Best Peptides for Joint Pain and Tendon Repair: Research Guide

Introduction#
Joint pain and tendon injuries represent some of the most common reasons people explore peptide research. Connective tissue — including tendons, ligaments, cartilage, and the joint capsule — is notoriously slow to heal due to limited blood supply and low metabolic activity. This has driven interest in peptides that may accelerate or enhance the natural repair processes in these tissues.
This guide examines five peptides with research profiles relevant to joint and tendon health. The evidence ranges from BPC-157's extensive preclinical tendon repair data to the indirect support mechanisms of growth hormone secretagogues like ipamorelin. For each compound, we cover the specific research evidence, proposed mechanisms, and important limitations.
Important note: No peptide in this guide is FDA-approved for joint pain, tendon repair, or any musculoskeletal indication. All applications discussed are investigational or preclinical.
Why Connective Tissue Is Hard to Heal#
Understanding why peptides are studied for joint and tendon repair requires appreciating the biology of connective tissue healing:
- Limited blood supply — tendons and ligaments have significantly lower vascularity than muscle, which limits nutrient delivery and waste removal during repair
- Low cellularity — connective tissues have fewer cells (tenocytes, chondrocytes) per unit volume than most other tissues
- Slow collagen turnover — the primary structural protein in tendons and ligaments (type I collagen) has a very slow turnover rate, meaning repair is inherently slow
- Mechanical loading — joints and tendons are under constant mechanical stress, which can disrupt healing tissue before it has matured
Peptides studied for these applications typically target one or more of these limitations — promoting angiogenesis, stimulating cell migration and proliferation, enhancing collagen synthesis, or modulating inflammation.
1. BPC-157 (Body Protection Compound)#
Evidence Level: Extensive preclinical; no human joint/tendon clinical data Primary Mechanism: Angiogenesis promotion; growth factor upregulation; NO system modulation FDA Status: Category 2 (banned from compounding)
BPC-157 has the most extensive preclinical research profile for tendon and ligament repair of any peptide in this guide. Derived from a protective protein found in human gastric juice, BPC-157 has been studied in numerous animal models of connective tissue injury.
Research Findings#
BPC-157 animal studies in tendon and joint repair include:
- Achilles tendon transection — accelerated healing with improved biomechanical properties (tensile strength, load to failure) in rat models
- MCL (medial collateral ligament) transection — faster ligament healing with improved collagen fiber organization
- Rotator cuff tears — improved tendon-to-bone healing in rat supraspinatus detachment models
- Quadriceps tendon repair — enhanced healing in surgically damaged quadriceps tendons
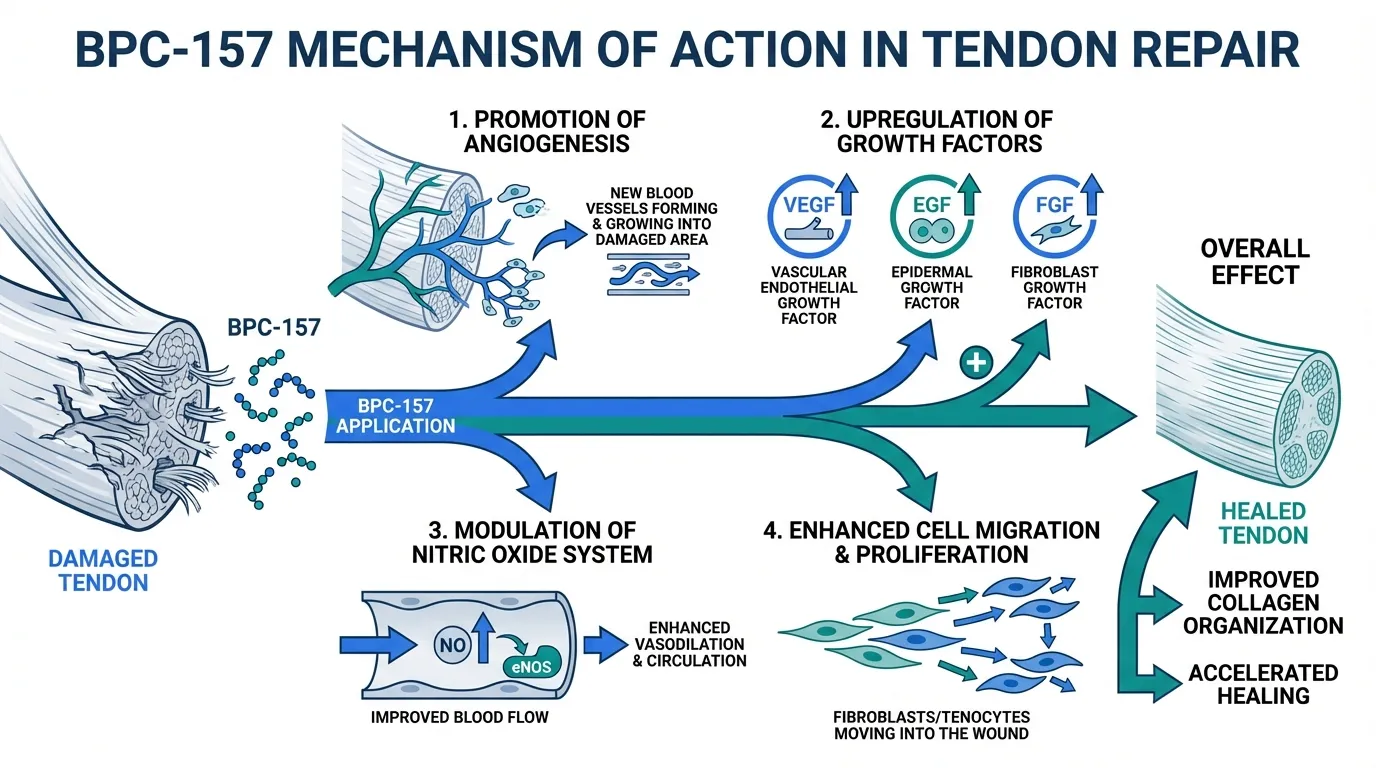
