Semaglutide vs Retatrutide vs Tirzepatide: Weight Loss Compared

Introduction#
The weight loss peptide landscape has undergone a transformation since semaglutide's approval, evolving from single-receptor GLP-1 agonists to multi-receptor compounds targeting two or three metabolic pathways simultaneously. This evolution has produced a spectrum of approved and investigational therapies with progressively greater efficacy — and increasingly complex pharmacology.
This guide compares the five most significant weight loss peptides in the current landscape: the FDA-approved semaglutide and tirzepatide, and the investigational next-generation compounds retatrutide, survodutide, and mazdutide. For clinical trial updates on these compounds, see Peptides in Clinical Trials 2026.
The Receptor Landscape#
Understanding the differences between these peptides requires understanding their receptor targets:
GLP-1 Receptor (Glucagon-Like Peptide-1)#
All five peptides activate the GLP-1 receptor. GLP-1 agonism produces appetite suppression through hypothalamic signaling, slowed gastric emptying (contributing to satiety), improved insulin secretion, and reduced glucagon release. This is the foundation of modern metabolic peptide therapy.
GIP Receptor (Glucose-Dependent Insulinotropic Polypeptide)#
Tirzepatide and retatrutide add GIP receptor agonism. GIP's role in weight loss was initially counterintuitive — GIP was historically considered an obesity-promoting hormone. However, pharmacological GIP agonism at high doses appears to enhance weight loss through mechanisms that are still being fully characterized, potentially including effects on fat metabolism and central appetite regulation.
Glucagon Receptor#
Retatrutide, survodutide, and mazdutide include glucagon receptor agonism. Glucagon promotes hepatic fat oxidation, increases energy expenditure, and may reduce appetite through CNS effects. The glucagon component is particularly relevant for liver-related metabolic disease (MASH) because glucagon directly promotes hepatic lipid metabolism.
Head-to-Head Comparison#
1. Semaglutide (Ozempic / Wegovy)#
Receptor Profile: GLP-1 only Approval Status: FDA-approved (2017 for diabetes; 2021 for obesity) Maximum Approved Dose: 2.4 mg weekly (Wegovy)
Semaglutide established the modern weight loss peptide category. It remains the most prescribed and best-studied compound in this class.
Key Efficacy Data:
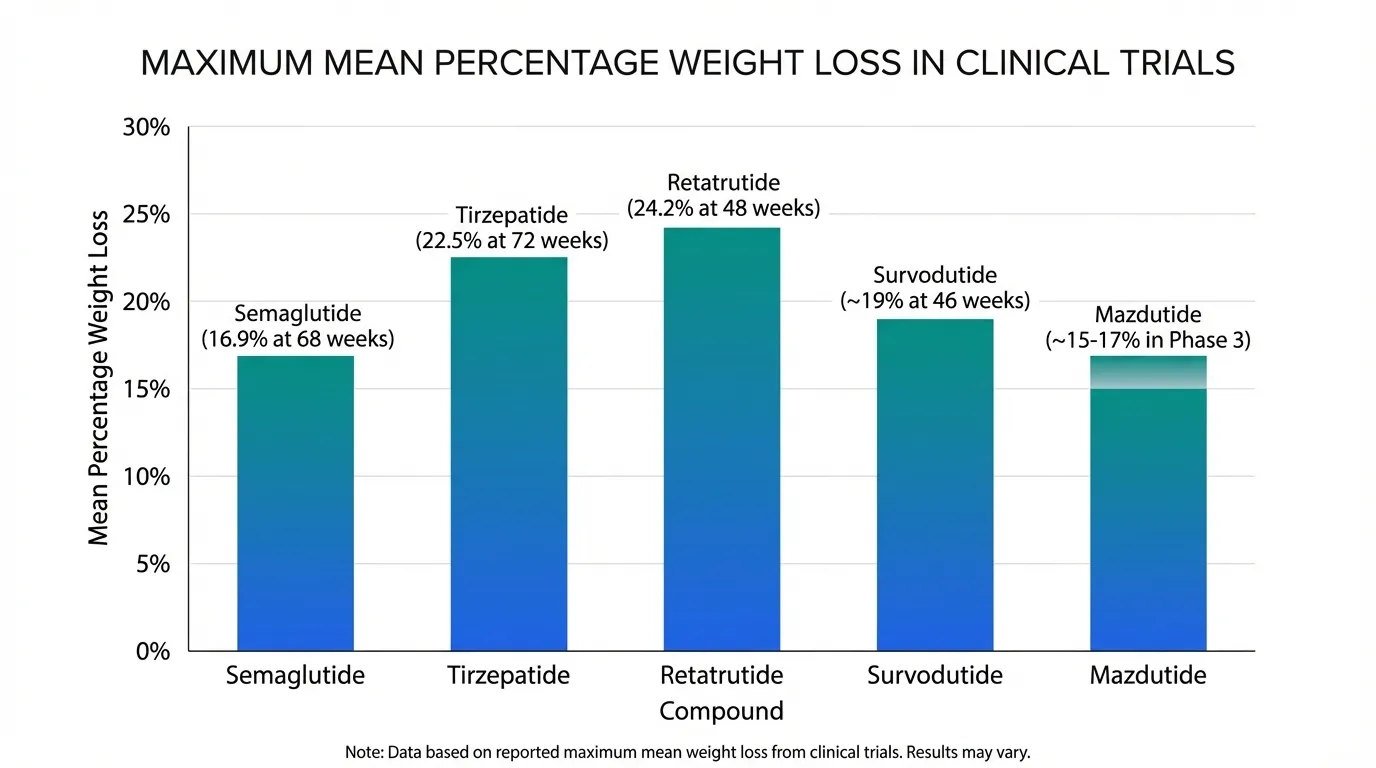
- STEP 1 trial: 16.9% mean weight loss at 2.4 mg over 68 weeks vs. 2.4% placebo
- STEP 3 (with intensive behavioral therapy): 16.0% weight loss
- STEP 5 (2-year data): weight loss maintained through 104 weeks
- SELECT cardiovascular outcomes trial: 20% reduction in major adverse cardiovascular events (MACE)
