What Is Peptide Therapy? A Complete Guide to Peptide-Based Treatments

Introduction#
Peptide therapy refers to the medical and research use of short-chain amino acid sequences -- known as peptides -- to target specific biological pathways in the body. These compounds, typically ranging from 2 to 50 amino acids in length, occupy a unique pharmacological space between small-molecule drugs and large biologic proteins. They can be highly selective for their target receptors, are often well-tolerated, and can modulate complex physiological processes including metabolism, hormone regulation, tissue repair, immune function, and cellular aging.
The field has a long history. Since the isolation of insulin in 1921 -- arguably the first therapeutic peptide -- researchers have identified, synthesized, and developed peptides for an expanding range of clinical applications. As of 2025, over 80 peptide-based drugs have received FDA approval, with hundreds more in clinical trials across therapeutic areas from oncology to metabolic disease to rare genetic disorders. The recent success of GLP-1 receptor agonists like semaglutide and tirzepatide for weight management and diabetes has brought peptide therapy into mainstream medical awareness on an unprecedented scale.
This guide covers what peptides are, how peptide therapy works, the major categories of therapeutic peptides, FDA-approved peptide drugs, the current state of clinical research, safety considerations, and how to evaluate the evidence behind peptide-based treatments.
What Are Peptides?#
Peptides are molecules composed of amino acids linked together by peptide bonds. While proteins are typically defined as having 50 or more amino acids, peptides are shorter chains -- generally between 2 and 50 amino acids. This distinction matters pharmacologically because peptides are small enough to be synthesized chemically (rather than requiring biological expression systems), yet large enough to interact with specific receptors with high selectivity.
The human body produces hundreds of endogenous peptides that serve as hormones, neurotransmitters, and signaling molecules. Examples include:
- Insulin (51 amino acids) -- regulates blood glucose
- Oxytocin (9 amino acids) -- involved in social bonding and uterine contractions
- GLP-1 (30 amino acids) -- stimulates insulin secretion and suppresses appetite
- Growth hormone-releasing hormone (GHRH) (44 amino acids) -- triggers growth hormone release from the pituitary
- GHK-Cu (3 amino acids) -- a naturally occurring copper-binding tripeptide involved in wound healing and tissue remodeling
Therapeutic peptides are either synthetic copies of these natural molecules, modified analogs designed for improved pharmacological properties (longer half-life, greater receptor selectivity, enhanced stability), or entirely novel sequences engineered to interact with specific biological targets. For a more detailed introduction to peptide biology, see our guide on what are peptides.
How Does Peptide Therapy Work?#
Peptide therapy works by introducing specific peptide sequences into the body to modulate targeted biological pathways. Unlike many small-molecule drugs that may interact with multiple targets and produce broad systemic effects, peptides tend to bind to specific receptors with high affinity, producing more focused biological responses.
Mechanisms of Action#
Different peptide therapies operate through distinct mechanisms depending on their target:
Receptor agonism -- Many therapeutic peptides mimic the action of endogenous hormones by binding to and activating their receptors. Semaglutide activates the GLP-1 receptor to stimulate insulin secretion and suppress appetite. Tirzepatide activates both GIP and GLP-1 receptors simultaneously for enhanced metabolic effects. These receptor agonists are among the most clinically successful peptide therapeutics.
Endogenous hormone stimulation -- Rather than replacing a hormone directly, some peptides stimulate the body's own production. Growth hormone secretagogues like ipamorelin act on the ghrelin receptor (GHS-R1a) in the pituitary gland to trigger the release of endogenous growth hormone, preserving the body's natural feedback regulation.
Enzyme modulation -- Some peptides influence cellular processes by modulating enzyme activity. Epitalon, for example, has been studied for its ability to activate telomerase, the enzyme responsible for maintaining telomere length at chromosome ends.
Growth factor signaling -- Peptides can upregulate or modulate growth factor pathways involved in tissue repair. BPC-157 has been studied in preclinical models for its ability to promote angiogenesis and upregulate VEGF, EGF, and other growth factor receptors.
