Ipamorelin vs Sermorelin: GH Secretagogue Comparison
Ipamorelin vs Sermorelin: Evidence-based comparison of two growth hormone secretagogues. Covers GHRP vs GHRH mechanisms, GH release profiles, clinical evidence, side effects, and synergistic combination protocols.
Verdict at a Glance
Sermorelin has stronger clinical evidence, including former FDA approval and well-established dosing protocols. Ipamorelin offers selective GH release without cortisol or prolactin stimulation. These peptides operate through complementary pathways (GHRH vs GHRP) and are frequently studied in combination for synergistic GH release greater than either alone.
| Best for | Pick | Why |
|---|---|---|
| Established clinical evidence and dosing guidance | Sermorelin | Former FDA approval provides regulatory-grade safety and dosing data that ipamorelin lacks |
| Avoiding cortisol and prolactin elevation | Ipamorelin | Does not stimulate ACTH, cortisol, or prolactin in preclinical studies, unlike some other GHRP-class peptides |
| Anti-aging and GH axis restoration | Sermorelin | Clinical studies in elderly subjects showed IGF-1 restoration and increased pituitary GH reserve |
| Maximizing GH release through combination protocols | Both | GHRH (sermorelin) plus GHRP (ipamorelin) pathways produce synergistic GH release substantially greater than either agent alone |
| Pediatric GH deficiency research | Sermorelin | FDA-approved history for pediatric GH deficiency diagnosis and treatment with sustained growth velocity data |
| Selective GH stimulation in research models | Ipamorelin | Cleanest hormonal profile among GHRP-class peptides with no ACTH or cortisol activation in animal studies |
| Category | Ipamorelin | Sermorelin | Advantage |
|---|---|---|---|
| Mechanism of Action | Selective GHS-R1a (ghrelin receptor) agonist that stimulates GH release via the PLC/PKC pathway. Does not activate ACTH or cortisol secretion, making it highly selective among GHRP-class peptides. | GHRH(1-29) analog that binds the GHRH receptor on pituitary somatotrophs, activating the cAMP/PKA pathway. Stimulates both GH release and GH gene transcription, increasing pituitary reserve. | Comparable |
| Research Evidence | Limited clinical data. Phase II trial in postoperative ileus failed its primary endpoint. No Phase III trials completed. Preclinical data shows selective GH release and bone anabolic effects. | Former FDA-approved peptide (Geref, 1997-2008). Supported by clinical studies in pediatric GH deficiency, diagnostic testing, and aging populations. Moderate evidence base with regulatory validation. | Sermorelin |
| Side Effect Profile | Phase II trial showed 87.5% TEAE rate (vs 94.8% placebo). Does not stimulate ACTH or cortisol in animal models. Limited long-term human safety data. Two fatal SAEs reported in surgical trial context. | Well-characterized safety profile from FDA-approved use. Common effects include injection site reactions, facial flushing, headache, and transient nausea. Somatostatin feedback prevents GH excess. | Sermorelin |
| Dosing Complexity | Typically studied at fixed doses via IV in clinical trials. No established human SC bioavailability data. Half-life approximately 2 hours IV. Dosing protocols are largely empirical. | Well-established dosing from FDA approval. Pediatric 30 mcg/kg SC at bedtime. Adult protocols typically 100-300 mcg SC nightly. Diagnostic dose 1 mcg/kg IV. Clear clinical guidance available. | Sermorelin |
| GH Selectivity | Highly selective for GH release without affecting cortisol, prolactin, or ACTH levels. Among GHRP-class peptides, ipamorelin shows the cleanest hormonal profile in preclinical studies. | Selective for GH via the GHRH receptor. Maintains pulsatile GH release and physiological feedback through the somatostatin axis. Does not directly affect cortisol or prolactin pathways. | Comparable |

Introduction#
Ipamorelin and sermorelin are both growth hormone secretagogues, but they operate through fundamentally different receptor pathways. Sermorelin is a synthetic GHRH(1-29) analog that stimulates GH release via the GHRH receptor on pituitary somatotrophs, while ipamorelin is a selective ghrelin receptor (GHS-R1a) agonist that triggers GH release through the growth hormone secretagogue receptor pathway. This distinction has practical implications for their pharmacological profiles, clinical evidence, and how they are used in research.