Strengths: Longest clinical track record among this group; cardiovascular outcomes data (SELECT trial); oral formulation available (Rybelsus); multiple approved indications; extensive real-world safety data.
Limitations: Lower maximum weight loss compared to tirzepatide and retatrutide; significant GI side effects (nausea, vomiting, diarrhea) particularly during dose titration; weight regain upon discontinuation demonstrated in STEP 1 extension data.
For cost comparisons, see Semaglutide vs Tirzepatide Cost.
2. Tirzepatide (Mounjaro / Zepbound)#
Receptor Profile: GIP + GLP-1 dual agonist Approval Status: FDA-approved (2022 for diabetes; 2023 for obesity) Maximum Approved Dose: 15 mg weekly
Tirzepatide is the first dual agonist to receive FDA approval and currently offers the highest weight loss among approved therapies.
Key Efficacy Data:
- SURMOUNT-1 trial: 20.9% mean weight loss at 15 mg over 72 weeks vs. 2.4% placebo
- SURMOUNT-2 (with type 2 diabetes): 14.7% weight loss at highest dose
- SURPASS trials: superior HbA1c reduction compared to semaglutide 1 mg (SURPASS-2)
- SUMMIT (heart failure): positive results for HFpEF with obesity
Strengths: Highest approved weight loss efficacy; dual mechanism provides broader metabolic benefits than GLP-1 alone; expanding indications (heart failure, sleep apnea, MASH); superior glycemic control vs. semaglutide in head-to-head.
Limitations: Shorter clinical track record than semaglutide; no completed cardiovascular outcomes trial (SURPASS-CVOT ongoing); GI side effect profile similar to semaglutide; higher cost in some markets. For detailed comparisons, see Semaglutide vs Tirzepatide and Retatrutide vs Tirzepatide.
3. Retatrutide (Investigational)#
Receptor Profile: GIP + GLP-1 + glucagon triple agonist Approval Status: Phase 3 (TRIUMPH program) Investigational Dose Range: 1-12 mg weekly
Retatrutide represents the next frontier in multi-agonist therapy, adding glucagon receptor activation to the GIP/GLP-1 foundation.
Key Efficacy Data:
- Phase 2 study: 24.2% mean weight loss at 12 mg over 48 weeks — the highest reported for any metabolic peptide in a clinical trial
- Dose-dependent response across all dose groups (1-12 mg)
- Significant improvements in glycemic parameters, lipids, and blood pressure
- Phase 2 MASH sub-study showed substantial hepatic fat reduction
Strengths: Highest weight loss of any compound in this class; glucagon component adds energy expenditure and liver-specific benefits; potential for MASH indication; Phase 3 program underway.
Limitations: Not yet approved — Phase 3 data pending; the Phase 2 study was relatively small and results may not fully replicate in larger trials; the contribution of each receptor component to efficacy and side effects is not fully characterized; theoretical concerns about glucagon's glycemic effects in diabetic populations. For detailed comparisons, see Retatrutide vs Semaglutide.
