Semaglutide vs Tirzepatide: Comprehensive Comparison of GLP-1 Medications
Evidence-based comparison of semaglutide (Ozempic/Wegovy) and tirzepatide (Mounjaro/Zepbound) for weight loss and type 2 diabetes, including STEP and SURMOUNT trial data.
Verdict at a Glance
Tirzepatide demonstrates greater weight loss and glycemic control than semaglutide in clinical trials, achieving up to 20.9% body weight reduction versus 14.9-16.0% with semaglutide. However, semaglutide has proven cardiovascular benefit (SELECT trial), longer post-marketing safety data, and an oral formulation option. Both are FDA-approved, well-tolerated, and represent major advances in metabolic medicine. The choice between them depends on clinical priorities: maximum weight loss favors tirzepatide, while cardiovascular risk reduction and formulation flexibility favor semaglutide.
| Best for | Pick | Why |
|---|---|---|
| Maximum Weight Loss | Tirzepatide | SURMOUNT-1 demonstrated 20.9% mean weight loss at the 15 mg dose, with up to 36% of patients achieving 25% or more reduction. This exceeds semaglutide's 14.9% in STEP 1. |
| Cardiovascular Risk Reduction | Semaglutide | The SELECT trial (n=17,604) demonstrated a 20% reduction in MACE in overweight/obese adults with established CVD. Tirzepatide's CVOT has not yet reported results. |
| Type 2 Diabetes (Glycemic Control) | Tirzepatide | SURPASS-2 directly compared tirzepatide to semaglutide 1 mg and showed statistically superior HbA1c reduction at all dose levels, with up to 52% of patients achieving normal HbA1c (<5.7%). |
| Oral Medication Preference | Semaglutide | Rybelsus is the only oral GLP-1 agonist available. Tirzepatide is available only as an injectable. Patients who prefer or require oral dosing have semaglutide as the sole option. |
| Established Safety Profile | Semaglutide | Approved since 2017 with over 7 years of post-marketing surveillance, 25,000+ clinical trial participants across SUSTAIN/PIONEER/STEP/SELECT programs, and proven cardiovascular safety and benefit. |
| Treatment-Naive Type 2 Diabetes | Tirzepatide | In SURPASS-1, tirzepatide monotherapy achieved HbA1c reductions of up to 2.07% and body weight reductions of 7.0-9.5 kg, offering robust dual benefit from the outset. |
| Category | Semaglutide | Tirzepatide | Advantage |
|---|---|---|---|
| Mechanism of Action | Selective GLP-1 receptor agonist. Mimics endogenous GLP-1 to enhance glucose-dependent insulin secretion, suppress glucagon, delay gastric emptying, and reduce appetite through hypothalamic signaling. | First-in-class dual GIP and GLP-1 receptor agonist. Activates both incretin pathways simultaneously, with approximately 5-fold greater potency at GIPR relative to native GIP and synergistic metabolic effects. | Tirzepatide |
