Retatrutide vs Semaglutide: Triple vs Single Agonist Comparison
Retatrutide vs Semaglutide: Evidence-based comparison of the investigational triple GIP/GLP-1/glucagon agonist versus the FDA-approved GLP-1 agonist. Covers weight loss efficacy, cardiovascular data, liver fat reduction, and regulatory status.
Verdict at a Glance
Semaglutide is the established gold standard with FDA approval, proven cardiovascular benefit, extensive clinical data, and multiple formulation options. Retatrutide's triple agonism shows promise for greater weight loss and liver fat reduction, but remains investigational with Phase 2 data only. Phase 3 results will determine whether retatrutide's early advantages translate into meaningful clinical superiority.
| Best for | Pick | Why |
|---|---|---|
| Currently available treatment with proven outcomes | Semaglutide | FDA-approved for diabetes (Ozempic), obesity (Wegovy), and CV risk reduction with 7+ years of clinical and post-marketing data |
| Cardiovascular risk reduction | Semaglutide | SELECT trial demonstrated 20% MACE reduction in 17,604 patients -- the first anti-obesity drug with proven cardiovascular benefit |
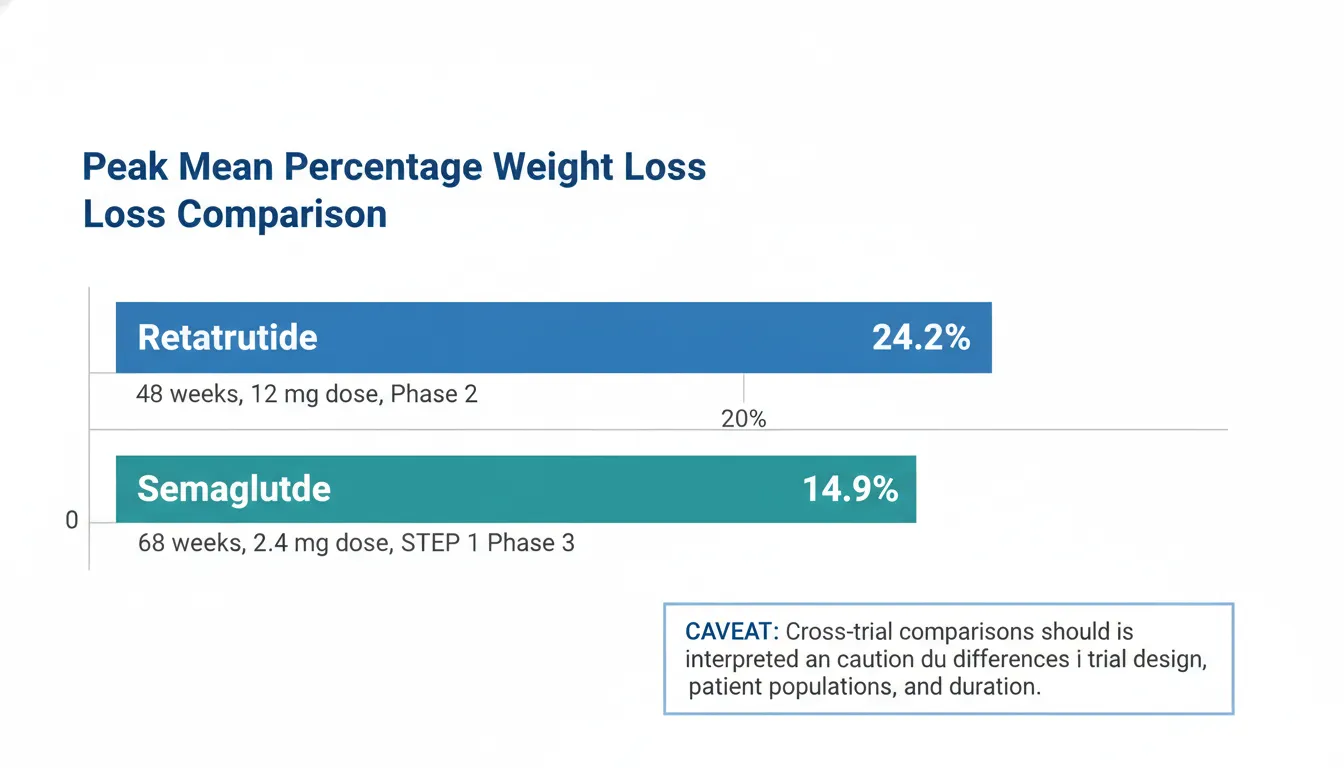
| Maximum weight loss potential | Retatrutide | Phase 2 data showed 24.2% weight loss at 48 weeks with weight curves still declining, though Phase 3 confirmation is required |
| Metabolic liver disease (MASLD/MASH) | Retatrutide | Glucagon receptor agonism directly promotes hepatic fat oxidation, a mechanistic advantage for liver-specific outcomes |
| Oral administration preference | Semaglutide | Only incretin-class drug available as an oral tablet (Rybelsus), with higher-dose oral formulations under development |