The proposed mechanism involves BPC-157's promotion of angiogenesis (new blood vessel formation) at the injury site — directly addressing the vascularity limitation of tendon healing. BPC-157 upregulates VEGF (vascular endothelial growth factor), EGF (epidermal growth factor), and FGF (fibroblast growth factor), while modulating the nitric oxide system to support blood flow to damaged tissue.
Important Considerations#
All BPC-157 tendon and joint data is from animal models, primarily in rats. No human clinical trials for musculoskeletal indications have been published. The translation from rat tendon healing to human connective tissue repair is uncertain — rats have different tendon loading patterns, healing rates, and biomechanical requirements than humans. BPC-157 was placed in FDA Category 2 in 2024. For a comprehensive review, see Best Healing Peptides.
2. TB-500 (Thymosin Beta-4 Fragment)#
Evidence Level: Preclinical; limited dermal wound healing human data (for thymosin beta-4) Primary Mechanism: Actin sequestration; cell migration; anti-inflammatory FDA Status: Category 2 (banned from compounding)
TB-500 is a synthetic peptide fragment of thymosin beta-4, a naturally occurring 43-amino-acid protein involved in cell migration, proliferation, and differentiation. TB-500's relevance to joint and tendon health centers on its role in promoting cellular repair processes in damaged connective tissue.
Research Findings#
TB-500 and its parent molecule thymosin beta-4 have been studied for tissue repair with several relevant findings:
- Cell migration — thymosin beta-4 promotes cell migration through its role in actin polymerization regulation. By sequestering G-actin monomers, it facilitates the cytoskeletal reorganization necessary for cells to migrate into wound sites
- Anti-inflammatory effects — TB-500 has demonstrated reduction in inflammatory cytokines in damaged tissue, which may create a more favorable environment for repair
- Collagen deposition — studies suggest thymosin beta-4 promotes organized collagen deposition in healing tissues, which is critical for restoring tendon and ligament structural integrity
- Corneal and dermal healing — the most advanced clinical data for thymosin beta-4 comes from ophthalmological and dermal wound healing studies (RGN-259), not musculoskeletal applications
Important Considerations#
The musculoskeletal-specific evidence for TB-500 is thinner than for BPC-157. Most joint and tendon extrapolations are based on the general wound healing properties of thymosin beta-4 rather than on studies specifically designed to evaluate tendon or ligament repair. TB-500 is also FDA Category 2. The combination of BPC-157 + TB-500 (the "Wolverine Stack") is popular but lacks published combination data — see Complete Guide to Peptide Stacks and BPC-157 vs TB-500.
3. GHK-Cu (Copper Peptide)#
Evidence Level: Extensive gene expression data; limited clinical outcomes data for musculoskeletal applications Primary Mechanism: Gene expression modulation; collagen synthesis stimulation; matrix metalloproteinase regulation FDA Status: Category 2 (injectable); available as topical ingredient
GHK-Cu is a naturally occurring tripeptide-copper complex that declines with age. While most commonly associated with skin health (see Peptides for Skin Health), GHK-Cu's gene expression profile includes pathways directly relevant to connective tissue repair and joint health.