| Weight Loss Efficacy | STEP 1 demonstrated 14.9% mean weight loss at 68 weeks with 2.4 mg weekly. STEP 3 showed 16.0% with intensive lifestyle intervention. 50.5% of patients achieved 15% or more weight loss in STEP 1. | SURMOUNT-1 demonstrated 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) weight loss at 72 weeks. Up to 36% of participants achieved 25% or more weight loss at the highest dose. | Tirzepatide |
| Glycemic Control | HbA1c reduction of 1.5-1.8% at 1 mg and 2.0-2.2% at 2 mg (SUSTAIN trials). 0.5 mg is the minimum therapeutic dose for T2D. | HbA1c reduction of 1.87-2.01% (5 mg), 2.07-2.24% (10 mg), and 2.30-2.58% (15 mg) in SURPASS trials. Up to 52% of patients achieved HbA1c below 5.7% (normal range) at 15 mg. | Tirzepatide |
| Cardiovascular Evidence | Proven cardiovascular benefit in SELECT trial (17,604 patients): 20% MACE reduction in overweight/obese adults with established CVD. SUSTAIN-6 showed 26% MACE reduction in T2D patients. First anti-obesity drug with proven CV benefit. | No increase in MACE observed in SURPASS trials. Dedicated cardiovascular outcomes trial (SURPASS-CVOT) is underway but not yet completed. CV benefit not yet proven. | Semaglutide |
| Side Effect Profile | GI side effects are dose-dependent. Nausea in 15-44%, vomiting 5-24%, diarrhea 8-30%. Higher rates at the 2.4 mg weight management dose. Well-characterized through 7+ years of post-marketing surveillance. | Similar GI side effect profile. Nausea 12-33%, diarrhea 12-21%, vomiting 5-13%. Comparable or slightly lower GI event rates versus semaglutide in the head-to-head SURPASS-2 trial. Less post-marketing data available. | Tirzepatide |
| Dosing and Formulation | Available as injectable (Ozempic/Wegovy, once weekly) and oral tablet (Rybelsus, daily). Three brand names covering T2D and obesity indications. Multi-dose pens (Ozempic) or single-dose pens (Wegovy). | Injectable only (Mounjaro/Zepbound, once weekly). Single-dose pre-filled pens with hidden needle. Six dose strengths available (2.5-15 mg). No oral formulation. | Semaglutide |

Introduction#
Semaglutide and tirzepatide are the two most prescribed incretin-based medications for weight management and type 2 diabetes, and their comparison is one of the most important questions in metabolic medicine today. Both are FDA-approved, once-weekly injectable medications that have demonstrated substantial weight loss and glycemic improvements in large clinical trial programs.