Sermorelin holds the distinction of being a formerly FDA-approved peptide (as Geref, 1997-2008), withdrawn from the market due to manufacturing difficulties rather than safety concerns. Ipamorelin progressed through Phase II clinical trials for postoperative ileus but did not advance further after failing to meet its primary endpoint. Despite different trajectories, both peptides continue to be studied as tools for stimulating endogenous GH production.
Understanding how these two peptides differ -- and how they may complement each other -- is essential for evaluating their respective roles in GH-related research.
Mechanism of Action Comparison#
Ipamorelin#
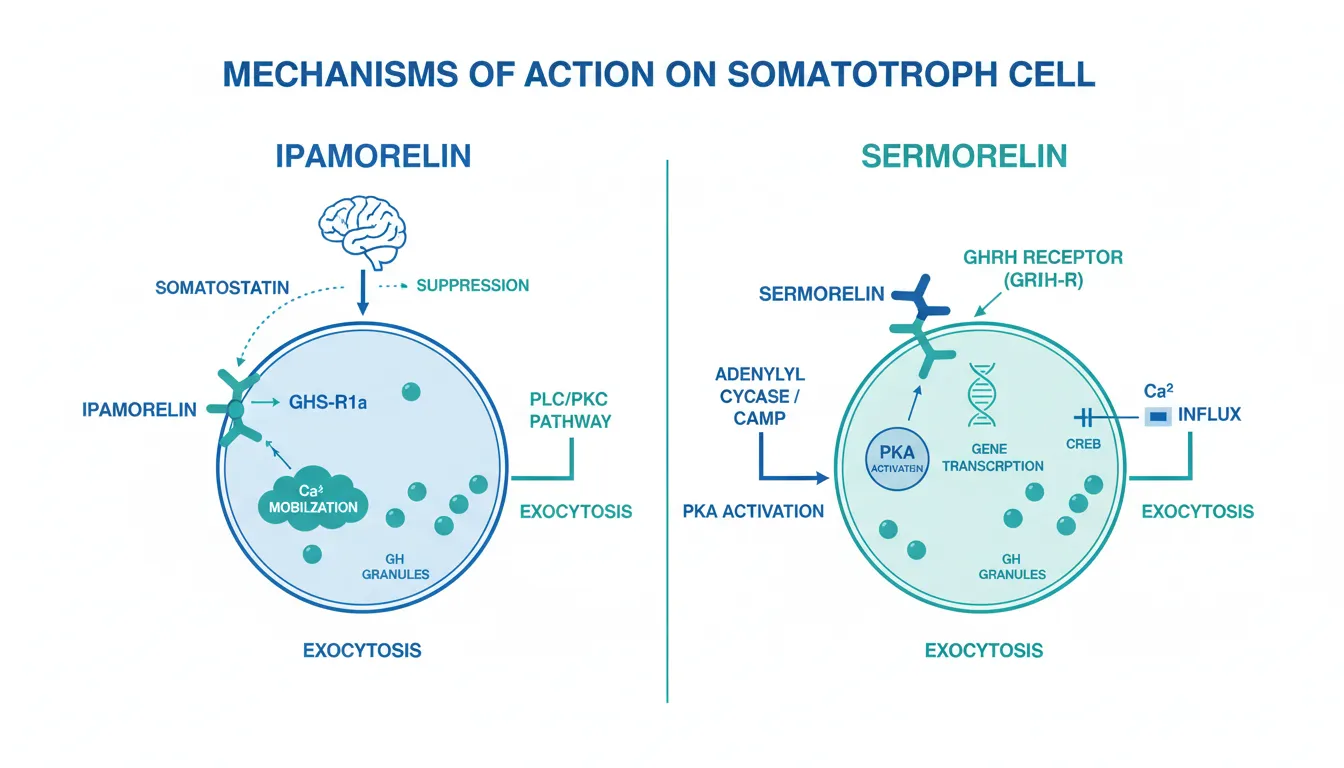
Ipamorelin is a synthetic pentapeptide that acts as a selective agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), the same receptor targeted by the endogenous hormone ghrelin. Upon binding GHS-R1a on pituitary somatotrophs, ipamorelin activates the phospholipase C (PLC) and protein kinase C (PKC) intracellular signaling cascade, leading to calcium mobilization and GH granule exocytosis.
