GHRPs, GHRH analogs directly increase GH mRNA transcription, maintaining pituitary GH reserves over time.
- Clean hormonal profile — GHRH receptor activation does not stimulate cortisol, prolactin, or ACTH release. It does not stimulate appetite. This makes GHRH analogs the "cleanest" option from a side effect perspective.
- Age-dependent decline — The GH response to GHRH decreases with age, partly due to reduced somatotroph mass and partly due to increased somatostatin tone. This decline is one reason GHRH analogs alone may produce a modest response in older individuals.
The GHRP / Ghrelin Pathway: A Parallel Amplifier#
How the Ghrelin Receptor Works#
The growth hormone secretagogue receptor (GHS-R1a) was identified in the 1990s as the molecular target for a class of synthetic peptides (GHRPs) that had been developed empirically since the 1970s. The endogenous ligand for this receptor — ghrelin — was discovered in 1999, revealing that GHRPs had been unknowingly targeting the same receptor as the body's own hunger hormone.
GHS-R1a is expressed on pituitary somatotrophs (where it triggers GH release) and in the hypothalamus (where it modulates appetite, somatostatin release, and GHRH neuron activity). The receptor signals primarily through the Gq-phospholipase C (PLC) pathway, generating inositol trisphosphate (IP3) and diacylglycerol (DAG). This leads to calcium release from intracellular stores and activation of protein kinase C (PKC), ultimately triggering GH granule exocytosis.
Critically, this is a different intracellular cascade from the cAMP-PKA pathway used by GHRH. The two signaling systems converge at the level of calcium mobilization and exocytosis, which is why they produce synergistic rather than additive effects.
The GHRP Family#
Growth hormone-releasing peptides were developed through systematic structure-activity optimization beginning with the enkephalin-derived peptide GHRP-6 in the 1980s. They share the common mechanism of GHS-R1a agonism but differ substantially in their selectivity, potency, and off-target effects.
GHRP-6 is the prototypical GHRP, a hexapeptide (His-D-Trp-Ala-Trp-D-Phe-Lys-NH2) that produces potent, dose-dependent GH release. It is the least selective of the commonly studied GHRPs, producing meaningful increases in cortisol (via ACTH stimulation), prolactin, and — notably — strong appetite stimulation through its activation of ghrelin-mediated hunger circuits in the hypothalamus. GHRP-6 also does not produce significant tachyphylaxis (reduced response with repeated dosing), making it viable for sustained use.
GHRP-2 (Pralmorelin) is a second-generation hexapeptide with improved potency and somewhat better selectivity than GHRP-6. It produces strong GH release with less cortisol and prolactin elevation than GHRP-6, though these effects are still measurable at higher doses. It is approved in Japan as a diagnostic agent for GH deficiency. Appetite stimulation is present but less pronounced than with GHRP-6.
Hexarelin is the most potent GHRP studied in humans, producing the highest acute GH levels of any peptide in this class. However, it also produces the most prominent cortisol and prolactin elevation and is highly prone to tachyphylaxis — the GH response diminishes significantly within weeks of continuous use. Hexarelin also binds to cardiac CD36 receptors, providing cardioprotective effects independent of GH.
Ipamorelin represents the other end of the selectivity spectrum. This pentapeptide produces dose-dependent GH release through GHS-R1a without significant elevation of cortisol, ACTH, or prolactin. It does not stimulate appetite at GH-effective doses. This exceptional selectivity makes ipamorelin the preferred GHRP for protocols where clean GH stimulation is prioritized over maximum amplitude.
Characteristics of the GHRP Pathway#
The ghrelin receptor pathway has several defining features that contrast with the GHRH pathway:
- Somatostatin suppression — GHRPs actively suppress somatostatin release from the hypothalamus, effectively removing the brake on GH secretion. This is a major differentiator from GHRH analogs and partly explains why GHRPs can produce GH release even during somatostatin-dominant periods.
- GHRH neuron activation — GHRPs stimulate hypothalamic GHRH neurons, creating a feedforward loop that indirectly activates the GHRH pathway as well. This dual hypothalamic action (suppressing somatostatin + stimulating GHRH) amplifies the pituitary-level GH release.
- Variable selectivity — Unlike GHRH analogs, which have a uniformly clean hormonal profile, GHRPs vary enormously in their off-target effects. The cortisol, prolactin, and appetite effects are receptor-mediated consequences of GHS-R1a signaling in different tissues, and different GHRPs activate these pathways to different degrees.
- No GH gene upregulation — GHRPs primarily release pre-formed GH stores without significantly increasing GH mRNA transcription. Over time, this could theoretically deplete pituitary reserves if not paired with GHRH pathway stimulation.
