Top 6 Growth Hormone Secretagogues Compared

Introduction#
Growth hormone secretagogues (GHSs) are peptides that stimulate the pituitary gland to release endogenous growth hormone (GH). Unlike exogenous GH replacement, secretagogues work with the body's own hormonal feedback systems, preserving the natural pulsatile pattern of GH release and the hypothalamic-pituitary axis regulatory mechanisms.
These peptides operate through two primary pathways: the growth hormone-releasing hormone (GHRH) pathway and the ghrelin/GHS receptor pathway. Understanding how each secretagogue interacts with these pathways is essential for evaluating their respective research profiles, side effects, and potential applications.
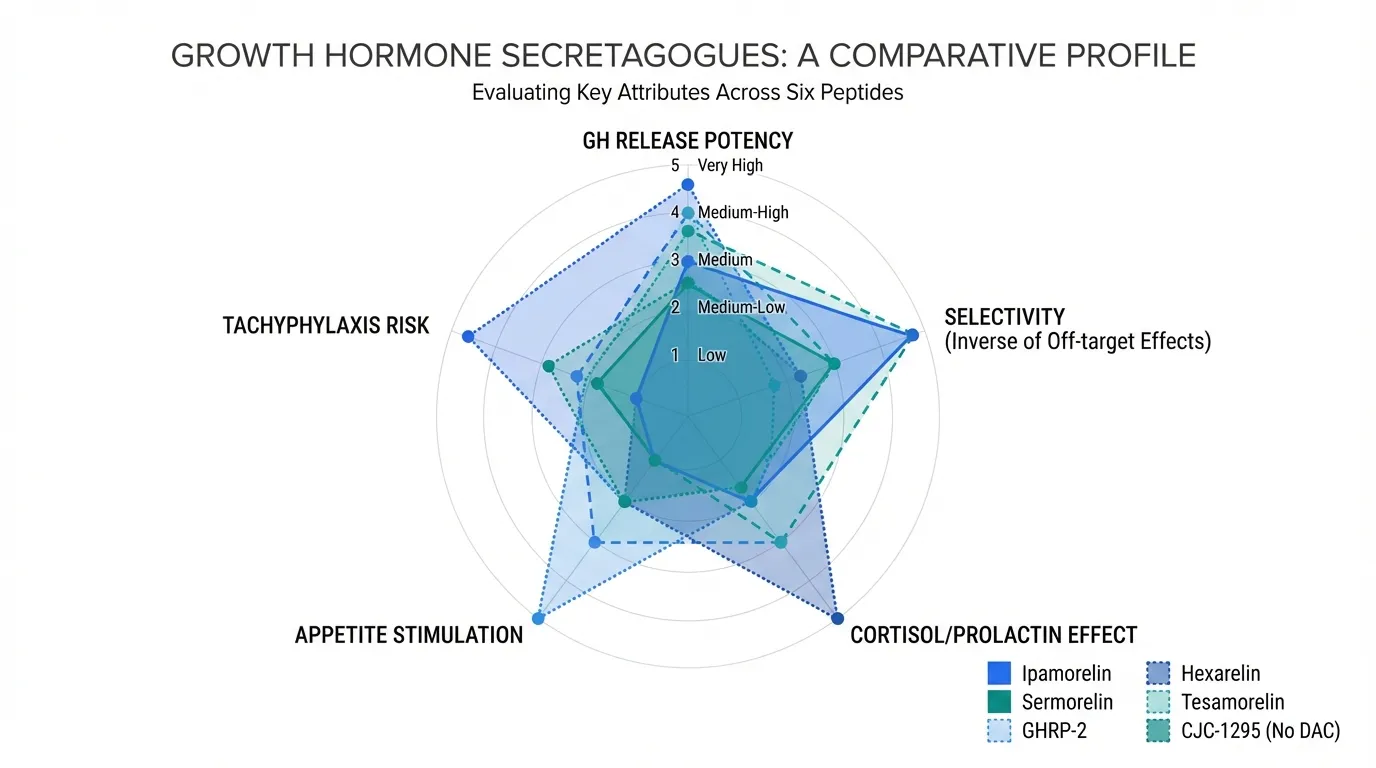
This guide compares six of the most studied GH secretagogues — ipamorelin, sermorelin, GHRP-2, hexarelin, tesamorelin, and CJC-1295 (No DAC) — across their mechanisms, selectivity, research evidence, and side effect profiles. For a visual comparison of their half-lives, see the Half-Life Comparison Tool.