| Type 2 diabetes with established treatment guidelines | Semaglutide | Integrated into clinical guidelines with multiple approved doses and formulations, extensive comparative data, and guideline positioning |
| Category | Retatrutide | Semaglutide | Advantage |
|---|---|---|---|
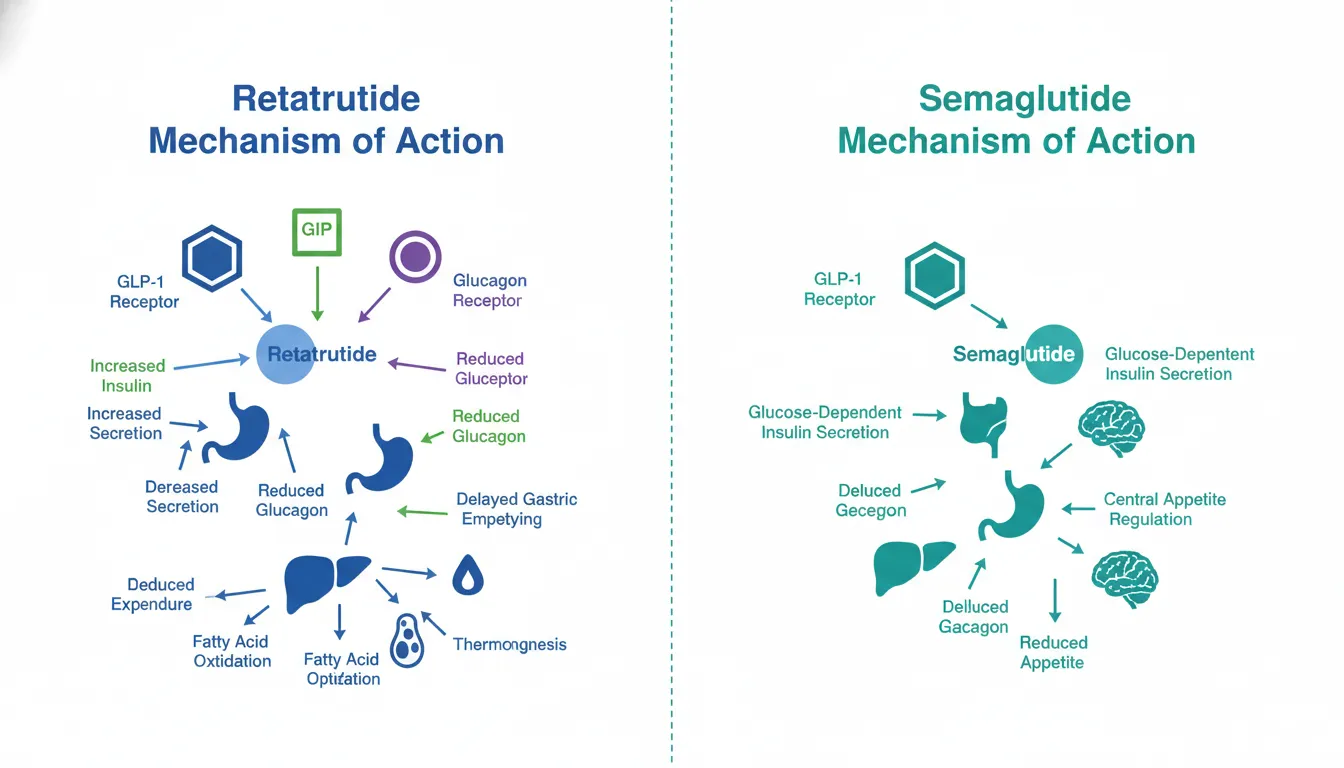
| Mechanism of Action | Triple agonist targeting GIP, GLP-1, and glucagon receptors simultaneously. Glucagon receptor activation adds energy expenditure and hepatic fat oxidation pathways not available with GLP-1 alone. | Selective GLP-1 receptor agonist. Well-characterized mechanism including appetite suppression, glucose-dependent insulin secretion, and gastric emptying delay. | Retatrutide |
| Weight Loss Efficacy | Up to 24.2% body weight loss at 48 weeks in Phase 2 (12 mg dose). Weight curves had not plateaued, suggesting further loss with longer treatment. | 14.9% weight loss at 68 weeks (STEP 1, 2.4 mg). Up to 16% with intensive behavioral therapy (STEP 3). Proven in over 5,000 trial participants. | Retatrutide |
| Cardiovascular Evidence | No cardiovascular outcomes data. Phase 2 only. Small heart rate increases (2-4 bpm) observed, possibly from glucagon component. | SELECT trial (n=17,604) demonstrated 20% MACE reduction in obese adults with CVD. SUSTAIN-6 showed 26% MACE reduction in T2D. First anti-obesity drug with proven CV benefit. | Semaglutide |
| Research Evidence | Phase 2 data in NEJM and Lancet (n=338 obesity, plus T2D trial). Phase 3 ongoing. No post-marketing data. Evidence level rated low. | Over 25,000 participants across SUSTAIN, PIONEER, STEP, and SELECT programs. FDA-approved for three indications. 7+ years post-marketing surveillance. Evidence level rated high. | Semaglutide |