Head-to-Head: GHRH Analogs vs GHRPs#
| Feature | GHRH Analogs | GHRPs |
|---|---|---|
| Receptor | GHRH-R (Gs-cAMP-PKA) | GHS-R1a (Gq-PLC-IP3-PKC) |
| Primary action | GH synthesis + release | GH release (stored granules) |
| Somatostatin interaction | Inhibited by somatostatin | Suppresses somatostatin release |
| Cortisol effect | None | Variable (none to significant) |
| Prolactin effect | None | Variable (none to significant) |
| Appetite effect | None | Variable (none to strong) |
| GH gene transcription | Yes (via Pit-1) | No |
| Age-related decline in response | More pronounced | Less pronounced |
| Tachyphylaxis risk | Low | Variable (low to high) |
| Examples | Sermorelin, CJC-1295, Tesamorelin | Ipamorelin, GHRP-6, GHRP-2, Hexarelin |
The Synergy Effect: Why Combining Pathways Matters#
The Science of Synergistic GH Release#
The most consistently replicated finding in growth hormone secretagogue research is that simultaneous activation of the GHRH and GHS-R1a receptors produces GH release that is synergistic — not merely additive. If a GHRH analog produces X amount of GH alone, and a GHRP produces Y amount alone, the combination produces significantly more than X + Y.
This synergy has been documented across multiple study designs. In a foundational study, the combination of GHRH with GHRP-6 produced GH responses approximately 2- to 3-fold greater than the sum of the individual agents. Similar results have been observed with other GHRH/GHRP pairings.
The mechanism of this synergy involves multiple levels of interaction:
-
Complementary intracellular signaling — The cAMP/PKA pathway (GHRH) and the PLC/IP3/PKC pathway (GHRPs) converge on calcium mobilization through different mechanisms. When both are activated simultaneously, the resulting calcium signal is amplified beyond what either can achieve alone.
-
Somatostatin suppression — GHRPs reduce somatostatin tone at the hypothalamic level, which "opens the gate" for GHRH to act more effectively at the pituitary. GHRH analogs are normally restrained by tonic somatostatin inhibition; GHRPs remove this restraint while GHRH drives the release.
-
Hypothalamic feedforward — GHRPs stimulate endogenous GHRH release from hypothalamic neurons, which adds to the effect of exogenous GHRH analogs acting directly at the pituitary. This creates a three-pronged stimulus: direct GHRH analog at the pituitary + endogenous GHRH from GHRP-stimulated neurons + direct GHRP at the pituitary.
-
Temporal optimization — The GH pulse produced by the combination is both larger in amplitude and more sustained than either agent alone, creating a physiologically robust secretory event.
Common Combination Pairings#
The most widely studied and used combinations pair one GHRH analog with one GHRP:
CJC-1295 (No DAC) + Ipamorelin — This is the most commonly referenced combination. Mod GRF 1-29 provides GHRH-receptor activation with improved stability over sermorelin, while ipamorelin provides GHS-R1a activation with the cleanest selectivity profile. The combination produces synergistic GH release while minimizing cortisol, prolactin, and appetite effects.
Sermorelin + GHRP-6 — An older but well-studied combination. Sermorelin provides the GHRH stimulus while GHRP-6 provides robust ghrelin-receptor activation. This combination produces strong GH release but carries GHRP-6's appetite stimulation and mild cortisol effects.
Sermorelin + Ipamorelin — A variation that substitutes ipamorelin for GHRP-6 to achieve a cleaner side effect profile while still capturing the synergistic benefit.
CJC-1295 DAC + Ipamorelin — A less common pairing because the DAC version's continuous GHRH-receptor stimulation produces sustained rather than pulsatile GH elevation. When combined with pulsatile GHRP administration, the result is a complex pharmacokinetic profile with elevated GH baseline punctuated by GHRP-driven pulses.
Why Not Combine Two GHRPs?#
Combining two GHRPs (for example, ipamorelin + GHRP-6) does not produce meaningful synergy because both peptides compete for the same receptor (GHS-R1a). Similarly, combining two GHRH analogs provides no benefit beyond using a single GHRH analog at an adequate dose. The synergy is pathway-specific — it requires simultaneous activation of both the GHRH-R and GHS-R1a.
Pulsatile vs Continuous GH Release: Why the Pattern Matters#
The Physiology of GH Pulsatility#
Natural GH secretion is not continuous. The pituitary releases GH in discrete pulses, with the largest occurring during slow-wave sleep and smaller pulses throughout the day. Between pulses, GH levels fall to near-undetectable trough levels. This pulsatile pattern is maintained by the alternating dominance of GHRH (which drives pulses) and somatostatin (which creates troughs).