Semaglutide (marketed as Ozempic, Wegovy, and Rybelsus) is a selective GLP-1 receptor agonist developed by Novo Nordisk. It was the first anti-obesity medication to demonstrate cardiovascular benefit in a dedicated outcomes trial (SELECT, 2023). Tirzepatide (marketed as Mounjaro and Zepbound) is a first-in-class dual GIP/GLP-1 receptor agonist developed by Eli Lilly that has demonstrated the largest body weight reductions of any approved anti-obesity pharmacotherapy, with up to 20.9% mean weight loss in clinical trials.
The SURPASS-2 trial provided the only head-to-head comparison, showing tirzepatide superior to semaglutide 1 mg for both glycemic control and weight loss in type 2 diabetes. However, the comparison is nuanced: semaglutide has longer real-world experience, proven cardiovascular outcomes data, and an oral formulation option that tirzepatide lacks.
Mechanism of Action Comparison#
Semaglutide#
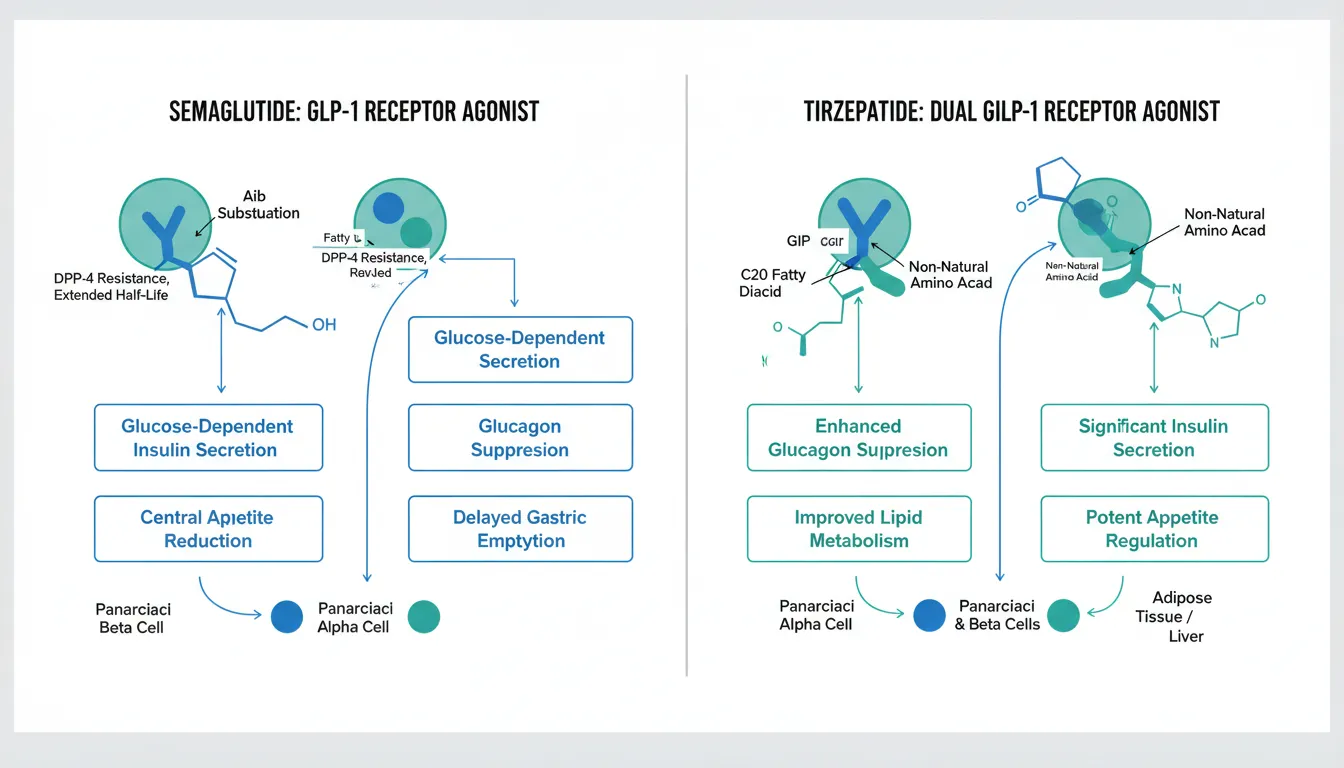
Semaglutide is a selective GLP-1 receptor agonist -- a synthetic analog of human GLP-1(7-37) with two key structural modifications. An alpha-aminoisobutyric acid (Aib) substitution at position 8 provides resistance to degradation by dipeptidyl peptidase-4 (DPP-4), and a C18 fatty diacid chain conjugated at lysine-26 enables non-covalent albumin binding that extends the half-life to approximately 7 days.
By activating GLP-1 receptors, semaglutide produces four key metabolic effects: glucose-dependent insulin secretion from pancreatic beta-cells, suppression of inappropriate glucagon release from alpha-cells, delayed gastric emptying that reduces postprandial glucose excursions and enhances satiety, and central appetite reduction through GLP-1 receptor activation in the hypothalamus and brainstem. The glucose-dependent nature of insulin secretion is clinically important because it minimizes the risk of hypoglycemia compared to insulin or sulfonylureas.
Tirzepatide#
Tirzepatide is a first-in-class dual GIP and GLP-1 receptor agonist. It is a 39-amino-acid synthetic peptide that simultaneously activates both the glucose-dependent insulinotropic polypeptide receptor (GIPR) and the GLP-1 receptor with an imbalanced potency profile -- approximately 5-fold greater potency at GIPR relative to native GIP, while having about 0.2-fold the potency of native GLP-1 at GLP-1R.
This dual agonism represents a fundamentally different approach from single-target GLP-1 agonists. GIPR activation potentiates insulin secretion, may improve lipid metabolism and fat distribution, and enhances central appetite regulation through mechanisms that are complementary to GLP-1R signaling. The synergistic effects of activating both pathways simultaneously produce greater glycemic and weight effects than either pathway alone, as demonstrated in the superior clinical outcomes compared to semaglutide in SURPASS-2.