Understanding the Two Pathways#
Before comparing individual peptides, it helps to understand the two signaling pathways involved in stimulating growth hormone release.
GHRH Pathway#
The GHRH receptor (GHRH-R) is located on somatotroph cells in the anterior pituitary. When GHRH binds to this receptor, it triggers GH synthesis and secretion. GHRH-pathway peptides (sermorelin, tesamorelin, CJC-1295) mimic or enhance this natural signaling cascade.
Ghrelin / GHS-R1a Pathway#
The growth hormone secretagogue receptor (GHS-R1a), also known as the ghrelin receptor, provides a separate mechanism for GH release. When activated, it amplifies GH secretion and can work synergistically with GHRH signaling. Ghrelin-pathway peptides (ipamorelin, GHRP-2, hexarelin) bind to this receptor.
The two pathways are complementary. Research suggests that combining a GHRH-pathway peptide with a ghrelin-pathway peptide produces synergistic GH release greater than either alone — a principle underlying many combination protocols studied in the literature.
1. Ipamorelin#
Pathway: Ghrelin / GHS-R1a Evidence Level: Phase 2 clinical trials Key Advantage: High selectivity — minimal cortisol, prolactin, and ACTH elevation
Ipamorelin is a pentapeptide that selectively activates the GHS-R1a receptor to stimulate GH release. It is distinguished from other ghrelin-receptor agonists by its unusually clean hormonal profile.
Research Highlights#
In clinical studies, ipamorelin demonstrated dose-dependent GH release without significant changes in cortisol, prolactin, FSH, LH, or TSH levels. A Phase 2 trial in patients recovering from abdominal surgery showed improved postoperative bowel function, though the primary focus was GH-mediated recovery effects.
Studies directly comparing ipamorelin to GHRP-2 and GHRP-6 found that ipamorelin produced similar GH release but with significantly less elevation of ACTH and cortisol. This selectivity makes it one of the most frequently studied secretagogues for protocols where minimizing side effects is a priority.
Side Effect Profile#
Ipamorelin is generally well-tolerated in published studies. The most common reported effects include mild headache, transient flushing, and injection site reactions. Unlike GHRP-2 and hexarelin, it does not produce significant appetite stimulation at standard research doses.
For a detailed head-to-head comparison, see Ipamorelin vs Sermorelin.
2. Sermorelin#
Pathway: GHRH Evidence Level: Previously FDA-approved; extensive clinical data Key Advantage: Physiological GH release pattern; long clinical track record
Sermorelin is a synthetic analog of the first 29 amino acids of endogenous GHRH (GRF 1-29). It was previously FDA-approved as Geref for diagnostic evaluation and treatment of GH deficiency in children, though it was withdrawn from the market for commercial reasons — not safety concerns.
Research Highlights#
Sermorelin has one of the longest clinical track records of any GH secretagogue. Studies in GH-deficient adults have demonstrated increased IGF-1 levels, improved body composition, and enhanced sleep quality. A notable 1997 study found that sermorelin administration increased GH secretion in elderly subjects, suggesting partial reversal of age-related somatopause.
Because sermorelin works through the GHRH receptor, the resulting GH release follows the body's natural pulsatile pattern. The pituitary's negative feedback mechanisms remain intact, which limits the risk of supraphysiological GH levels.
Side Effect Profile#
Sermorelin's side effects in clinical studies were generally mild: injection site reactions, facial flushing, and occasional headache. Because it does not activate the ghrelin receptor, it does not stimulate appetite or significantly elevate cortisol or prolactin.