Research Findings#
GHK-Cu's relevance to joint and tendon health comes from its broad gene expression effects:
- Collagen synthesis — GHK-Cu upregulates genes for collagen types I and III, the primary structural collagens in tendons and ligaments
- Glycosaminoglycan production — stimulates production of decorin and other proteoglycans that organize collagen fibers and provide structural integrity to connective tissue
- Matrix metalloproteinase regulation — GHK-Cu modulates MMPs that break down extracellular matrix, potentially creating a more favorable balance between tissue breakdown and repair
- Anti-inflammatory gene expression — suppression of inflammatory gene pathways that can interfere with orderly tissue repair
- Antioxidant defense — upregulation of superoxide dismutase and other protective enzymes that may protect healing tissue from oxidative damage
Important Considerations#
GHK-Cu's evidence for joint and tendon applications is primarily extrapolated from gene expression data and skin studies. Direct studies of GHK-Cu on tendon, ligament, or cartilage repair are limited. The gene expression profile is compelling but the gap between gene modulation and clinical musculoskeletal outcomes has not been bridged with controlled human studies.
4. Ipamorelin#
Evidence Level: Clinical data for GH release; indirect evidence for connective tissue benefits Primary Mechanism: Selective GH secretagogue (ghrelin receptor agonist); increases endogenous GH and IGF-1 FDA Status: Not FDA-approved; investigational
Ipamorelin approaches joint and tendon health from a different angle than the direct repair peptides above. As a selective growth hormone secretagogue, ipamorelin stimulates the body's own GH release, which in turn elevates IGF-1 — a growth factor with well-established roles in connective tissue metabolism.
Research Findings#
The rationale for ipamorelin in joint health is based on GH/IGF-1 physiology:
- GH and collagen synthesis — growth hormone and IGF-1 are known stimulators of collagen synthesis in tendons and ligaments. GH deficiency is associated with impaired connective tissue healing
- Selective profile — ipamorelin produces GH release without significant cortisol or prolactin elevation. This is relevant because cortisol is catabolic to connective tissue
- Age-related decline — GH secretion declines with age (somatopause), and this decline correlates with reduced connective tissue repair capacity. Ipamorelin may partially restore youthful GH pulsatility
- Synergy with GHRH pathway — when combined with a GHRH analog like CJC-1295 (No DAC), ipamorelin produces synergistic GH release through dual-pathway activation (see CJC-1295 + Ipamorelin Stack)
Important Considerations#
Ipamorelin has not been specifically studied for joint or tendon repair in clinical trials. The connective tissue rationale is based on the known relationship between GH/IGF-1 and collagen metabolism, not on direct evidence of ipamorelin improving joint outcomes. Growth hormone excess can also have negative effects (joint swelling, carpal tunnel syndrome), highlighting the importance of appropriate dosing. For comparisons with other GH secretagogues, see Growth Hormone Secretagogues Compared.
5. Sermorelin#
Evidence Level: Clinical data for GH stimulation; indirect evidence for connective tissue Primary Mechanism: GHRH analog; stimulates pituitary GH release through the GHRH receptor FDA Status: Previously FDA-approved (discontinued commercial production)
Sermorelin is a synthetic analog of the first 29 amino acids of growth hormone-releasing hormone (GHRH). Like ipamorelin, its relevance to joint health is indirect — through stimulation of endogenous GH release and subsequent IGF-1 elevation.
Research Findings#
Sermorelin's joint health rationale parallels ipamorelin's, with some distinctions:
- Physiological GH release — sermorelin stimulates GH in a pulsatile, physiological pattern that preserves the body's natural feedback mechanisms, reducing the risk of GH excess
- Clinical history — sermorelin was previously FDA-approved for GH-deficient children, providing a longer clinical safety track record than most research peptides
- Connective tissue support — the GH released by sermorelin stimulates hepatic IGF-1 production, which supports collagen synthesis and connective tissue metabolism through IGF-1 receptor signaling
- Shorter half-life — sermorelin's half-life (~10-20 minutes) means its effects are more transient than CJC-1295, requiring more frequent administration
Important Considerations#
Like ipamorelin, sermorelin has not been directly studied for joint or tendon repair outcomes. The connective tissue benefits are theoretical, based on GH/IGF-1 physiology. Sermorelin's commercial production was discontinued, though it remains available through compounding pharmacies. For a detailed comparison, see Ipamorelin vs Sermorelin.