A C20 fatty diacid modification enables albumin binding and a half-life of approximately 5 days, supporting once-weekly administration similar to semaglutide.
Mechanistic Comparison#
| Feature | Semaglutide | Tirzepatide |
|---|---|---|
| Receptor targets | GLP-1R only | GIP-R + GLP-1R (dual) |
| Molecular size | 31 amino acids (4,114 Da) | 39 amino acids (4,813 Da) |
| Half-life | ~7 days | ~5 days |
| Acylation | C18 fatty diacid at Lys26 | C20 fatty diacid at Lys20 |
| GLP-1R potency | High (designed as selective agonist) | Moderate (~0.2x native GLP-1) |
| GIPR potency | None | High (~5x native GIP) |
| DPP-4 resistance | Aib at position 8 | Aib at position 2 |
| Insulin secretion mechanism | GLP-1R-mediated, glucose-dependent | Dual GLP-1R + GIPR-mediated, glucose-dependent |
Dosing Comparison#
Semaglutide Dosing#
Semaglutide is available in three formulations across two indications:
For type 2 diabetes (Ozempic): Start at 0.25 mg weekly for 4 weeks (tolerability dose), then increase to 0.5 mg. May escalate to 1 mg and then 2 mg at 4-week intervals based on glycemic response. The 0.5 mg dose is the minimum therapeutic dose.
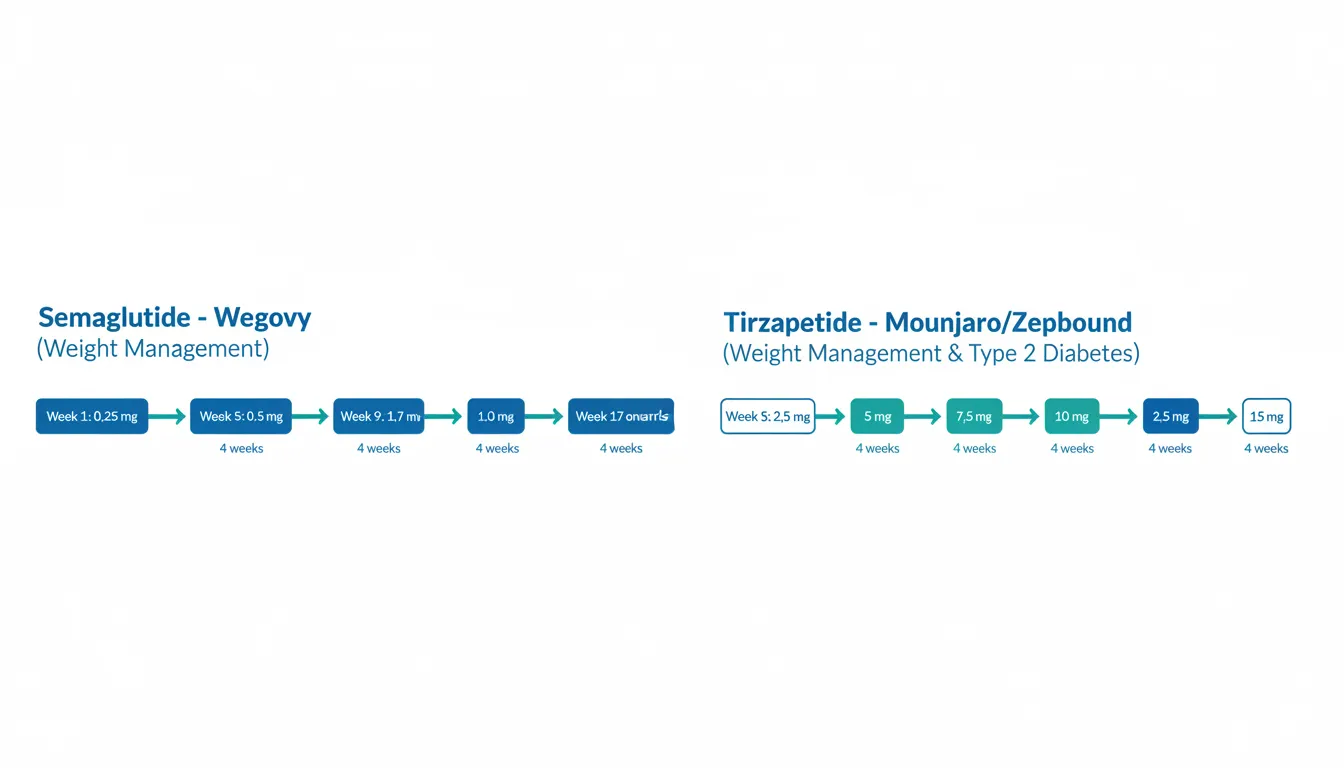
For weight management (Wegovy): A more gradual 16-week escalation from 0.25 mg to the target dose of 2.4 mg weekly (0.25 mg, 0.5 mg, 1.0 mg, 1.7 mg, 2.4 mg at 4-week intervals).