A defining characteristic of ipamorelin is its selectivity. Unlike other GHRP-class peptides such as GHRP-6 and GHRP-2, ipamorelin does not stimulate adrenocorticotropic hormone (ACTH), cortisol, or prolactin release in preclinical studies. This selectivity profile makes it unusual among ghrelin receptor agonists and suggests a more targeted mechanism of GH stimulation.
Ipamorelin also has indirect effects through the hypothalamus, where GHS-R1a activation suppresses somatostatin release, reducing the primary inhibitory signal on GH secretion.
Sermorelin#
Sermorelin (GHRH(1-29)NH2) is the shortest synthetic fragment of growth hormone-releasing hormone that retains full biological activity at the GHRH receptor. It consists of the first 29 amino acids of the 44-amino acid native GHRH molecule.
Sermorelin binds to the GHRH receptor (GHRH-R) on anterior pituitary somatotrophs, activating adenylyl cyclase and increasing intracellular cyclic AMP (cAMP) levels. This triggers protein kinase A (PKA) activation, which phosphorylates the transcription factor CREB and upregulates GH messenger RNA transcription. Simultaneously, cAMP-mediated calcium influx through voltage-gated channels triggers release of stored GH granules.
A key distinction is that sermorelin does not merely trigger GH release -- it also stimulates GH gene transcription, increasing the pituitary's GH reserve capacity over time. The negative feedback system through somatostatin remains fully intact, meaning that rising GH and IGF-1 levels will suppress further GH release, preventing supraphysiological elevations.
Pathway Comparison#
| Feature | Ipamorelin | Sermorelin |
|---|---|---|
| Receptor target | GHS-R1a (ghrelin receptor) | GHRH-R (GHRH receptor) |
| Signaling pathway | PLC/PKC/calcium | cAMP/PKA/CREB |
| GH gene transcription | Not directly stimulated | Upregulated via CREB |
| Pituitary reserve | Not increased | Increased over chronic use |
| Somatostatin interaction | Suppresses somatostatin release | Regulated by somatostatin feedback |
| Cortisol/ACTH effect | No stimulation (preclinical) | No direct effect |
| Prolactin effect | No stimulation (preclinical) | No direct effect |
Dosing Comparison#
Ipamorelin Dosing#
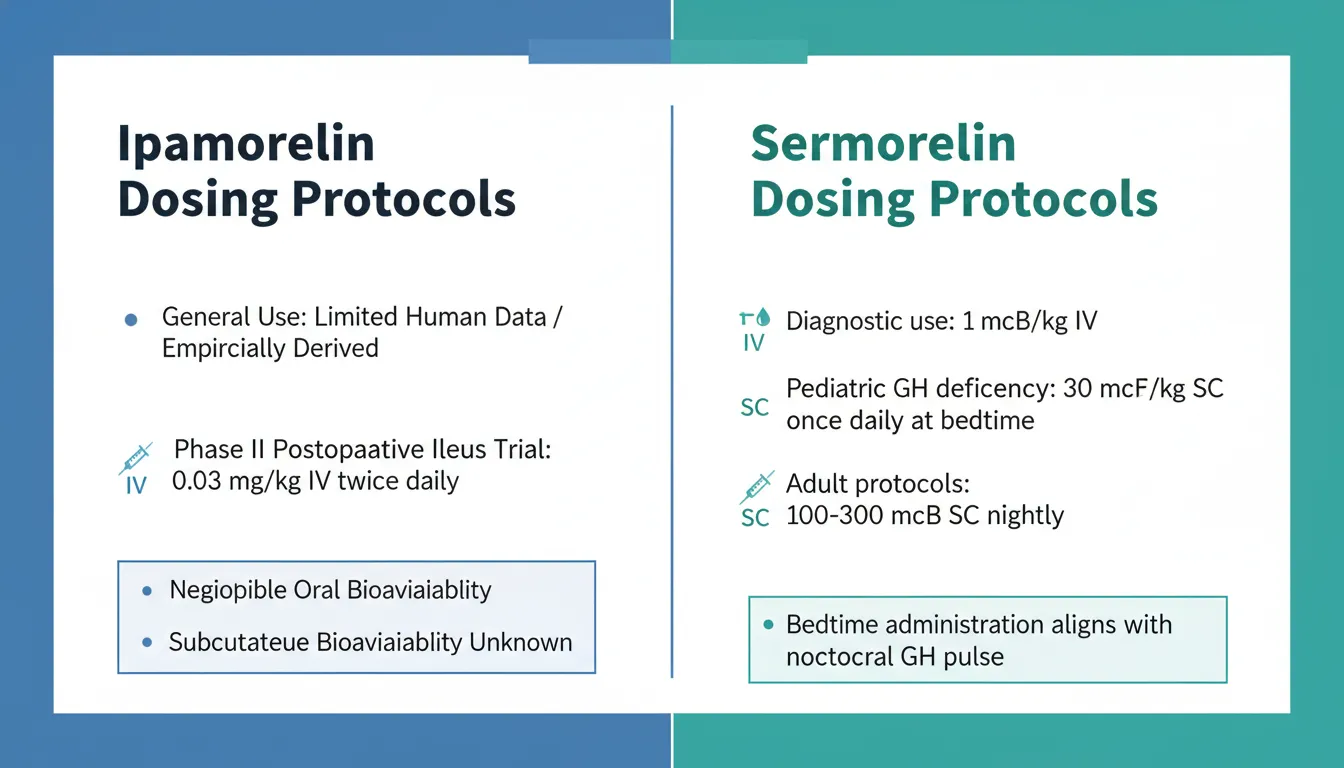