| Liver Fat Reduction | Glucagon receptor activation promotes hepatic fat oxidation. Phase 2 exploratory data showed significant liver fat reduction. MASLD trials planned. | Moderate hepatic fat reduction observed. STEP-NASH showed improvement in steatosis and NASH resolution. Phase 3 liver trials ongoing. | Retatrutide |
| Formulation Options | Once-weekly subcutaneous injection only. Investigational formulation not commercially available. Pre-filled pen expected if approved. | Injectable (Ozempic/Wegovy) and oral tablet (Rybelsus) formulations available. Higher-dose oral (25-50 mg) under investigation for obesity. | Semaglutide |

Introduction#
Retatrutide and semaglutide represent different generations and strategies in incretin-based metabolic therapeutics. Semaglutide, a selective GLP-1 receptor agonist marketed as Ozempic, Wegovy, and Rybelsus, is one of the most extensively studied anti-obesity and anti-diabetes medications in history, with over 25,000 clinical trial participants and FDA approval for three distinct indications. Retatrutide, an investigational triple GIP/GLP-1/glucagon receptor agonist developed by Eli Lilly, demonstrated unprecedented weight loss in Phase 2 trials but has not yet completed Phase 3 development.
This comparison examines whether retatrutide's triple agonist mechanism offers clinically meaningful advantages over semaglutide's proven single-agonist approach, while acknowledging the fundamental asymmetry in evidence quality between a fully approved drug and an investigational compound.
Cross-trial comparisons must be interpreted with caution. Differences in trial design, participant populations, treatment duration, and endpoints mean that direct numerical comparisons between retatrutide Phase 2 data and semaglutide Phase 3 data are hypothesis-generating, not definitive.
