The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics

Introduction#
The development of GLP-1 (glucagon-like peptide-1) receptor agonists represents one of the most significant therapeutic advances in metabolic medicine over the past two decades. What began as a strategy to enhance the naturally short-lived incretin effect has evolved into a new paradigm of multi-receptor agonism that addresses obesity, type 2 diabetes, cardiovascular disease, and potentially liver disease through increasingly sophisticated pharmacological approaches.
This evolution can be traced through four key inflection points: the establishment of GLP-1 monoagonism with compounds like semaglutide; the introduction of dual GIP/GLP-1 agonism with tirzepatide; the expansion to triple GIP/GLP-1/glucagon agonism with retatrutide; and the alternative dual agonist strategy of glucagon/GLP-1 with survodutide. Each step has not only increased efficacy but has also revealed new biology about how metabolic receptor systems interact and how different receptor combinations create distinct therapeutic profiles.
This review examines the evidence, mechanisms, and clinical implications at each stage of this evolution, analyzing what multi-receptor strategies have taught us about metabolic pharmacology and where the field is heading.
The Foundation: GLP-1 Monoagonism#
The Incretin Effect and GLP-1 Biology#
GLP-1 is a 30-amino acid peptide hormone secreted by intestinal L-cells in response to nutrient ingestion. Its physiological effects include glucose-dependent insulin secretion enhancement, glucagon suppression, gastric emptying delay, and central satiety signaling through hypothalamic and brainstem receptors. The therapeutic potential of GLP-1 was recognized early, but native GLP-1 has a plasma half-life of only 2-3 minutes due to rapid degradation by dipeptidyl peptidase-4 (DPP-4).
The development of DPP-4-resistant GLP-1 analogs -- first exenatide (from Gila monster saliva), then liraglutide, and ultimately semaglutide -- progressively extended the half-life and potency of GLP-1 agonism. Semaglutide, with its C18 fatty diacid modification enabling albumin binding and a half-life of approximately 7 days, became the benchmark GLP-1 monoagonist.
Semaglutide: Defining the Ceiling of GLP-1 Monoagonism#
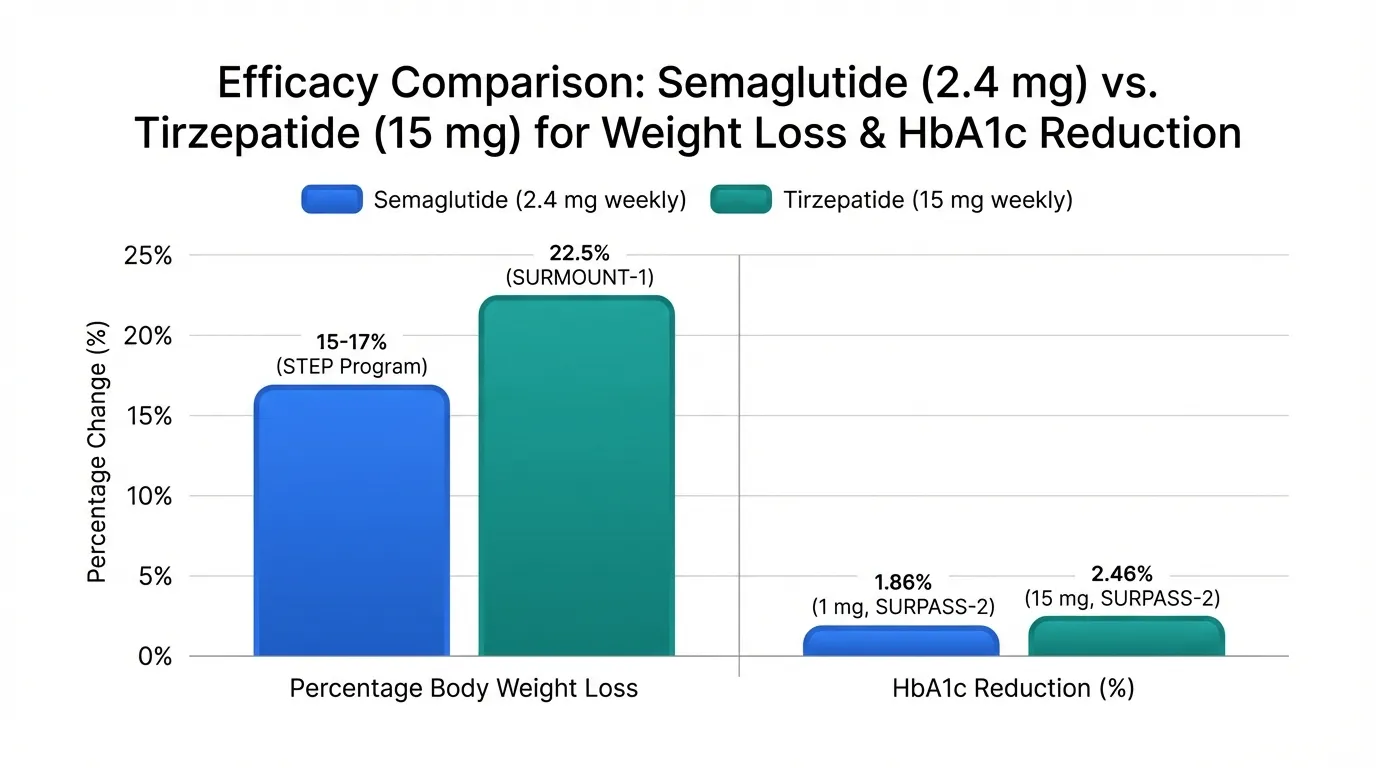
The STEP clinical trial program established semaglutide 2.4 mg weekly (Wegovy) as a transformative obesity treatment, demonstrating approximately 15-17% body weight loss at 68 weeks. The SELECT cardiovascular outcomes trial further demonstrated a 20% reduction in major adverse cardiovascular events independent of diabetes status. However, semaglutide also defined the apparent efficacy ceiling of pure GLP-1 agonism: weight loss plateaued in the 15-17% range, and dose escalation beyond 2.4 mg was limited by gastrointestinal tolerability.