4. Survodutide (Investigational)#
Receptor Profile: GLP-1 + glucagon dual agonist Approval Status: Phase 3 (SYNCHRONIZE and obesity programs) Investigational Dose Range: Up to 6 mg weekly
Survodutide combines GLP-1 with glucagon agonism but omits GIP, creating a differentiated profile particularly suited to liver disease.
Key Efficacy Data:
- Phase 2 obesity: approximately 19% weight loss at highest dose over 46 weeks
- Phase 2 MASH: up to 83% MASH resolution with histological improvement at 48 weeks
- Significant liver fat reduction consistent with glucagon's hepatic effects
Strengths: Strongest MASH data of any compound in this class; GLP-1/glucagon combination targets hepatic fat metabolism directly; clear differentiation from tirzepatide's GIP-based mechanism; Phase 3 MASH program is among the most advanced.
Limitations: Lower weight loss than retatrutide (no GIP component); Phase 3 data pending; glucagon's potential glycemic effects require careful characterization in diabetic populations; developed by Boehringer Ingelheim, which has less experience in the obesity therapeutic market than Lilly or Novo Nordisk.
5. Mazdutide (Investigational)#
Receptor Profile: GLP-1 + glucagon dual agonist Approval Status: Phase 3 (GLORY program, primarily China) Investigational Dose Range: Up to 9 mg
Mazdutide shares survodutide's dual GLP-1/glucagon mechanism but is being developed primarily in Asian populations.
Key Efficacy Data:
- Phase 3 GLORY data: approximately 15-17% weight loss in Chinese populations with obesity
- Significant HbA1c reductions in type 2 diabetes populations
- Dual agonist effects consistent with the GLP-1/glucagon mechanism class
Strengths: Critical Asian population data addressing a major evidence gap; closest to regulatory approval in China; addresses the world's largest absolute obesity population; Phase 3 data available.
Limitations: Comparatively lower weight loss than retatrutide or tirzepatide; development concentrated in China with uncertain global regulatory timeline; limited head-to-head data with other compounds.
Complete Comparison Table#
| Feature | Semaglutide | Tirzepatide | Retatrutide | Survodutide | Mazdutide |
|---|---|---|---|---|---|
| Receptor Targets | GLP-1 | GIP + GLP-1 | GIP + GLP-1 + glucagon | GLP-1 + glucagon | GLP-1 + glucagon |
| Maximum Weight Loss | ~17% (68 wk) | ~20.9% (72 wk) | ~24.2% (48 wk) | ~19% (46 wk) | ~17% (Phase 3) |
| FDA Status | Approved | Approved | Phase 3 | Phase 3 | Phase 3 (China) |
| MASH Data | Limited | In development | Phase 2 (promising) | Phase 2 (strongest) | Limited |
| CV Outcomes | SELECT (positive) | SURPASS-CVOT (ongoing) | Not yet studied | Not yet studied | Not yet studied |
| Dosing | Once weekly SC | Once weekly SC | Once weekly SC | Once weekly SC | Once weekly SC |
| Oral Option | Yes (Rybelsus) | No | No | No | No |
| Developer | Novo Nordisk | Eli Lilly | Eli Lilly | Boehringer Ingelheim | Innovent Biologics |
Beyond Weight Loss: Differentiated Benefits#
Liver Health (MASH)#
Survodutide and retatrutide — both containing glucagon receptor agonism — show the most promise for liver-specific benefits. Glucagon directly promotes hepatic fat oxidation, providing a mechanistic advantage over GLP-1-only or GIP/GLP-1 compounds for MASH treatment.
Cardiovascular Protection#
Semaglutide currently has the only completed cardiovascular outcomes data (SELECT trial). Tirzepatide's SURPASS-CVOT will provide the next major dataset. The cardiovascular effects of retatrutide and survodutide are unknown.
Glycemic Control#
All five compounds improve glycemic parameters. Tirzepatide has shown superior HbA1c reduction versus semaglutide in head-to-head trials (SURPASS-2). The glucagon component in retatrutide, survodutide, and mazdutide theoretically complicates glycemic control (glucagon raises blood glucose), though clinical data has not shown problematic hyperglycemia.
Body Composition#
Emerging data suggests that the specific receptor profile may influence the ratio of fat mass to lean mass loss. GLP-1 agonists alone produce substantial lean mass loss alongside fat loss. Whether multi-agonist approaches preserve lean mass better is an active area of investigation.