This pattern is not arbitrary. Research indicates that the biological effects of GH depend not just on the total amount released but on the pattern of release:
- Pulsatile GH preferentially activates the JAK2-STAT5b signaling pathway in the liver, which drives IGF-1 production and the majority of GH's anabolic and metabolic effects.
- Continuous GH exposure activates different STAT pathways and produces a different gene expression profile. Studies in animal models have shown that continuous GH infusion produces qualitatively different metabolic effects compared to pulsatile administration, including different effects on liver gene expression, body composition, and even sex-specific growth patterns.
Implications for Peptide Selection#
This distinction has practical implications for peptide selection:
Pulsatile-preserving approaches — Sermorelin, CJC-1295 (No DAC), Ipamorelin, GHRP-2, GHRP-6, and Hexarelin all produce discrete GH pulses when administered as bolus injections. Their short-to-moderate half-lives mean that GH levels rise, peak, and return to baseline between doses, preserving the pulsatile pattern. These peptides work with the body's existing feedback mechanisms.
Continuous elevation — CJC-1295 DAC, with its 6-8 day half-life, creates sustained GHRH-receptor stimulation. This results in elevated baseline GH and IGF-1 levels rather than discrete pulses. While this is convenient (fewer injections), it represents a departure from physiological GH dynamics. Some researchers consider this suboptimal for long-term use due to the potential for altered GH signaling patterns and increased somatotroph desensitization.
Exogenous GH (HGH 191aa) — For context, recombinant human growth hormone bypasses the pituitary entirely, delivering GH directly. When injected as a daily subcutaneous dose, it produces a supraphysiological peak followed by a gradual decline — a pattern that is pulsatile but at a frequency and amplitude not governed by natural feedback systems.
Practical Considerations for Each Pathway#
When GHRH Analogs Are Preferred#
GHRH analogs are the better choice when:
- Minimal side effects are the priority — No cortisol, prolactin, or appetite effects
- GH synthesis maintenance matters — GHRH analogs upregulate GH gene transcription, supporting long-term pituitary function
- The research context requires a clean GH stimulus — Isolating GH effects from cortisol or prolactin confounders
- FDA-approved options are required — Tesamorelin (Egrifta) is the only FDA-approved GH secretagogue
When GHRPs Are Preferred#
GHRPs are the better choice when:
- Somatostatin resistance is a concern — GHRPs suppress somatostatin, making them effective even when somatostatin tone is high (as in older individuals)
- Appetite stimulation is desirable — GHRP-6 and GHRP-2 increase appetite through ghrelin signaling, useful in cachexia or wasting contexts
- The strongest GH response is needed — GHRPs (particularly hexarelin and GHRP-2) produce higher peak GH levels than GHRH analogs alone
- Age-related GH decline is present — GHRPs show less age-related attenuation of response compared to GHRH analogs
When Combination Is Optimal#
The combination approach is favored when:
- Maximum physiological GH release is the goal — The synergistic effect produces the largest GH pulses achievable through secretagogue stimulation
- Pulsatile pattern should be maintained — Using short-acting agents from both pathways preserves the rise-and-fall pattern
- Pituitary function should be supported long-term — The GHRH analog maintains GH synthesis while the GHRP amplifies each pulse
- The somatostatin-GHRH balance should be optimized — The GHRP suppresses somatostatin while the GHRH analog drives release, creating optimal conditions for each pulse
Age, Somatopause, and Pathway Relevance#
Growth hormone secretion declines approximately 14% per decade after age 30, a phenomenon termed somatopause. This decline involves changes in both pathways:
-
GHRH pathway changes: Somatotroph mass decreases with age, and somatostatin tone increases. The pituitary response to GHRH stimulation is blunted in older individuals. Studies with sermorelin have shown that while GH release can still be stimulated in elderly subjects, the magnitude of response is reduced compared to younger adults.
-
Ghrelin pathway changes: The GH response to GHRPs also declines with age but to a lesser degree than the GHRH response. GHRPs partially overcome the age-related increase in somatostatin tone by suppressing somatostatin release. Studies have demonstrated that GHRP-2 and GHRP-6 can partially restore GH secretion in aging subjects.
-
Combination advantage in aging: The synergistic combination approach appears to be particularly valuable in older populations. By simultaneously activating both pathways and suppressing somatostatin, the combination can overcome age-related barriers that limit either pathway alone.
This age-dependent differential response has led some researchers to favor GHRP-dominant approaches in older individuals, where somatostatin suppression may be more important than GHRH receptor stimulation for achieving adequate GH pulses.