Gene expression modulation -- Some peptides influence the expression of large numbers of genes. GHK-Cu has been shown in gene expression studies to modulate over 4,000 human genes involved in tissue remodeling, antioxidant defense, and anti-inflammatory processes.
Routes of Administration#
Peptide therapies are administered through several routes depending on the specific compound and its pharmacological properties:
| Route | Examples | Advantages | Limitations |
|---|---|---|---|
| Subcutaneous injection | Semaglutide, tirzepatide, ipamorelin | High bioavailability, controlled dosing | Requires injection, patient training |
| Oral | Oral semaglutide (Rybelsus) | Patient convenience, no needles | Lower bioavailability, requires specific conditions |
| Topical | GHK-Cu creams and serums | Non-invasive, targeted delivery | Limited to skin and superficial tissues |
| Intranasal | Oxytocin, some neuropeptides | Bypasses blood-brain barrier partially | Variable absorption |
| Intravenous | Some clinical peptides | 100% bioavailability | Requires clinical setting |
Most research peptides and newer therapeutic peptides are administered via subcutaneous injection. The development of oral peptide formulations is an active area of pharmaceutical research, with oral semaglutide (Rybelsus, and more recently an oral formulation of Wegovy approved in late 2025) representing a significant milestone in the field.
Major Categories of Peptide Therapy#
Therapeutic peptides span several major categories, each defined by their primary biological target. For a detailed exploration of these categories, see our understanding peptide categories guide.
Metabolic Peptides#
Metabolic peptides regulate energy metabolism, glucose homeostasis, and body weight. This category has seen the most dramatic clinical success, driven by GLP-1 receptor agonists and their multi-receptor successors.
FDA-approved examples:
- Semaglutide (Ozempic, Wegovy, Rybelsus) -- GLP-1 receptor agonist for type 2 diabetes and obesity
- Tirzepatide (Mounjaro, Zepbound) -- dual GIP/GLP-1 receptor agonist for type 2 diabetes and obesity
- Liraglutide (Victoza, Saxenda) -- GLP-1 receptor agonist for diabetes and weight management
In clinical trials:
- Retatrutide -- triple GIP/GLP-1/glucagon receptor agonist (Phase 3), demonstrating up to 24.2% body weight reduction in Phase 2 trials
- Survodutide -- dual glucagon/GLP-1 agonist (Phase 3), with particular promise for liver disease (MASH)
The metabolic peptide category illustrates how peptide therapy has progressed from single-receptor approaches to multi-receptor agonism, with each additional receptor target providing complementary biological effects.
Growth Hormone Secretagogues#
Growth hormone secretagogues (GHSs) stimulate the pituitary gland to release endogenous growth hormone. Unlike exogenous growth hormone replacement, these peptides work with the body's own hormonal feedback systems.
FDA-approved examples:
- Tesamorelin (Egrifta) -- GHRH analog approved for HIV-associated lipodystrophy
Investigational examples:
- Ipamorelin -- selective GHS-R1a agonist (Phase 2), notable for stimulating GH release without significantly elevating cortisol or prolactin
- Sermorelin -- GHRH analog studied for GH deficiency
- GHRP-2 and GHRP-6 -- earlier-generation ghrelin receptor agonists
Healing and Tissue Repair Peptides#
Healing peptides accelerate tissue repair processes through mechanisms including angiogenesis promotion, growth factor upregulation, and anti-inflammatory modulation.
Notable research compounds:
- BPC-157 -- a 15-amino acid peptide derived from human gastric juice proteins, studied in over 100 preclinical studies across multiple tissue types (gastrointestinal, musculoskeletal, neurological)
- TB-500 -- active fragment of thymosin beta-4, studied for cell migration and tissue repair
- GHK-Cu -- copper-binding tripeptide with applications in wound healing and dermatology
A critical distinction in this category is that most healing peptides remain in preclinical research. While the breadth and consistency of preclinical data for compounds like BPC-157 is substantial, no completed randomized controlled human clinical trials have been published for many of these compounds.