Side Effect Comparison#
The GI side effect profile is broadly similar across all five compounds, driven primarily by GLP-1 receptor agonism:
- Nausea — the most common side effect, typically most pronounced during dose titration (30-50% across compounds)
- Vomiting — less common than nausea but clinically significant (10-25%)
- Diarrhea — variable (10-20%)
- Constipation — less common but reported (5-15%)
The GIP component (tirzepatide, retatrutide) may partially mitigate GI side effects through anti-emetic properties of GIP receptor agonism, though this has not been conclusively demonstrated. The glucagon component (retatrutide, survodutide, mazdutide) raises theoretical concerns about increased heart rate and glycemic effects, though clinical data has not shown clinically significant differences.
Choosing Between Approved Options#
For patients and clinicians choosing between currently approved therapies:
- Semaglutide may be preferred when cardiovascular risk reduction is a primary goal (SELECT data), when an oral option is desired, or when the longer safety track record provides additional confidence
- Tirzepatide may be preferred when maximum weight loss efficacy is the primary goal, when glycemic control needs are significant, or when body composition considerations are important
Both compounds share similar contraindications: personal or family history of medullary thyroid carcinoma, MEN2 syndrome, pregnancy, and hypersensitivity. For a detailed cost comparison, see Semaglutide vs Tirzepatide Cost.
The Future Landscape#
The metabolic peptide field is evolving rapidly. Beyond the five compounds covered here, the pipeline includes:
- CagriSema (cagrilintide + semaglutide) — amylin/GLP-1 combination in Phase 3 (see Cagrilintide + Semaglutide Stack)
- Orforglipron — oral non-peptide GLP-1 agonist that could eliminate injection requirements
- AMG 133 (maridebart cafraglutide) — a bispecific antibody combining GIP antagonism with GLP-1 agonism (opposite GIP approach from tirzepatide)
- Longer-acting formulations — monthly and potentially quarterly injection options under development
Conclusion#
The weight loss peptide landscape in 2026 offers a spectrum of options from the established single-agonist semaglutide to the investigational triple-agonist retatrutide. Each generation of compounds has demonstrated incrementally greater weight loss efficacy, with the trade-off of increasing pharmacological complexity.
For approved therapies, the choice between semaglutide and tirzepatide depends on individual patient factors, comorbidities, and treatment goals. The investigational compounds — retatrutide for maximum efficacy, survodutide for liver-specific benefits, and mazdutide for Asian population data — will reshape the landscape further as Phase 3 results emerge.
For pharmacokinetic modeling of these compounds, visit the GLP-1 Saturation Calculator. For dose calculations and safety information, see the Dosing Calculator and Safety page.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Survodutide Overview and Research Guide
- Survodutide Dosing Protocols
- Survodutide Side Effects and Safety
- Mazdutide Overview and Research Guide
- Mazdutide Dosing Protocols
- Mazdutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About Semaglutide vs Retatrutide vs Tirzepatide: Weight Loss Compared
What does this article cover?
Compare semaglutide, tirzepatide, retatrutide, survodutide, and mazdutide — mechanisms, efficacy, and the shift to multi-agonist therapy. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, Retatrutide, Survodutide, Mazdutide. Key context: Semaglutide (FDA-approved GLP-1 receptor agonist that established the modern weight loss peptide category with...); Tirzepatide (FDA-approved dual GIP/GLP-1 agonist with up to 20.9% weight loss, currently the most effective ap...); Retatrutide (Investigational triple GIP/GLP-1/glucagon agonist with 24.2% weight loss in Phase 2, the highest ...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Semaglutide vs Retatrutide vs Tirzepatide: Weight Loss Compared." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: FDA-approved GLP-1 receptor agonist that established the modern weight loss peptide category with.... FDA-approved dual GIP/GLP-1 agonist with up to 20.9% weight loss, currently the most effective ap.... Investigational triple GIP/GLP-1/glucagon agonist with 24.2% weight loss in Phase 2, the highest .... These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: FDA-approved GLP-1 receptor agonist that established the modern weight loss peptide category with 15-17% weight loss in clinical trials. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Peptides in Clinical Trials 2026: The Most Promising Pipeline
A research-focused overview of the most promising peptides in clinical trials as of 2026, including Retatrutide Phase 3 TRIUMPH data, Survodutide, Mazdutide, Ecnoglutide, and other emerging compounds reshaping metabolic medicine.
Weight Loss Peptides: Mechanisms, Evidence, and How They Compare
A mechanism-focused guide to weight loss peptides — how GLP-1, GIP, and glucagon pathways drive fat loss, how single, dual, and triple agonists compare, and what the clinical evidence actually shows.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.
You Might Also Like
Related content you may find interesting