This ceiling raised a fundamental question: could engaging additional metabolic receptors alongside GLP-1 provide additive or synergistic efficacy beyond what GLP-1 agonism alone could achieve? The subsequent development of multi-receptor agonists answered this question decisively.
First Leap: Tirzepatide and Dual GIP/GLP-1 Agonism#
The GIP Hypothesis#
The decision to combine GLP-1 agonism with GIP (glucose-dependent insulinotropic polypeptide) agonism was not obvious. GIP was historically considered primarily a glucose-dependent insulin secretagogue, and paradoxically, some early research suggested that GIP receptor antagonism might be beneficial for obesity. Eli Lilly's development of tirzepatide was therefore a pharmacological bet on the hypothesis that GIP agonism, when combined with GLP-1 agonism, would provide complementary metabolic benefits.
Tirzepatide is a 39-amino acid peptide with a C20 fatty diacid moiety, engineered with approximately 5-fold selectivity for GIP over GLP-1 receptors. This GIP-dominant profile was a deliberate design choice, reflecting preclinical evidence that GIP receptor engagement in the brain activates satiety pathways partially distinct from GLP-1 signaling, and that GIP effects on adipose tissue, bone metabolism, and beta-cell function provide complementary metabolic actions.
Clinical Evidence: SURPASS and SURMOUNT Programs#
Tirzepatide's clinical validation came through two comprehensive Phase 3 programs:
SURPASS (Type 2 Diabetes):
- SURPASS-2 directly compared tirzepatide 15 mg to semaglutide 1 mg and demonstrated superior HbA1c reduction (2.46% vs 1.86%) and weight loss (12.4 kg vs 6.2 kg)
- SURPASS-1, -3, -4, and -5 confirmed superiority over insulin analogs and placebo across diverse patient populations
- HbA1c reductions of 1.87-2.59% placed tirzepatide at the top of available glycemic therapies
SURMOUNT (Obesity):
- SURMOUNT-1 demonstrated 20.9% body weight reduction at 72 weeks with the 15 mg dose in non-diabetic obese patients -- a 4-6 percentage point improvement over semaglutide's STEP results
- SURMOUNT-2 confirmed efficacy in obese patients with T2D (14.7% weight loss)
- SURMOUNT-3 and SURMOUNT-4 evaluated intensive lifestyle intervention followed by tirzepatide and sustained treatment effects
These results established that dual GIP/GLP-1 agonism could surpass the GLP-1 monoagonist ceiling, validating the multi-receptor approach. Tirzepatide received FDA approval as Mounjaro (May 2022) for type 2 diabetes and Zepbound (November 2023) for chronic weight management, becoming the first dual-agonist incretin to reach the market.