Ipamorelin dosing protocols in human clinical research are limited. In the Phase II postoperative ileus trial, ipamorelin was administered at 0.03 mg/kg IV twice daily starting from postoperative day 1 up to day 7. The intravenous half-life is approximately 2 hours based on pharmacokinetic studies.
Human subcutaneous bioavailability data have not been published, which represents a significant gap in the clinical pharmacology literature. The oral bioavailability of ipamorelin is negligible. Most current dosing protocols used outside of clinical trials are empirically derived rather than supported by published pharmacokinetic data.
Sermorelin Dosing#
Sermorelin has the most well-characterized dosing among GH secretagogues due to its former FDA-approved status:
- Diagnostic use: 1 mcg/kg IV with serial GH sampling at 15, 30, 45, and 60 minutes
- Pediatric GH deficiency: 30 mcg/kg SC once daily at bedtime
- Adult protocols: Typically 100-300 mcg SC administered nightly
The bedtime administration timing aligns with the natural nocturnal GH pulse pattern. The established clinical dosing for sermorelin provides a clear advantage in terms of evidence-based guidance compared to ipamorelin's largely empirical protocols.
Side Effects Comparison#
Ipamorelin Side Effects#
Data from the Phase II multicenter trial (n=114 safety population) reported a treatment-emergent adverse event (TEAE) rate of 87.5% with ipamorelin compared to 94.8% with placebo, in the context of post-surgical patients. Common adverse events included nausea (33.9%) and were largely attributable to the surgical setting rather than the drug itself.
Two fatal serious adverse events (anastomotic leaks) were reported in the ipamorelin arm and assessed as possibly related to treatment. Long-term safety data specific to ipamorelin in non-surgical populations are limited, though preclinical studies consistently show no stimulation of ACTH or cortisol, suggesting a favorable hormonal safety profile.
Class-related safety signals from other ghrelin receptor agonists include heart failure concerns (ibutamoren), hypotension (ulimorelin), and CYP3A4 interactions (tabimorelin). These have not been specifically reported with ipamorelin but warrant consideration as class effects.