Limitation#
Sermorelin has a short half-life (approximately 10-20 minutes), which means its GH-stimulating window is brief. This has led many researchers to favor longer-acting GHRH analogs like CJC-1295 or to combine sermorelin with ghrelin-pathway peptides.
3. GHRP-2#
Pathway: Ghrelin / GHS-R1a Evidence Level: Extensive clinical research; not FDA-approved Key Advantage: Potent, reliable GH release
GHRP-2 (growth hormone-releasing peptide-2) is a synthetic hexapeptide that binds to the GHS-R1a receptor with high affinity. It is one of the most potent GH secretagogues studied, producing robust and reproducible GH release across published trials.
Research Highlights#
GHRP-2 has been studied in numerous clinical settings. It produces strong, dose-dependent GH release that is amplified when combined with GHRH-pathway peptides. Studies in both healthy volunteers and GH-deficient populations have demonstrated consistent efficacy.
Research in aging populations has shown that GHRP-2 can partially restore the blunted GH response associated with aging, though the magnitude of response decreases with age compared to younger subjects.
Side Effect Profile#
GHRP-2 is less selective than ipamorelin. It produces moderate increases in cortisol and prolactin, particularly at higher doses. It also stimulates appetite through the ghrelin receptor — a significant consideration in research design. Some studies have reported transient water retention and mild gastrointestinal effects.
Compared to Ipamorelin#
GHRP-2 produces stronger peak GH release than ipamorelin in most comparative studies, but at the cost of greater hormonal side effects. The choice between the two in research contexts typically comes down to whether maximal GH output or minimal off-target effects is the priority.
4. Hexarelin#
Pathway: Ghrelin / GHS-R1a Evidence Level: Extensive clinical research; not FDA-approved Key Advantage: Highest potency GH release among GHS-R1a agonists
Hexarelin is a synthetic hexapeptide and one of the earliest GH secretagogues developed. It produces the strongest acute GH release of any peptide in this class, but also carries the most pronounced side effect profile.
Research Highlights#
Hexarelin produces potent GH release in both healthy volunteers and GH-deficient subjects. A notable finding from the research literature is hexarelin's cardioprotective properties — it has been shown to bind to cardiac receptors (CD36) independently of its GH-releasing effects. Studies suggest it may have direct cardiovascular benefits through mechanisms separate from the GH axis.
However, hexarelin is also the secretagogue most prone to tachyphylaxis (reduced response with repeated dosing). Studies have demonstrated significant desensitization of the GH response within weeks of continuous use, which limits its utility for sustained protocols.
Side Effect Profile#
Hexarelin produces significant increases in cortisol, prolactin, and ACTH — more so than GHRP-2 or ipamorelin. These hormonal effects are dose-dependent and represent the primary limitation of this compound. Appetite stimulation is also more pronounced than with other GHS-R1a agonists.
5. Tesamorelin#
Pathway: GHRH Evidence Level: FDA-approved (Egrifta) Key Advantage: Only FDA-approved GH secretagogue; strong clinical evidence base
Tesamorelin is a synthetic GHRH analog approved by the FDA under the brand name Egrifta for the treatment of HIV-associated lipodystrophy (excess abdominal fat). It is the only GH secretagogue with full FDA approval for a therapeutic indication.
Research Highlights#
Tesamorelin's clinical program includes large randomized controlled trials demonstrating significant reductions in visceral adipose tissue (VAT) in HIV patients. Studies showed approximately 15-18% reduction in trunk fat over 26 weeks of treatment compared to placebo.
Beyond its approved indication, research suggests tesamorelin may have broader metabolic benefits. Studies have explored its effects on liver fat (NAFLD), cognitive function in aging adults, and body composition in non-HIV populations. A study in older adults demonstrated improvements in verbal memory and executive function, suggesting potential cognitive benefits mediated through GH/IGF-1 signaling.
Side Effect Profile#
In FDA-approved clinical trials, the most common side effects were injection site reactions (erythema, pruritus, pain), arthralgia, myalgia, and peripheral edema. These were generally mild to moderate. Tesamorelin carries label warnings regarding potential effects on glucose metabolism and the theoretical risk of promoting growth of pre-existing malignancies (a class concern for all GH-promoting agents).