What Tirzepatide Revealed#
Beyond its clinical efficacy, tirzepatide provided important biological insights:
- GIP is not merely an insulin secretagogue: Its central and peripheral metabolic effects are clinically meaningful
- Multi-receptor engagement is additive: The additional 5-7% weight loss over GLP-1 monoagonism was not explained by increased GLP-1 activity alone
- GI tolerability can be maintained: Despite greater overall efficacy, tirzepatide's GI side effect profile was comparable to or better than semaglutide at equivalent weight loss, possibly because GIP activates partially non-overlapping satiety pathways with different tolerability profiles
Second Leap: Retatrutide and Triple GIP/GLP-1/Glucagon Agonism#
Adding Glucagon: Counterintuitive Pharmacology#
The inclusion of glucagon receptor agonism in a metabolic therapeutic initially appeared paradoxical. Glucagon is the primary counter-regulatory hormone to insulin, promoting hepatic glucose output and potentially worsening hyperglycemia. However, glucagon's metabolic effects extend well beyond glycogenolysis:
- Hepatic fat oxidation: Glucagon potently stimulates beta-oxidation of fatty acids in the liver, directly reducing hepatic steatosis
- Thermogenesis: Glucagon activates brown adipose tissue and increases resting energy expenditure through futile metabolic cycling
- Satiety: Glucagon signaling in the brain contributes to appetite suppression
- Amino acid catabolism: Glucagon promotes hepatic amino acid processing, with implications for body composition
The pharmacological hypothesis behind retatrutide was that glucagon's hyperglycemic potential could be adequately counterbalanced by concurrent GLP-1 and GIP agonism, while glucagon's catabolic and thermogenic effects would provide additional weight loss beyond what dual GIP/GLP-1 agonism achieves.
Phase 2 Results: A New Benchmark#
Retatrutide (LY3437943) is a 39-amino acid peptide simultaneously targeting all three receptors. The Phase 2 dose-finding trial, published in the New England Journal of Medicine in 2023, produced results that shifted expectations for the field:
- Weight loss: The 12 mg dose achieved 24.2% body weight reduction at 48 weeks in Phase 2, subsequently confirmed and exceeded by Phase 3 TRIUMPH-4 data showing 28.7% at 68 weeks -- the highest reported for any metabolic peptide in a Phase 3 trial
- Liver fat: MRI-PDFF measurements showed up to 82.4% reduction in liver fat content at the highest dose, a magnitude not achieved by any other pharmacological intervention
- Metabolic parameters: Improvements in HbA1c, triglycerides, and blood pressure consistent with substantial metabolic benefit
- Dose-response: Clear dose-dependent efficacy across 1 mg, 4 mg, 8 mg, and 12 mg weekly doses
The liver fat data was particularly striking. While GLP-1 monoagonists and GIP/GLP-1 dual agonists reduce liver fat primarily through weight loss and improved insulin sensitivity, retatrutide's glucagon component directly drives hepatic fat oxidation -- a weight-independent mechanism that produced liver fat reductions far exceeding what weight loss alone would predict.
Safety Considerations#
Retatrutide's Phase 2 data also revealed the safety trade-offs of adding glucagon agonism:
- GI side effects were comparable in incidence to tirzepatide but included higher rates of diarrhea at the 12 mg dose
- Small mean heart rate increases of 2-4 bpm were observed, likely related to glucagon-mediated sympathetic activation
- Glucose homeostasis was maintained despite the glucagon component, with the GLP-1 and GIP agonism providing adequate counter-regulation
- Transient liver enzyme elevations occurred in some patients, though paradoxically in the context of dramatic liver fat reduction
Phase 3 results from TRIUMPH-4 have confirmed the Phase 2 efficacy, with 28.7% weight loss at 68 weeks. Additional Phase 3 trials across the TRIUMPH program will further characterize safety at scale.