Mechanism of Action Comparison#
Retatrutide#
Retatrutide (LY3437943) is a 39-amino acid synthetic peptide that simultaneously activates three metabolically important receptors:
- GLP-1 receptor: Enhances glucose-dependent insulin secretion, suppresses glucagon, slows gastric emptying, and reduces appetite through hypothalamic and brainstem signaling
- GIP receptor: Potentiates insulin secretion, may improve beta-cell survival, and contributes to adipose tissue metabolism and central appetite regulation
- Glucagon receptor: Increases hepatic energy expenditure, promotes fatty acid oxidation in the liver, stimulates thermogenesis in brown adipose tissue, and enhances lipolysis
The glucagon receptor component is the defining innovation. While glucagon traditionally raises blood glucose, the concurrent GLP-1 and GIP agonism counterbalances this hyperglycemic effect, allowing retatrutide to achieve net glycemic improvement while harnessing glucagon's catabolic benefits for energy expenditure and liver fat clearance. This creates a dual metabolic lever: reduced energy intake (via GLP-1/GIP appetite suppression) combined with increased energy output (via glucagon-mediated thermogenesis).
A C18 fatty acid modification at Lys30 enables albumin binding and a half-life of approximately 6 days, supporting once-weekly dosing.
Semaglutide#
Semaglutide is a 31-amino acid GLP-1(7-37) analog with two key structural modifications: an Aib substitution at position 8 for DPP-4 resistance, and a C18 fatty diacid at Lys26 for albumin binding and a half-life of approximately 7 days.
Semaglutide selectively activates the GLP-1 receptor, producing:
- Glucose-dependent insulin secretion: Reduces hypoglycemia risk compared to non-incretin agents
- Glucagon suppression: Reduces hepatic glucose output in the hyperglycemic state
- Gastric emptying delay: Contributes to postprandial glucose control and satiety
- Central appetite regulation: Acts on GLP-1 receptors in the hypothalamus and brainstem to reduce hunger and alter food preferences
The simplicity of semaglutide's single-receptor mechanism is both a limitation (no energy expenditure enhancement from glucagon) and a strength (thoroughly understood pharmacology, predictable effects, extensive safety characterization).
Receptor Comparison#
| Feature | Retatrutide | Semaglutide |
|---|---|---|
| GLP-1 receptor | Yes | Yes |
| GIP receptor | Yes | No |
| Glucagon receptor | Yes | No |
| Energy intake reduction | Yes (GLP-1/GIP) | Yes (GLP-1) |
| Energy expenditure increase | Yes (glucagon) | No |
| Hepatic fat oxidation | Yes (glucagon) | Indirect only |
| Half-life | ~6 days | ~7 days |
| Dosing frequency | Once weekly | Once weekly (injectable) |
Weight Loss Efficacy#
Retatrutide Phase 2 Results#
The Phase 2 obesity trial (Jastreboff et al., NEJM 2023; n=338) demonstrated dose-dependent weight loss over 48 weeks:
| Dose | Weight Loss at 48 Weeks |
|---|---|
| Placebo | ~2.1% |
| 1 mg | ~8.7% |
| 4 mg | ~17.1% |
| 8 mg | ~22.1% |
| 12 mg | ~24.2% |
The 24.2% weight loss at the 12 mg dose was the largest mean weight loss reported for any anti-obesity medication at the time of publication. Notably, weight loss curves in the higher dose groups had not fully plateaued at 48 weeks, suggesting that additional weight loss might be achieved with longer treatment. Approximately 83% of participants in the 12 mg group lost at least 15% of body weight, and 26% lost 30% or more.