Sermorelin Side Effects#
Sermorelin's safety profile is well characterized from its FDA-approved clinical use:
- Injection site reactions: Pain, swelling, or redness at the injection site (most common)
- Facial flushing: Transient warmth and redness, typically resolving within minutes
- Headache: Reported in clinical studies
- Nausea and dizziness: Generally mild and transient
- Metallic taste: Occasionally reported
The intact somatostatin feedback mechanism provides a built-in safety feature that prevents excessive GH elevation, distinguishing sermorelin from direct GH administration where supraphysiological levels are possible. No serious long-term safety signals emerged during sermorelin's period of FDA-approved use.
Research Evidence Comparison#
Ipamorelin Research#
The ipamorelin evidence base remains largely preclinical:
- Beck et al. (2014): Phase II multicenter RCT in postoperative ileus (n=117). No statistically significant improvement in the primary endpoint (time to first tolerated meal). Exploratory signals in open laparotomy subgroups did not reach significance.
- Venkova et al. (2009): Rat model showing repetitive dosing accelerated colonic transit and improved food intake, but these preclinical findings did not translate to human efficacy.
- Svensson et al. (2000): 12-week rat study demonstrating increased bone mineral content and cortical bone dimensions with chronic ipamorelin administration.
- Class-level meta-analysis (2016): Pooled data from 12 RCTs of ghrelin receptor agonists showed improvements in energy intake, lean body mass, and grip strength in malnourished adults, but ipamorelin-specific estimates were not isolated.
Development was discontinued after the negative Phase II results, and no Phase III trials were initiated.
Sermorelin Research#
Sermorelin has a substantially more developed evidence base:
- Prakash and Goa (1999): Comprehensive review establishing IV sermorelin at 1 mcg/kg as a specific diagnostic test for GH deficiency, and SC 30 mcg/kg/day as effective for pediatric growth promotion with sustained height velocity increases over 12 months.
- Vittone et al. (1997): Prospective study in elderly subjects showing significant IGF-1 increases by 2 weeks of nightly GHRH(1-29) administration, with concurrent increases in IGFBP-3 and GH binding protein.
- Walker (2006): Review proposing sermorelin as a better approach than rhGH for adult-onset GH insufficiency, citing preserved pituitary reserve, intact neuroendocrine feedback, and lower risk profile.
- Lanes et al. (1993): Clinical study showing sustained growth velocity increases in children with idiopathic short stature treated with daily GHRH(1-29).
- Siebert and Rao (2020): Review of GH secretagogues including sermorelin for body composition management, supporting synergistic protocols with GHRPs.
The evidence quality is moderate overall, supported by the former FDA approval but limited by the absence of large-scale randomized trials for anti-aging applications.
The Synergy Factor#
Perhaps the most important aspect of the ipamorelin-sermorelin comparison is that these peptides are not necessarily competitors but potential complements. Research consistently shows that co-administration of a GHRH agonist and a GHRP agonist produces GH release substantially greater than either agent alone.
This synergy operates through multiple mechanisms:
- Complementary signaling: Sermorelin activates cAMP/PKA while ipamorelin activates PLC/PKC, and both pathways converge on calcium mobilization for GH exocytosis
- Somatostatin suppression: Ipamorelin (via GHS-R1a) suppresses hypothalamic somatostatin release, while sermorelin's effects are regulated by somatostatin -- reducing this brake enhances sermorelin's action
- GH synthesis plus release: Sermorelin increases GH gene transcription and pituitary reserve, while ipamorelin triggers release of the accumulated GH stores
The combined GHRH + GHRP approach is a well-documented strategy in growth hormone secretagogue research, and the ipamorelin-sermorelin combination specifically has gained attention due to ipamorelin's clean hormonal profile (no cortisol or prolactin stimulation) paired with sermorelin's established clinical track record.