Alternative Strategy: Survodutide and Dual Glucagon/GLP-1 Agonism#
A Different Receptor Pairing#
While retatrutide expanded the multi-receptor concept by adding glucagon to the GIP/GLP-1 foundation, survodutide (BI 456906, developed by Boehringer Ingelheim) took a different approach: pairing glucagon with GLP-1 while omitting GIP. This creates a fundamentally different metabolic profile -- one focused more on catabolic energy expenditure and hepatic fat oxidation than on incretin-mediated appetite suppression.
Survodutide's molecular weight of 4170.6 Da and its glucagon/GLP-1 dual agonism position it as a metabolic therapeutic with particularly strong potential for liver-related indications. The glucagon component provides direct hepatic fat catabolism, while the GLP-1 component counterbalances glucagon's hyperglycemic effects and provides appetite suppression.
Clinical Evidence and MASH Focus#
Survodutide's clinical development reflects its differentiated mechanism:
Obesity Phase 2: Demonstrated up to 18.7% weight loss at 46 weeks, which, while impressive, is lower than tirzepatide's Phase 3 and retatrutide's Phase 2 results. This suggests that the GIP component present in tirzepatide and retatrutide provides additional appetite-suppressive efficacy that glucagon/GLP-1 dual agonism alone does not fully replicate.
MASH Phase 2: This is where survodutide's differentiation is most apparent. Phase 2 data showed significant liver fat reduction measured by MRI-PDFF, with a notable proportion of patients achieving MASH resolution without fibrosis worsening on histological assessment. These results positioned survodutide as a leading candidate for MASH treatment, a disease with very limited approved pharmacological options.
Phase 3 Program (SYNCHRONIZE): Ongoing trials are evaluating survodutide in both obesity and MASH, with the latter representing its potentially strongest clinical niche.
The Receptor Pairing Debate#
The existence of both survodutide (glucagon/GLP-1) and tirzepatide (GIP/GLP-1) as dual agonists, alongside retatrutide (GIP/GLP-1/glucagon) as a triple agonist, creates a natural experiment in receptor pharmacology:
- GIP/GLP-1 (tirzepatide): Maximum incretin synergy; strongest glucose lowering; 20.9% weight loss
- Glucagon/GLP-1 (survodutide): Maximum hepatic catabolism; strongest liver fat effects; 18.7% weight loss
- GIP/GLP-1/glucagon (retatrutide): All three pathways; highest weight loss (28.7% Phase 3 TRIUMPH-4); strongest liver fat reduction (82.4%)
This comparison suggests that GIP agonism contributes primarily to appetite suppression and incretin-mediated effects, while glucagon agonism contributes primarily to energy expenditure and hepatic fat catabolism. The triple agonist captures both contributions.
Mechanistic Lessons from the Multi-Receptor Era#
Non-Redundant Receptor Biology#
The progression from mono- to dual to triple agonists has revealed that GLP-1, GIP, and glucagon receptors drive partially non-overlapping biological effects:
| Receptor | Appetite | Glucose | Liver Fat | Energy Expenditure |
|---|---|---|---|---|
| GLP-1 | Strong suppression | Strong lowering | Moderate reduction (indirect) | Minimal effect |
| GIP | Moderate suppression | Moderate lowering | Minimal effect | Minimal effect |
| Glucagon | Moderate suppression | Raises acutely | Strong reduction (direct) | Strong increase |
This non-redundancy explains why multi-receptor approaches provide more than just "more of the same" -- each receptor adds qualitatively different metabolic effects.
The Tolerability Paradox#
A notable observation across the clinical programs is that multi-receptor agonists have not shown proportionally worse GI tolerability despite greater overall metabolic efficacy. This may be because:
- Different receptors activate partially distinct satiety circuits, distributing the anorexigenic signal across multiple pathways rather than saturating a single one
- GIP receptor engagement may actually attenuate GLP-1-mediated GI side effects through complementary signaling
- Glucagon's catabolic effects contribute to weight loss through energy expenditure rather than appetite suppression alone
Implications for Specific Disease Populations#
The multi-receptor data suggest differentiated clinical positioning:
- Pure obesity: Triple agonists (retatrutide) may offer maximum weight loss once Phase 3 data are confirmed
- T2D with obesity: Tirzepatide is the established standard with proven glucose-lowering and weight loss
- MASH/MASLD: Glucagon-containing agonists (survodutide, retatrutide) show the most promise for hepatic endpoints
- Cardiovascular risk reduction: GLP-1 agonists have the most cardiovascular outcomes data; multi-receptor compounds await CVOT results
Future Directions#
Beyond Triple Agonism#
The logical extension of multi-receptor agonism raises the question: are there additional receptors worth engaging? Candidates under investigation include:
- Amylin receptor: Cagrilintide combined with semaglutide (CagriSema) targets the amylin pathway for additional satiety signaling
- Fibroblast growth factor receptors: FGF21 analogs (efruxifermin, pegozafermin) target metabolic and liver endpoints through non-incretin mechanisms
- Peptide YY: PYY analogs provide post-prandial satiety signaling complementary to GLP-1
Oral Formulations#
The current multi-receptor agonists all require subcutaneous injection. The development of oral semaglutide (Rybelsus) demonstrated that GLP-1 agonists can be delivered orally, and efforts are underway to develop oral formulations of dual and triple agonists. Oral tirzepatide and oral orforglipron (a non-peptide GLP-1 agonist) are in clinical development.