6. CJC-1295 (No DAC) / Modified GRF 1-29#
Pathway: GHRH Evidence Level: Limited clinical data; primarily preclinical Key Advantage: Improved stability over sermorelin; often used in combination protocols
CJC-1295 (No DAC), also known as Modified GRF 1-29 or Mod GRF 1-29, is a synthetic analog of GHRH with four amino acid substitutions that improve its resistance to enzymatic degradation. This gives it a longer effective half-life than sermorelin (estimated at 30+ minutes vs. 10-20 minutes) while still preserving pulsatile GH release.
Research Highlights#
The modified GRF 1-29 sequence was designed to address sermorelin's rapid degradation by DPP-IV and other enzymes. While direct clinical trial data for the no-DAC version is more limited than for sermorelin or tesamorelin, its mechanism of action through the GHRH receptor is well-established.
CJC-1295 (No DAC) is most frequently studied in combination with ghrelin-pathway peptides like ipamorelin. The rationale is that concurrent GHRH-receptor and GHS-R1a activation produces synergistic GH release — a phenomenon well-documented in studies combining GHRH analogs with ghrelin-receptor agonists.
Important Distinction: DAC vs. No DAC#
CJC-1295 exists in two forms. The DAC (Drug Affinity Complex) version binds to albumin, extending its half-life to approximately 6-8 days. This creates sustained, non-pulsatile GH elevation. The No DAC version has a shorter half-life that preserves pulsatile GH release patterns. Most research protocols favor the No DAC version for this reason, as maintaining the body's natural GH pulse frequency is considered physiologically preferable.
For more details on this distinction, see CJC-1295 DAC.
Head-to-Head Comparison#
| Feature | Ipamorelin | Sermorelin | GHRP-2 | Hexarelin | Tesamorelin | CJC-1295 (No DAC) |
|---|---|---|---|---|---|---|
| Pathway | GHS-R1a | GHRH | GHS-R1a | GHS-R1a | GHRH | GHRH |
| GH Release Potency | Moderate | Moderate | High | Very High | Moderate-High | Moderate |
| Selectivity | Very High | High | Moderate | Low | High | High |
| Cortisol Effect | Minimal | Minimal | Moderate | Significant | Minimal | Minimal |
| Prolactin Effect | Minimal | Minimal | Moderate | Significant | Minimal | Minimal |
| Appetite Stimulation | Low | None | Moderate | High | None | None |
| Tachyphylaxis Risk | Low | Low | Moderate | High | Low | Low |
| FDA Status | Not approved | Previously approved | Not approved | Not approved | Approved (Egrifta) | Not approved |
| Human Trial Data | Phase 2 | Extensive | Extensive | Extensive | Phase 3 (approved) | Limited |
| Half-Life | ~2 hours | ~10-20 min | ~15-30 min | ~20-30 min | ~26 min | ~30+ min |
How to Choose: Research Considerations#
Selectivity Priority#
For research protocols prioritizing minimal off-target hormonal effects, ipamorelin stands out among ghrelin-pathway peptides, while sermorelin and tesamorelin offer clean profiles through the GHRH pathway. The Dosing Calculator can assist with weight-based calculations for research protocols.
Maximum GH Output#
If peak GH release is the primary research endpoint, hexarelin produces the highest acute response, followed by GHRP-2. However, hexarelin's tachyphylaxis and broader hormonal effects limit its utility for sustained protocols.
Clinical Validation#
Tesamorelin offers the strongest clinical evidence base with FDA approval and large randomized controlled trials. For researchers requiring the most validated compound, tesamorelin provides the highest standard of human evidence.
Combination Protocols#
The most studied combination approach pairs a GHRH-pathway peptide with a ghrelin-pathway peptide — most commonly CJC-1295 (No DAC) + ipamorelin. Research suggests this combination produces synergistic GH release while preserving ipamorelin's favorable selectivity profile.