Key Differences Summary#
| Feature | Ipamorelin | Sermorelin |
|---|---|---|
| Peptide class | GHRP (ghrelin receptor agonist) | GHRH analog |
| Amino acids | 5 (pentapeptide) | 29 |
| Receptor | GHS-R1a | GHRH-R |
| Regulatory history | Phase II only (discontinued) | Former FDA approval (Geref) |
| Evidence level | Low (primarily preclinical) | Moderate (clinical studies, FDA approval) |
| GH pulsatility | Triggers acute GH pulse | Maintains physiological pulsatile pattern |
| Pituitary reserve | Not increased | Increased via GH mRNA upregulation |
| Cortisol stimulation | None (preclinical) | None |
| Prolactin stimulation | None (preclinical) | None |
| Established human dosing | No (empirical protocols) | Yes (FDA-established) |
| Half-life (IV) | ~2 hours | Short (minutes) |
| Primary research focus | GI motility, bone anabolism | GH deficiency, anti-aging |
Conclusion#
Sermorelin holds clear advantages in clinical evidence and regulatory history. As a formerly FDA-approved peptide with established dosing protocols, well-characterized safety data, and demonstrated efficacy in pediatric GH deficiency and aging populations, it represents the more thoroughly validated option. Its ability to increase pituitary GH reserve through gene transcription upregulation provides a mechanistic advantage for sustained GH axis support.
Ipamorelin's primary strengths lie in its exceptional selectivity for GH release without cortisol or prolactin stimulation, and its role as a complementary pathway in combination protocols. However, its clinical development stalled at Phase II with a negative primary outcome, leaving its evidence base substantially below that of sermorelin.
For researchers and clinicians, the combination of both peptides may represent the most promising application, leveraging sermorelin's GHRH pathway to build pituitary reserve while using ipamorelin's GHRP pathway to augment GH release. This synergistic approach, targeting two distinct receptor systems simultaneously, consistently produces greater GH responses than either peptide alone in research settings.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Established clinical evidence and dosing guidance
Sermorelin
Former FDA approval provides regulatory-grade safety and dosing data that ipamorelin lacks
Avoiding cortisol and prolactin elevation
Ipamorelin
Does not stimulate ACTH, cortisol, or prolactin in preclinical studies, unlike some other GHRP-class peptides
Anti-aging and GH axis restoration
Sermorelin
Clinical studies in elderly subjects showed IGF-1 restoration and increased pituitary GH reserve
Maximizing GH release through combination protocols
Both
GHRH (sermorelin) plus GHRP (ipamorelin) pathways produce synergistic GH release substantially greater than either agent alone
Pediatric GH deficiency research
Sermorelin
FDA-approved history for pediatric GH deficiency diagnosis and treatment with sustained growth velocity data
Selective GH stimulation in research models
Ipamorelin
Cleanest hormonal profile among GHRP-class peptides with no ACTH or cortisol activation in animal studies
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Ipamorelin vs Sermorelin: GH Secretagogue Comparison
Which is better, Ipamorelin or Sermorelin?
Sermorelin has stronger clinical evidence, including former FDA approval and well-established dosing protocols. Ipamorelin offers selective GH release without cortisol or prolactin stimulation. These peptides operate through complementary pathways (GHRH vs GHRP) and are frequently studied in combination for synergistic GH release greater than either alone. Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Ipamorelin and Sermorelin?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Sermorelin; Side Effect Profile: advantage goes to Sermorelin. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Sermorelin over Ipamorelin?
For the scenario of "Established clinical evidence and dosing guidance," research data suggests Sermorelin may be more relevant. Former FDA approval provides regulatory-grade safety and dosing data that ipamorelin lacks. This is based on currently available evidence and individual circumstances may differ.
How do Ipamorelin and Sermorelin differ in their mechanisms of action?
Ipamorelin: Selective GHS-R1a (ghrelin receptor) agonist that stimulates GH release via the PLC/PKC pathway. Does not activate ACTH or cortisol secretion, making it highly selective among GHRP-class peptides.. Sermorelin: GHRH(1-29) analog that binds the GHRH receptor on pituitary somatotrophs, activating the cAMP/PKA pathway. Stimulates both GH release and GH gene transcription, increasing pituitary reserve..
Which has fewer side effects, Ipamorelin or Sermorelin?
In terms of side effects and tolerability, the advantage goes to Sermorelin. Ipamorelin: Phase II trial showed 87.5% TEAE rate (vs 94.8% placebo). Does not stimulate ACTH or cortisol in animal models. Limited long-term human safety data.... Sermorelin: Well-characterized safety profile from FDA-approved use. Common effects include injection site reactions, facial flushing, headache, and transient ....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.