Anti-Aging Peptides#
Anti-aging peptides target fundamental mechanisms of cellular aging, including telomere attrition, senescent cell accumulation, and declining repair capacity.
Notable research compounds:
- Epitalon -- synthetic tetrapeptide studied for telomerase activation and lifespan extension in animal models
- FOXO4-DRI -- senolytic peptide that disrupts FOXO4-p53 interactions in senescent cells
- SS-31 (Elamipretide) -- synthetic mitochondrial-targeted peptide in Phase 3 clinical trials for Barth syndrome (approved in 2025 by FDA)
Neuropeptides and Cognitive Peptides#
Neuropeptides modulate brain function, stress response, and cognitive performance.
Notable examples:
- Selank -- synthetic analog of the immunomodulatory peptide tuftsin, studied for anxiolytic and nootropic effects
- Semax -- synthetic analog of ACTH(4-10), studied for cognitive enhancement and neuroprotection
- Cerebrolysin -- a peptide preparation approved in some countries for stroke and cognitive disorders
Reproductive and Hormonal Peptides#
These peptides regulate reproductive hormones and sexual function.
FDA-approved examples:
- Gonadorelin -- GnRH analog used for diagnostic testing and fertility treatment
- Triptorelin -- GnRH agonist used in prostate cancer and endometriosis
- PT-141 (bremelanotide, Vyleesi) -- melanocortin receptor agonist approved for hypoactive sexual desire disorder
FDA-Approved Peptide Therapeutics#
The number of FDA-approved peptide drugs has grown steadily over the past several decades. Over 80 peptide-based drugs are currently approved by the FDA, spanning therapeutic areas including:
| Therapeutic Area | Examples | Indication |
|---|---|---|
| Metabolic disease | Semaglutide, tirzepatide, liraglutide | Type 2 diabetes, obesity |
| Endocrine disorders | Tesamorelin, octreotide | HIV lipodystrophy, acromegaly |
| Oncology | Leuprolide, degarelix, triptorelin | Prostate cancer, breast cancer |
| Reproductive health | Gonadorelin, cetrorelix | Fertility, contraception |
| Cardiovascular | Bivalirudin, eptifibatide | Anticoagulation, acute coronary syndrome |
| Sexual health | Bremelanotide (PT-141) | Hypoactive sexual desire disorder |
| Rare diseases | Elamipretide (SS-31) | Barth syndrome |
| Diabetes | Insulin and analogs | Type 1 and type 2 diabetes |
Insulin, first used therapeutically in 1922, remains the most widely used peptide drug globally. However, the recent success of GLP-1 receptor agonists has made semaglutide and tirzepatide among the most prescribed medications worldwide, with annual sales exceeding tens of billions of dollars.
The Clinical Evidence Landscape#
Understanding the evidence behind peptide therapy requires distinguishing between compounds at very different stages of scientific validation.