Regulatory Note#
Tesamorelin (Egrifta) is the only FDA-approved GH secretagogue, and only for HIV-associated lipodystrophy. Sermorelin was previously FDA-approved but has been withdrawn from the market. All other secretagogues in this guide remain investigational compounds not approved by the FDA for any indication. CJC-1295 (both DAC and No DAC versions) was placed under increased regulatory scrutiny following the 2024 FDA compounding restrictions.
Conclusion#
Growth hormone secretagogues represent a diverse class of peptides with significantly different profiles despite sharing the common goal of stimulating endogenous GH release. The two-pathway framework — GHRH receptor vs. ghrelin receptor — provides the foundation for understanding why these peptides differ in their selectivity, potency, and side effect profiles.
Ipamorelin offers the cleanest ghrelin-pathway activation. Sermorelin provides a long clinical track record through the GHRH pathway. GHRP-2 delivers potent but less selective GH release. Hexarelin is the most powerful but carries the most side effects and desensitization risk. Tesamorelin stands alone as the only FDA-approved option with rigorous Phase 3 data. And CJC-1295 (No DAC) serves as the preferred GHRH analog for combination protocols.
For researchers evaluating these compounds, the choice depends on the specific research question: whether the priority is selectivity, potency, clinical validation, or synergistic combination potential. As always, the quality of evidence varies across these peptides, and researchers should evaluate the primary literature for each compound in their specific context of interest.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- Sermorelin Overview and Research Guide
- Sermorelin Dosing Protocols
- Sermorelin Side Effects and Safety
- GHRP-2 Overview and Research Guide
- GHRP-2 Dosing Protocols
- GHRP-2 Side Effects and Safety
- Hexarelin Overview and Research Guide
- Hexarelin Dosing Protocols
- Hexarelin Side Effects and Safety
- Tesamorelin Overview and Research Guide
- Tesamorelin Dosing Protocols
- Tesamorelin Side Effects and Safety
- CJC-1295 (No DAC) Overview and Research Guide
- CJC-1295 (No DAC) Dosing Protocols
- CJC-1295 (No DAC) Side Effects and Safety

{kind=link}
Frequently Asked Questions About Top 6 Growth Hormone Secretagogues Compared
What does this article cover?
Compare 6 growth hormone secretagogues — ipamorelin, sermorelin, GHRP-2, hexarelin, tesamorelin, and CJC-1295 — by mechanism and side effects. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Ipamorelin, Sermorelin, GHRP-2, Hexarelin, Tesamorelin, CJC-1295 (No DAC). Key context: Ipamorelin (Selective GHS-R1a agonist known for minimal cortisol and prolactin elevation); Sermorelin (GHRH analog that stimulates GH release through the GHRH receptor pathway); GHRP-2 (Potent ghrelin receptor agonist with robust GH release but broader hormonal effects). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Top 6 Growth Hormone Secretagogues Compared." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Selective GHS-R1a agonist known for minimal cortisol and prolactin elevation. GHRH analog that stimulates GH release through the GHRH receptor pathway. Potent ghrelin receptor agonist with robust GH release but broader hormonal effects. These takeaways are based on the research data available at the time of publication.
What is Ipamorelin and why is it significant?
Ipamorelin is a peptide discussed in this article because: Selective GHS-R1a agonist known for minimal cortisol and prolactin elevation. For a complete profile of Ipamorelin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?
A beginner-friendly guide to growth hormone secretagogues including ipamorelin, sermorelin, CJC-1295, and more. Learn how GH peptides work, compare options, and understand which secretagogue may fit your research goals.
Best Growth Hormone Peptides Ranked: 2026 Evidence-Based Guide
A ranked comparison of 8 growth hormone secretagogues and related peptides — from FDA-approved tesamorelin to IGF-1 LR3 — evaluating each on mechanism of action, clinical evidence strength, key advantages, and known drawbacks.

CJC-1295 + Ipamorelin Stack: Growth Hormone Secretagogue Research Guide
An evidence-based review of the CJC-1295 (no DAC) and ipamorelin peptide stack, examining clinical research on growth hormone stimulation, the rationale for combining GHRH and GHRP pathways, and key limitations.
You Might Also Like
Related content you may find interesting