Regulatory Status and Evidence Landscape#
The evidence base varies substantially across these peptides:
FDA-approved: Tesamorelin (Egrifta) is the only FDA-approved GH secretagogue, indicated for HIV-associated lipodystrophy. Sermorelin was previously FDA-approved for GH deficiency in children but was withdrawn for commercial reasons.
Regulatory approval outside the US: GHRP-2 (pralmorelin) is approved in Japan as a diagnostic tool for GH deficiency.
Investigational with clinical data: Ipamorelin has Phase I/II clinical data. GHRP-6, GHRP-2, and Hexarelin have extensive clinical pharmacology data from human studies.
Increased regulatory scrutiny: CJC-1295 (both DAC and No DAC) came under increased regulatory scrutiny following the 2024 FDA compounding restrictions affecting several peptides.
The quality and depth of human evidence should be considered when evaluating these peptides. Tesamorelin has the largest and most rigorous clinical dataset, while CJC-1295 has the most limited human trial data relative to its widespread research use.
Summary#
The GHRH and GHRP pathways represent two fundamentally different but complementary mechanisms for stimulating growth hormone release. GHRH analogs (Sermorelin, CJC-1295 DAC, CJC-1295 (No DAC)) work through the cAMP-PKA cascade to drive both GH release and GH synthesis, with a clean hormonal profile but sensitivity to somatostatin inhibition. GHRPs (Ipamorelin, GHRP-6, GHRP-2, Hexarelin) work through the PLC-IP3-PKC cascade to release stored GH while suppressing somatostatin, with variable selectivity ranging from ipamorelin's clean profile to hexarelin's broad hormonal effects.
The combination of both pathways produces synergistic GH release by engaging complementary signaling cascades, removing somatostatin inhibition, and creating feedforward amplification at the hypothalamic level. This synergistic principle underlies the widely studied CJC-1295 (No DAC) + Ipamorelin combination and remains the cornerstone of modern GH secretagogue research design.
For head-to-head comparisons of specific peptides, see GHRP-6 vs Ipamorelin, GHRP-2 vs Ipamorelin, or our comprehensive Growth Hormone Secretagogues Compared guide.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Sermorelin Overview and Research Guide
- Sermorelin Dosing Protocols
- Sermorelin Side Effects and Safety
- CJC-1295 DAC Overview and Research Guide
- CJC-1295 DAC Dosing Protocols
- CJC-1295 DAC Side Effects and Safety
- CJC-1295 (No DAC) Overview and Research Guide
- CJC-1295 (No DAC) Dosing Protocols
- CJC-1295 (No DAC) Side Effects and Safety
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- GHRP-6 Overview and Research Guide
- GHRP-6 Dosing Protocols
- GHRP-6 Side Effects and Safety

{kind=link}
Frequently Asked Questions About GHRH vs GHRP: Two Pathways to Growth Hormone Release Explained
What does this article cover?
Understand the two pathways to growth hormone release — GHRH analogs and GHRPs — how they work, differ, and combine for synergistic pulsatile GH secretion. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Sermorelin, CJC-1295 DAC, CJC-1295 (No DAC), Ipamorelin, GHRP-6. Key context: Sermorelin (GHRH analog and the prototypical example of the GHRH-receptor pathway for stimulating growth horm...); CJC-1295 DAC (Long-acting GHRH analog with albumin-binding DAC technology extending its half-life to several days); CJC-1295 (No DAC) (Modified GRF 1-29 analog representing the pulsatile GHRH-pathway approach used in combination pro...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "GHRH vs GHRP: Two Pathways to Growth Hormone Release Explained." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: GHRH analog and the prototypical example of the GHRH-receptor pathway for stimulating growth horm.... Long-acting GHRH analog with albumin-binding DAC technology extending its half-life to several days. Modified GRF 1-29 analog representing the pulsatile GHRH-pathway approach used in combination pro.... These takeaways are based on the research data available at the time of publication.
What is Sermorelin and why is it significant?
Sermorelin is a peptide discussed in this article because: GHRH analog and the prototypical example of the GHRH-receptor pathway for stimulating growth hormone release. For a complete profile of Sermorelin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?
A beginner-friendly guide to growth hormone secretagogues including ipamorelin, sermorelin, CJC-1295, and more. Learn how GH peptides work, compare options, and understand which secretagogue may fit your research goals.

Growth Hormone and Sleep: How GH Secretagogues Enhance Recovery
How growth hormone secretagogues enhance sleep recovery through nocturnal GH amplification. Covers ipamorelin, sermorelin, CJC-1295, and GHRP-6.

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
You Might Also Like
Related content you may find interesting