Oral formulation (Rybelsus): Start at 3 mg daily for 30 days, then increase to 7 mg, with optional escalation to 14 mg. Must be taken on an empty stomach with no more than 4 oz of water, 30 minutes before food or other medications.
Semaglutide is supplied as multi-dose pens (Ozempic) and single-dose pens (Wegovy). No reconstitution is required.
Tirzepatide Dosing#
Tirzepatide uses a unified escalation schedule for both indications:
For both T2D (Mounjaro) and weight management (Zepbound): Start at 2.5 mg weekly for 4 weeks, then escalate in 2.5 mg increments at minimum 4-week intervals: 2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg. The 5 mg dose is the first therapeutic dose. Not all patients require the maximum 15 mg dose.
Tirzepatide is supplied exclusively as single-dose pre-filled pens with a hidden needle design. Six pen strengths are available. No oral formulation exists.
Dosing Comparison Table#
| Parameter | Semaglutide | Tirzepatide |
|---|---|---|
| Starting dose | 0.25 mg weekly | 2.5 mg weekly |
| Maximum dose (T2D) | 2 mg weekly | 15 mg weekly |
| Maximum dose (obesity) | 2.4 mg weekly | 15 mg weekly |
| Escalation interval | Minimum 4 weeks per step | Minimum 4 weeks per step |
| Time to maximum dose | 12-16 weeks | 20+ weeks |
| Dose steps | 4 (Ozempic) / 5 (Wegovy) | 6 |
| Oral option available | Yes (Rybelsus 3/7/14 mg daily) | No |
| Pen type | Multi-dose (Ozempic) or single-dose (Wegovy) | Single-dose only |
Side Effects Comparison#
Semaglutide Side Effects#
The GI adverse event profile of semaglutide is well characterized through the SUSTAIN, PIONEER, STEP, and SELECT programs involving over 25,000 participants, plus 7+ years of post-marketing surveillance.
Nausea is the most common adverse event, reported in 15-20% of patients on Ozempic (1 mg) and up to 44% on Wegovy (2.4 mg). Vomiting occurs in 5-24%, diarrhea in 8-30%, and constipation in 5-24%, with higher rates at the weight management dose. Most GI effects are mild to moderate, occur during dose escalation, and diminish with continued treatment. Fewer than 5% of patients in STEP 1 discontinued due to nausea.
Other notable effects include cholelithiasis (1.6% vs 0.7% placebo in STEP 1, related to rapid weight loss), a diabetic retinopathy signal in SUSTAIN-6 (HR 1.76, attributed to rapid HbA1c improvement), and a modest increase in resting heart rate of 2-4 bpm.
Semaglutide carries a boxed warning for thyroid C-cell tumors based on rodent data, though this risk has not been confirmed in over 8 years of human use.