Personalized Selection#
As the therapeutic menu expands, clinicians will need frameworks for selecting among GLP-1 monoagonists, GIP/GLP-1 dual agonists, glucagon/GLP-1 dual agonists, and triple agonists based on individual patient characteristics. Factors including hepatic steatosis, glycemic control needs, cardiovascular risk profile, and tolerability history will likely guide receptor combination selection.
Conclusion#
The evolution from GLP-1 monoagonism through dual and triple agonism represents a paradigm shift in metabolic therapeutics. Semaglutide established that GLP-1 agonism could produce clinically meaningful weight loss and cardiovascular benefit. Tirzepatide demonstrated that adding GIP receptor engagement breaks through the GLP-1 monoagonist ceiling, achieving FDA approval with 20.9% weight loss. Retatrutide's data confirm that adding glucagon agonism pushes efficacy further, with 28.7% weight loss in Phase 3 TRIUMPH-4 (24.2% in Phase 2) and extraordinary liver fat reduction. Survodutide offers an alternative glucagon-inclusive strategy specifically targeting the large unmet need in MASH treatment.
The multi-receptor era has not only improved clinical outcomes but has fundamentally expanded our understanding of metabolic receptor biology. Each new receptor addition has revealed previously underappreciated physiological roles for GIP and glucagon, demonstrated that metabolic pathways are more complementary than redundant, and shown that rationally designed multi-receptor peptides can provide qualitatively different therapeutic profiles rather than simply greater potency.
As Phase 3 data for retatrutide and survodutide become available, the field will have an unprecedented toolkit of metabolic peptide therapeutics tailored to different patient populations and clinical needs. The trajectory from semaglutide to retatrutide -- from single-receptor simplicity to multi-receptor sophistication -- illustrates how iterative pharmacological innovation can transform an entire therapeutic area within a single decade.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Survodutide Overview and Research Guide
- Survodutide Dosing Protocols
- Survodutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
What does this article cover?
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Tirzepatide, Retatrutide, Survodutide. Key context: Tirzepatide (First FDA-approved dual GIP/GLP-1 receptor agonist, demonstrating that multi-receptor approaches ...); Retatrutide (Triple GIP/GLP-1/glucagon receptor agonist representing the next evolutionary step with the highe...); Survodutide (Dual glucagon/GLP-1 agonist offering a different receptor pairing strategy with particular promis...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: First FDA-approved dual GIP/GLP-1 receptor agonist, demonstrating that multi-receptor approaches .... Triple GIP/GLP-1/glucagon receptor agonist representing the next evolutionary step with the highe.... Dual glucagon/GLP-1 agonist offering a different receptor pairing strategy with particular promis.... These takeaways are based on the research data available at the time of publication.
What is Tirzepatide and why is it significant?
Tirzepatide is a peptide discussed in this article because: First FDA-approved dual GIP/GLP-1 receptor agonist, demonstrating that multi-receptor approaches surpass GLP-1 monoagonism. For a complete profile of Tirzepatide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Retatrutide Canada Guide
Retatrutide in Canada: Everything You Need to Know — part of the Next-Gen Weight Loss content cluster.

The History of Peptide Research: From Insulin to Modern Therapeutics
History of peptide research from insulin's 1921 discovery to modern GLP-1 agonists. Key milestones in synthesis and therapeutics.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.
You Might Also Like
Related content you may find interesting