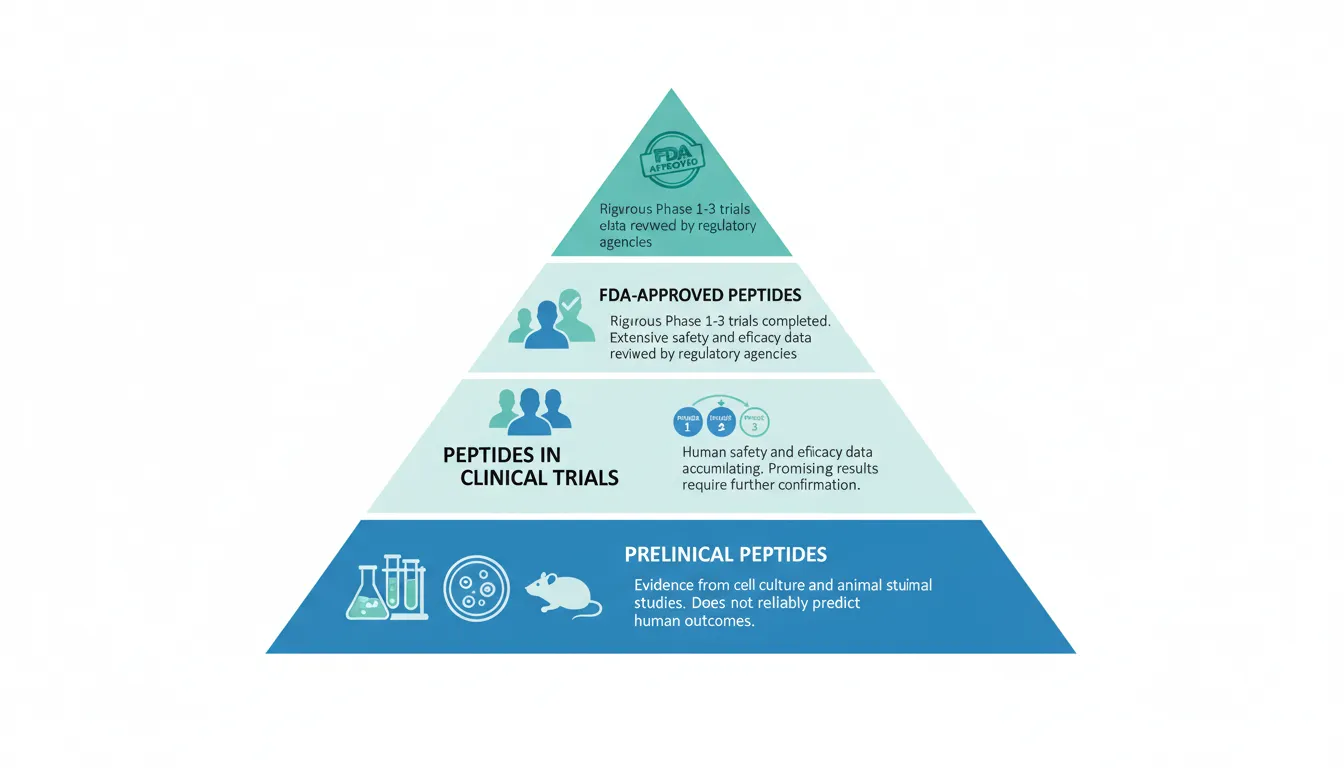
Levels of Evidence#
FDA-approved peptides (e.g., semaglutide, tirzepatide, tesamorelin) have undergone rigorous Phase 1-3 clinical trials involving thousands of human participants, with safety and efficacy data reviewed by regulatory agencies. The evidence base for these compounds is extensive and high-quality.
For example, semaglutide's clinical program includes the STEP trials (demonstrating 14.9-16.0% body weight reduction), the SUSTAIN trials (demonstrating HbA1c reduction in type 2 diabetes), and the SELECT cardiovascular outcomes trial (demonstrating a 20% reduction in major adverse cardiovascular events). This represents some of the strongest evidence in pharmacology.
Peptides in clinical trials (e.g., retatrutide, survodutide, ipamorelin) have human safety and efficacy data, but the evidence is still being accumulated. Phase 2 results for retatrutide showing 24.2% body weight loss are promising but require Phase 3 confirmation. These peptides are further along the evidence continuum than preclinical compounds but have not yet met the full regulatory standard for approval.
Preclinical peptides (e.g., BPC-157, epitalon, FOXO4-DRI) have evidence primarily or exclusively from cell culture and animal studies. While these studies can be mechanistically informative and help guide future clinical research, animal data does not reliably predict human outcomes. The leap from rodent models to human clinical efficacy is substantial, and many compounds that show promise in animal studies fail in human trials.
How to Evaluate Peptide Research#
When encountering claims about peptide therapy, consider these questions:
- Is the peptide FDA-approved for this indication? If yes, the evidence base is strong.
- Are there published human clinical trials? Look for peer-reviewed publications in recognized journals.
- What phase are the trials? Phase 3 data is more reliable than Phase 1 or 2.
- Is the evidence preclinical only? Be cautious about extrapolating animal data to human outcomes.