Tirzepatide Side Effects#
Tirzepatide's GI adverse event profile is broadly similar but with some favorable differences. Nausea is reported in 12-33% of patients across the SURPASS and SURMOUNT programs, diarrhea in 12-21%, and vomiting in 5-13%. These rates are generally comparable to or slightly lower than semaglutide at equivalent levels of weight loss efficacy.
In the head-to-head SURPASS-2 trial, tirzepatide demonstrated comparable GI tolerability to semaglutide 1 mg despite producing greater glycemic and weight effects. Fewer than 1% of tirzepatide patients in SURPASS trials discontinued due to nausea at any dose level.
Tirzepatide shares the same boxed warning for thyroid C-cell tumors, similar cholelithiasis risk, and comparable effects on heart rate. Hypoglycemia risk is low as monotherapy but increases with concurrent insulin or sulfonylurea use.
Tirzepatide has less post-marketing surveillance data than semaglutide (approved 2022 vs 2017), meaning rare adverse events may still be identified.
Safety Comparison Table#
| Adverse Event | Semaglutide 2.4 mg | Tirzepatide 15 mg | Notes |
|---|---|---|---|
| Nausea | 44% | 18-33% | Higher semaglutide rates may reflect dose differences |
| Diarrhea | 30% | 14-21% | Similar mechanism |
| Vomiting | 24% | 6-13% | Lower with tirzepatide in trials |
| Constipation | 24% | 6-11% | Lower with tirzepatide |
| Cholelithiasis | 1.6% | ~1.0% | Both related to rapid weight loss |
| Heart rate increase | +2-4 bpm | +2-4 bpm | GLP-1R class effect |
| Discontinuation (GI) | <5% | 4.3-7.1% | Comparable |
| Boxed warning | MTC/MEN2 (thyroid C-cell tumors) | MTC/MEN2 (thyroid C-cell tumors) | Same class warning |
Research Evidence Comparison#
Semaglutide Research#
Semaglutide has one of the most extensive evidence bases of any GLP-1 receptor agonist, with four major phase 3 programs:
SUSTAIN (T2D, injectable): Seven trials enrolling over 4,000 patients, demonstrating HbA1c reductions of 1.2-2.2% across dose levels. SUSTAIN-6 was the cardiovascular safety trial showing 26% MACE reduction.
PIONEER (T2D, oral): Nine trials enrolling over 9,000 patients, validating oral semaglutide efficacy with HbA1c reductions of 1.0-1.4% at the 14 mg dose.
STEP (obesity): Multiple trials enrolling over 5,000 patients, with the pivotal STEP 1 demonstrating 14.9% mean weight loss and STEP 3 showing 16.0% with intensive lifestyle intervention. STEP 5 confirmed sustained 15.2% weight loss at 2 years.
SELECT (CV outcomes): The landmark 17,604-patient trial demonstrating 20% MACE reduction in overweight/obese adults with established CVD but without diabetes -- establishing semaglutide as the first anti-obesity medication with proven cardiovascular benefit.
Evidence level: High -- multiple large RCTs, cardiovascular outcomes data, oral and injectable formulations studied.
Tirzepatide Research#
Tirzepatide's evidence base, while newer, includes pivotal trials that have produced the largest weight reductions of any approved pharmacotherapy:
SURPASS (T2D): Five trials enrolling over 9,000 patients. SURPASS-1 demonstrated HbA1c reductions of up to 2.07% as monotherapy. SURPASS-2 was the critical head-to-head trial showing superiority over semaglutide 1 mg for both HbA1c and weight (tirzepatide 15 mg: -2.46% HbA1c and -12.4 kg vs semaglutide 1 mg: -1.86% and -6.2 kg).
SURMOUNT (obesity): Multiple trials enrolling over 5,000 patients. The pivotal SURMOUNT-1 demonstrated mean weight reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) at 72 weeks, with 36% of patients on the highest dose achieving 25% or more weight loss.