How These Peptides Compare#
| Feature | BPC-157 | TB-500 | GHK-Cu | Ipamorelin | Sermorelin |
|---|---|---|---|---|---|
| Mechanism | Direct repair (growth factors, angiogenesis) | Direct repair (cell migration, actin) | Gene expression (collagen, ECM) | Indirect (GH/IGF-1 elevation) | Indirect (GH/IGF-1 elevation) |
| Tendon-Specific Data | Extensive preclinical | Limited | Gene expression only | None (GH physiology) | None (GH physiology) |
| Evidence Level | Strong preclinical | Moderate preclinical | In vitro / gene expression | Clinical (for GH release) | Clinical (for GH release) |
| FDA Status | Category 2 | Category 2 | Category 2 (injectable) | Not approved | Previously approved |
| Administration | SC injection | SC injection | Topical or SC injection | SC injection | SC injection |
| Onset of Action | Days to weeks (animal data) | Days to weeks (animal data) | Unknown for joints | Weeks to months (GH effects) | Weeks to months (GH effects) |
Complementary Approaches#
Several non-peptide strategies for joint and tendon health have established evidence bases and may complement peptide research:
- Physical therapy and progressive loading — the most evidence-based approach to tendon rehabilitation
- Collagen supplementation — oral hydrolyzed collagen with vitamin C has shown modest benefits in tendon repair studies (see Peptides for Skin Health for collagen peptide research)
- PRP (platelet-rich plasma) — growth factor-rich plasma injections with mixed clinical evidence for tendon and joint conditions
- Addressing inflammation — for inflammatory joint conditions, anti-inflammatory peptides like KPV may have theoretical relevance (see Peptides for Inflammation)
Conclusion#
Peptides for joint pain and tendon repair fall into two broad categories: direct repair peptides (BPC-157, TB-500, GHK-Cu) that target tissue healing mechanisms at the local level, and indirect support peptides (ipamorelin, sermorelin) that elevate systemic growth factors involved in connective tissue metabolism.
BPC-157 has the strongest preclinical evidence base specifically for tendon repair, though the absence of human clinical data remains a significant limitation. TB-500 complements BPC-157 through different repair mechanisms. GHK-Cu offers compelling gene expression data. The GH secretagogues provide an indirect approach based on established GH/IGF-1 physiology.
For dose calculations and further research tools, visit the Dosing Calculator and HED Calculator. For important safety information, see the Safety page.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- BPC-157 Overview and Research Guide
- BPC-157 Dosing Protocols
- BPC-157 Side Effects and Safety
- TB-500 Overview and Research Guide
- TB-500 Dosing Protocols
- TB-500 Side Effects and Safety
- GHK-Cu Overview and Research Guide
- GHK-Cu Dosing Protocols
- GHK-Cu Side Effects and Safety
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- Sermorelin Overview and Research Guide
- Sermorelin Dosing Protocols
- Sermorelin Side Effects and Safety

{kind=link}
Frequently Asked Questions About Best Peptides for Joint Pain and Tendon Repair: Research Guide
What does this article cover?
Peptides for joint pain and tendon repair — BPC-157, TB-500, GHK-Cu, ipamorelin, and sermorelin — with evidence and mechanisms. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers BPC-157, TB-500, GHK-Cu, Ipamorelin, Sermorelin. Key context: BPC-157 (Gastric pentadecapeptide with extensive preclinical data on tendon, ligament, and joint tissue re...); TB-500 (Thymosin beta-4 fragment studied for tissue repair through actin regulation and cell migration pr...); GHK-Cu (Copper peptide with gene expression data on collagen synthesis and extracellular matrix remodeling). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Best Peptides for Joint Pain and Tendon Repair: Research Guide." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Gastric pentadecapeptide with extensive preclinical data on tendon, ligament, and joint tissue re.... Thymosin beta-4 fragment studied for tissue repair through actin regulation and cell migration pr.... Copper peptide with gene expression data on collagen synthesis and extracellular matrix remodeling. These takeaways are based on the research data available at the time of publication.
What is BPC-157 and why is it significant?
BPC-157 is a peptide discussed in this article because: Gastric pentadecapeptide with extensive preclinical data on tendon, ligament, and joint tissue repair. For a complete profile of BPC-157, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.

Peptides for Athletic Recovery: Beyond BPC-157 and TB-500
A comprehensive guide to peptides researched for athletic recovery, covering BPC-157, TB-500, GH secretagogues, MGF, GHK-Cu, and DSIP. Includes WADA anti-doping considerations, evidence levels, and recovery-focused protocol rationale.
You Might Also Like
Related content you may find interesting