- Are specific studies cited? Claims without referenced studies should be treated with skepticism.
For more guidance on interpreting peptide research, see our guide on reading research.
How Peptide Therapy Differs from Other Treatments#
Peptide therapeutics occupy a distinct pharmacological niche with characteristics that set them apart from both small-molecule drugs and large biologic proteins:
Compared to Small-Molecule Drugs#
- Higher selectivity: Peptides typically bind to specific receptors with greater selectivity than many small molecules, potentially reducing off-target effects
- Natural analogs: Many therapeutic peptides are based on endogenous molecules, meaning the body already has mechanisms for their metabolism and clearance
- Larger molecular size: Peptides generally cannot cross cell membranes freely, which limits their targets to extracellular receptors and surfaces but also reduces intracellular off-target effects
- Shorter half-life: Unmodified peptides are rapidly degraded by enzymes (DPP-4, NEP, and others), though modern engineering approaches like fatty acid conjugation and PEGylation have dramatically extended peptide half-lives
Compared to Biologic Proteins (Antibodies)#
- Smaller size: Peptides (typically 0.5-5 kDa) are much smaller than antibodies (~150 kDa), allowing better tissue penetration
- Chemical synthesis: Peptides can be manufactured through chemical synthesis rather than cell-culture expression systems, potentially simplifying production
- Lower immunogenicity: Smaller peptides generally provoke less immune response than large proteins
- Oral potential: While challenging, oral delivery of peptides is achievable (as demonstrated by oral semaglutide), whereas oral delivery of antibodies is not currently feasible
Safety and Side Effects#
The safety profile of peptide therapy varies dramatically depending on the specific compound, dose, route of administration, and treatment duration. FDA-approved peptides have well-characterized safety profiles established through large clinical trials, while investigational peptides may have limited safety data.
Common Considerations#
Injection site reactions: Subcutaneous peptide injections commonly cause mild, transient injection site reactions including redness, swelling, and discomfort.
GI side effects: Metabolic peptides (GLP-1 agonists and multi-receptor agonists) are associated with nausea, vomiting, diarrhea, and constipation, particularly during dose escalation. These effects typically diminish over time but can be dose-limiting in some patients.
Hormonal effects: Growth hormone secretagogues can affect cortisol, prolactin, and other hormones depending on their receptor selectivity. More selective peptides like ipamorelin produce fewer off-target hormonal effects than less selective compounds like GHRP-6.
Immunogenic potential: While generally low, some peptides can trigger immune responses, particularly with repeated dosing. This is more common with larger peptides and those that differ significantly from endogenous sequences.
Important Safety Caveats#
- Quality and purity: Research peptides obtained outside of FDA-approved pharmaceutical channels may vary significantly in purity, potency, and contamination. This is a major safety concern for non-pharmaceutical peptides.
- Drug interactions: Some peptides can interact with other medications. GLP-1 agonists, for example, slow gastric emptying and can affect the absorption of oral medications.
- Contraindications: Specific peptide therapies have defined contraindications. GLP-1 agonists, for instance, carry warnings regarding medullary thyroid carcinoma based on animal studies and are contraindicated in patients with a personal or family history of this cancer.
- Long-term data: For newer peptides still in clinical development, long-term safety data (beyond 1-2 years) may not yet be available.
For detailed safety information on specific peptides, browse our peptide directory and consult the side effects and risks profiles for individual compounds.
Current Trends in Peptide Therapy Research#
The peptide therapy field is evolving rapidly, with several key trends shaping the landscape in 2025-2026:
Multi-Receptor Agonists#
The progression from single-target to multi-target peptides represents the most significant trend in metabolic peptide therapy. The evolution from semaglutide (GLP-1 monoagonist) through tirzepatide (dual GIP/GLP-1) to retatrutide (triple GIP/GLP-1/glucagon) demonstrates that engaging complementary receptor pathways can produce additive or synergistic therapeutic effects. For a deep dive into this evolution, see our article on the evolution of GLP-1 receptor agonists.