SURPASS-CVOT: A dedicated cardiovascular outcomes trial is underway but results have not yet been reported.
Evidence level: High -- large RCTs with head-to-head data vs semaglutide, but lacking cardiovascular outcomes data.
Head-to-Head: SURPASS-2#
The SURPASS-2 trial is the only direct comparison of tirzepatide and semaglutide, enrolling 1,879 adults with type 2 diabetes. At 40 weeks, all three tirzepatide doses demonstrated statistical superiority over semaglutide 1 mg for HbA1c reduction and weight loss:
| Endpoint | Semaglutide 1 mg | Tirzepatide 5 mg | Tirzepatide 10 mg | Tirzepatide 15 mg |
|---|---|---|---|---|
| HbA1c reduction | -1.86% | -2.01% | -2.24% | -2.46% |
| Weight loss (kg) | -6.2 kg | -7.6 kg | -9.3 kg | -12.4 kg |
| HbA1c <7.0% | 79% | 82% | 86% | 88% |
| HbA1c <5.7% | 19% | 27% | 40% | 46% |
Important caveat: SURPASS-2 compared tirzepatide to semaglutide at 1 mg, not the now-available 2 mg dose for T2D or the 2.4 mg dose for weight management. A head-to-head trial comparing tirzepatide 15 mg to semaglutide 2.4 mg has not been conducted.
Key Differences Summary#
- Receptor pharmacology: Semaglutide is a selective GLP-1 agonist; tirzepatide is a dual GIP/GLP-1 agonist, representing a novel incretin mechanism.
- Weight loss: Tirzepatide produces greater mean weight reduction (20.9% at 15 mg) compared to semaglutide (14.9% at 2.4 mg) in their respective pivotal obesity trials.
- Glycemic control: Tirzepatide demonstrated superior HbA1c reduction versus semaglutide 1 mg in SURPASS-2, with up to 52% of patients achieving normal HbA1c.
- Cardiovascular outcomes: Semaglutide has proven cardiovascular benefit from the SELECT trial (20% MACE reduction). Tirzepatide's CVOT is pending.
- Formulation options: Semaglutide is available as injectable (Ozempic, Wegovy) and oral (Rybelsus). Tirzepatide is injectable only (Mounjaro, Zepbound).
- Market experience: Semaglutide has been available since 2017 with extensive post-marketing data. Tirzepatide was approved in 2022 with less real-world safety experience.
- GI tolerability: SURPASS-2 suggested comparable or slightly better GI tolerability with tirzepatide at equivalent efficacy levels.
- Dose range: Tirzepatide offers more dose granularity with 6 dose levels (2.5-15 mg) compared to semaglutide's 4-5 dose levels.
- Both drugs: Share the same contraindications (MTC/MEN2, pregnancy), similar boxed warnings, and the same general GI side effect profile. Both require dose escalation over weeks to months.
Conclusion#
Semaglutide and tirzepatide are both highly effective, FDA-approved medications for type 2 diabetes and chronic weight management, representing the most significant advances in obesity pharmacotherapy in decades. The evidence consistently shows that tirzepatide produces greater weight loss and glycemic improvement, driven by its novel dual GIP/GLP-1 receptor agonism.
However, the choice between these medications is not simply about maximum efficacy. Semaglutide remains the only incretin-based anti-obesity medication with proven cardiovascular benefit, a distinction that is critically important for patients with established cardiovascular disease. It also offers the unique advantage of an oral formulation (Rybelsus) and has the longest track record of post-marketing safety surveillance.
For patients whose primary goal is maximum weight reduction, tirzepatide at 10-15 mg offers a clear advantage. For patients with established cardiovascular disease requiring evidence-based risk reduction, semaglutide 2.4 mg is the evidence-supported choice until tirzepatide's CVOT reports. For patients who prefer or require oral administration, semaglutide (Rybelsus) is the only option. Both medications should be prescribed by qualified healthcare providers with appropriate dose escalation and monitoring.
It is important to note that the only head-to-head trial (SURPASS-2) compared tirzepatide against semaglutide at 1 mg rather than the higher doses now used for weight management. A direct comparison at maximal obesity doses would provide more definitive guidance for clinical decision-making.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Maximum Weight Loss
Tirzepatide
SURMOUNT-1 demonstrated 20.9% mean weight loss at the 15 mg dose, with up to 36% of patients achieving 25% or more reduction. This exceeds semaglutide's 14.9% in STEP 1.
Cardiovascular Risk Reduction
Semaglutide
The SELECT trial (n=17,604) demonstrated a 20% reduction in MACE in overweight/obese adults with established CVD. Tirzepatide's CVOT has not yet reported results.
Type 2 Diabetes (Glycemic Control)
Tirzepatide
SURPASS-2 directly compared tirzepatide to semaglutide 1 mg and showed statistically superior HbA1c reduction at all dose levels, with up to 52% of patients achieving normal HbA1c (<5.7%).
Oral Medication Preference
Semaglutide
Rybelsus is the only oral GLP-1 agonist available. Tirzepatide is available only as an injectable. Patients who prefer or require oral dosing have semaglutide as the sole option.
Established Safety Profile
Semaglutide
Approved since 2017 with over 7 years of post-marketing surveillance, 25,000+ clinical trial participants across SUSTAIN/PIONEER/STEP/SELECT programs, and proven cardiovascular safety and benefit.
Treatment-Naive Type 2 Diabetes
Tirzepatide
In SURPASS-1, tirzepatide monotherapy achieved HbA1c reductions of up to 2.07% and body weight reductions of 7.0-9.5 kg, offering robust dual benefit from the outset.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Semaglutide vs Tirzepatide: Comprehensive Comparison of GLP-1 Medications
Which is better, Semaglutide or Tirzepatide?
Tirzepatide demonstrates greater weight loss and glycemic control than semaglutide in clinical trials, achieving up to 20.9% body weight reduction versus 14.9-16.0% with semaglutide. However, semaglutide has proven cardiovascular benefit (SELECT trial), longer post-marketing safety data, and an oral formulation option. Both are FDA-approved, well-tolerated, and represent major advances in metabolic medicine. The choice between them depends on clinical priorities: maximum weight loss favors ti... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Semaglutide and Tirzepatide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Tirzepatide; Weight Loss Efficacy: advantage goes to Tirzepatide; Glycemic Control: advantage goes to Tirzepatide. 3 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tirzepatide over Semaglutide?
For the scenario of "Maximum Weight Loss," research data suggests Tirzepatide may be more relevant. SURMOUNT-1 demonstrated 20.9% mean weight loss at the 15 mg dose, with up to 36% of patients achieving 25% or more reduction. This exceeds semaglutide's 14.9% in STEP 1.. This is based on currently available evidence and individual circumstances may differ.
How do Semaglutide and Tirzepatide differ in their mechanisms of action?
Semaglutide: Selective GLP-1 receptor agonist. Mimics endogenous GLP-1 to enhance glucose-dependent insulin secretion, suppress glucagon, delay gastric emptying, and reduce appetite through hypothalamic signaling.. Tirzepatide: First-in-class dual GIP and GLP-1 receptor agonist. Activates both incretin pathways simultaneously, with approximately 5-fold greater potency at GIPR relative to native GIP and synergistic metabol....
Which has fewer side effects, Semaglutide or Tirzepatide?
In terms of side effects and tolerability, the advantage goes to Tirzepatide. Semaglutide: GI side effects are dose-dependent. Nausea in 15-44%, vomiting 5-24%, diarrhea 8-30%. Higher rates at the 2.4 mg weight management dose. Well-chara.... Tirzepatide: Similar GI side effect profile. Nausea 12-33%, diarrhea 12-21%, vomiting 5-13%. Comparable or slightly lower GI event rates versus semaglutide in t....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.