Oral Peptide Delivery#
The development of oral formulations has been a longstanding challenge in peptide pharmacology. Oral semaglutide (Rybelsus) proved that oral delivery of a GLP-1 agonist is achievable, and in late 2025 an oral formulation of semaglutide for weight management received FDA approval. Oral tirzepatide and non-peptide oral GLP-1 agonists (like orforglipron) are also in clinical development, suggesting that the era of injection-only peptide therapy may be nearing its end for some compounds.
AI-Designed Peptides#
Artificial intelligence and machine learning are increasingly being applied to peptide drug design. AI tools can predict peptide-receptor interactions, optimize amino acid sequences for stability and selectivity, and identify novel therapeutic candidates from vast sequence spaces. In 2026, AI-designed peptides are expected to begin entering early clinical phases, particularly for antimicrobial resistance and metabolic disorders.
Mitochondrial Peptides#
The discovery of mitochondrial-derived peptides (MDPs) -- signaling molecules encoded by the mitochondrial genome -- has opened a new frontier in peptide research. Compounds like MOTS-c and humanin represent a previously unknown class of endogenous peptides with metabolic and cytoprotective effects. SS-31 (elamipretide), a synthetic mitochondrial-targeted peptide, received FDA approval in 2025 for Barth syndrome, marking the first FDA-approved mitochondrial peptide therapy.
Combination Protocols#
Research is increasingly exploring combinations of peptides that target complementary pathways. CagriSema (cagrilintide plus semaglutide) combines amylin receptor agonism with GLP-1 agonism for enhanced weight management. In the research peptide space, growth hormone secretagogue protocols often combine GHRH-pathway and ghrelin-pathway peptides (e.g., sermorelin plus ipamorelin) for synergistic GH release.
Who Uses Peptide Therapy?#
Peptide therapy spans several contexts, from mainstream medicine to investigational research:
Mainstream clinical medicine: FDA-approved peptides like semaglutide, tirzepatide, and insulin are prescribed by physicians across endocrinology, internal medicine, and primary care for established indications including type 2 diabetes, obesity, and cardiovascular risk reduction.
Specialty medicine: Peptides like tesamorelin (HIV-associated lipodystrophy), triptorelin (prostate cancer), and bremelanotide (sexual health) are used in specialized clinical settings.
Anti-aging and longevity clinics: Some clinics prescribe peptides like growth hormone secretagogues, BPC-157, and other investigational compounds for age-related concerns. The evidence base for many of these applications varies significantly, and patients should carefully evaluate the supporting research.
Dermatology and cosmetics: Peptides like GHK-Cu are widely used in topical skincare formulations for wound healing, anti-aging, and skin rejuvenation applications.
Research: Academic and pharmaceutical researchers use peptides extensively in preclinical and clinical studies across nearly every therapeutic area.
Questions to Ask About Peptide Therapy#
If you are considering peptide therapy or evaluating claims about peptide treatments, these questions can help guide your assessment:
- Is this a specific, named peptide with published research? Vague references to "peptide therapy" without specifying the compound should raise questions.
- What is the regulatory status? FDA-approved, in clinical trials, or preclinical only?
- What does the clinical trial data show? Look for published results in peer-reviewed journals, not just promotional materials.
- What are the known side effects and risks? Every effective medication has potential side effects.
- Is the source pharmaceutical-grade? For FDA-approved peptides, use products from licensed pharmacies. Quality and purity of non-pharmaceutical peptides can vary significantly.
- Is the prescribing clinician qualified? Peptide therapy should involve appropriately credentialed healthcare providers who understand the specific compounds being used.
Conclusion#
Peptide therapy encompasses a broad and rapidly evolving spectrum of treatments, from FDA-approved blockbuster drugs like semaglutide and tirzepatide to investigational compounds in early clinical trials to preclinical research molecules. The field's strength lies in the ability of peptides to target specific biological pathways with high selectivity, leveraging the body's own signaling systems for therapeutic benefit.
The evidence base varies enormously across the peptide landscape. Metabolic peptides like the GLP-1 agonists represent some of the most rigorously validated treatments in modern medicine, supported by large randomized controlled trials and decades of clinical experience. At the other end of the spectrum, many healing, anti-aging, and neuroprotective peptides have compelling preclinical data but limited or no human clinical trial evidence.
For anyone interested in peptide therapy, the most important step is understanding where a specific peptide falls on this evidence continuum. An FDA-approved peptide prescribed for its labeled indication by a qualified clinician represents a fundamentally different proposition than an investigational peptide obtained from an unregulated source. Both may have genuine biological rationale, but the level of evidence, quality assurance, and clinical oversight differ substantially.
The future of peptide therapy is promising. Multi-receptor agonists are pushing the boundaries of metabolic medicine, oral delivery platforms are expanding patient access, AI-driven design is accelerating drug discovery, and new classes of peptides -- from mitochondrial-derived peptides to senolytics -- are opening therapeutic frontiers that were unimaginable a decade ago. As the field continues to mature, the gap between research promise and clinical reality will likely narrow, bringing the benefits of peptide-based treatments to an ever-wider patient population.
Explore our complete peptide directory to learn more about specific compounds, or visit our learning center for educational resources on peptide science, research methods, and safety considerations.
References#
- Lau DCW, et al. Once-weekly cagrilintide for weight management in people with overweight and obesity. Lancet. 2021;398(10317):2160-2172.
- Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387(4):327-340. (SURMOUNT-1)
- Jastreboff AM, et al. Triple-hormone-receptor agonist retatrutide for obesity. N Engl J Med. 2023;389(6):514-526.
- Wilding JPH, et al. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384(11):989-1002. (STEP 1)
- Lincoff AM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389(24):2221-2232. (SELECT)
- Muttenthaler M, et al. Trends in peptide drug discovery. Nat Rev Drug Discov. 2021;20(4):309-325.
- Wang L, et al. Therapeutic peptides: historical perspectives, current development trends, and future directions. Bioorg Med Chem. 2018;26(10):2801-2815.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- BPC-157 Overview and Research Guide
- BPC-157 Dosing Protocols
- BPC-157 Side Effects and Safety
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- Epitalon Overview and Research Guide
- Epitalon Dosing Protocols
- Epitalon Side Effects and Safety
- GHK-Cu Overview and Research Guide
- GHK-Cu Dosing Protocols
- GHK-Cu Side Effects and Safety
- Tesamorelin Overview and Research Guide
- Tesamorelin Dosing Protocols
- Tesamorelin Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About What Is Peptide Therapy? A Complete Guide to Peptide-Based Treatments
What does this article cover?
Peptide therapy uses short-chain amino acids to target specific biological pathways. Learn how peptide treatments work, FDA-approved options, clinical applications, and what the research shows. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, BPC-157, Ipamorelin, Epitalon, GHK-Cu, Tesamorelin, Retatrutide. Key context: Semaglutide (FDA-approved GLP-1 receptor agonist representing the most commercially successful class of peptid...); Tirzepatide (First dual GIP/GLP-1 receptor agonist approved by the FDA, demonstrating the multi-receptor agoni...); BPC-157 (Widely studied preclinical healing peptide illustrating the gap between research interest and cli...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "What Is Peptide Therapy? A Complete Guide to Peptide-Based Treatments." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: FDA-approved GLP-1 receptor agonist representing the most commercially successful class of peptid.... First dual GIP/GLP-1 receptor agonist approved by the FDA, demonstrating the multi-receptor agoni.... Widely studied preclinical healing peptide illustrating the gap between research interest and cli.... These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: FDA-approved GLP-1 receptor agonist representing the most commercially successful class of peptide therapeutics for metabolic disease. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.
Best Peptides to Stack with Retatrutide (2026 Research Guide)
A 2026 research-focused review of the peptides most often discussed alongside retatrutide for GI side effects, lean-mass preservation, hair and skin changes, sleep, and adjunct fat loss — what the literature does and does not support.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.
You Might Also Like
Related content you may find interesting