Semaglutide Phase 3 Results#
Semaglutide's weight loss data come from the much larger STEP program:
| Trial | Population | Weight Loss | Duration |
|---|---|---|---|
| STEP 1 (n=1,961) | Obesity without T2D | 14.9% | 68 weeks |
| STEP 2 (n=1,210) | Obesity with T2D | 9.6% | 68 weeks |
| STEP 3 (n=611) | Obesity + intensive behavioral therapy | 16.0% | 68 weeks |
| STEP 5 (n=304) | Obesity without T2D (2-year) | 15.2% | 104 weeks |
In STEP 1, 86.4% achieved at least 5% weight loss, 69.1% achieved at least 10%, and 50.5% achieved at least 15%.
Cross-Trial Context#
Retatrutide's 24.2% weight loss at 48 weeks appears numerically superior to semaglutide's 14.9% at 68 weeks, but several factors complicate direct comparison:
- Trial phase: Phase 2 trials often yield more favorable results than Phase 3 (smaller, more controlled populations)
- Treatment duration: Semaglutide data are at 68-104 weeks; retatrutide data are at 48 weeks only
- Population differences: Participant demographics, baseline BMI, and comorbidity profiles may differ
- Dose optimization: Retatrutide's Phase 3 may use different doses than Phase 2
A head-to-head randomized trial would be needed to definitively establish relative efficacy.
Dosing Comparison#
Retatrutide Dosing#
Based on Phase 2 clinical trial protocols (investigational only):
- Starting dose: 0.5 mg weekly subcutaneous injection
- Escalation: Gradual increase over 12-24 weeks to target dose (up to 12 mg)
- Target doses tested: 1, 4, 8, and 12 mg weekly
- Escalation rationale: Extended 24-week escalation for higher doses reduces GI side effects compared to faster 12-week escalation
No commercial formulation exists. No dose adjustment guidelines, missed dose protocols, or special population recommendations have been established.
Semaglutide Dosing#
FDA-approved dosing with established protocols:
- Ozempic (T2D): Start 0.25 mg weekly, escalate to 0.5-2 mg over 8-16 weeks
- Wegovy (obesity): Start 0.25 mg weekly, escalate through 0.5, 1.0, 1.7, to 2.4 mg maintenance over 16 weeks
- Rybelsus (oral T2D): Start 3 mg daily, escalate to 7-14 mg daily over 30-60 days
Semaglutide benefits from established guidelines for missed doses, switching between formulations, special populations (renal/hepatic impairment, elderly), and drug interactions. Pre-filled pen delivery systems are commercially available.
Side Effects Comparison#
Retatrutide Side Effects#
Phase 2 data (n=338 obesity trial):
- Nausea: ~25% at higher doses (8-12 mg)
- Diarrhea: ~20%
- Vomiting: ~15%
- Constipation: Common
- Decreased appetite: Common (pharmacological effect)
- Heart rate: Small increase (2-4 bpm), potentially related to glucagon component
- Injection site reactions: Mild, transient
- Discontinuation rate: 6-10% due to adverse events
The glucagon receptor component introduces theoretical concerns for hyperglycemia (counterbalanced by GLP-1/GIP in practice), cardiovascular effects (chronotropic glucagon action), and hepatic effects, none of which produced safety signals in Phase 2 but require larger-scale monitoring.
Semaglutide Side Effects#
Extensively characterized across 25,000+ trial participants and 7+ years post-marketing:
- Nausea: 15-44% depending on dose (highest with Wegovy 2.4 mg)
- Vomiting: 5-24%
- Diarrhea: 8-30%
- Constipation: 5-24%
- Heart rate: 2-4 bpm increase (GLP-1 class effect)
- Cholelithiasis: 1.6% vs 0.7% placebo (associated with rapid weight loss)
- Diabetic retinopathy: HR 1.76 in SUSTAIN-6 (attributed to rapid HbA1c improvement)
- Pancreatitis: Rare (<0.2%)
- Boxed warning: Thyroid C-cell tumors (rodent data; not confirmed in humans)
Semaglutide's safety profile is well understood, with known risks that can be monitored and managed. Post-marketing surveillance continues to identify rare signals (e.g., ileus, aspiration during anesthesia).
Research Evidence Comparison#
Retatrutide Research#
The retatrutide evidence base consists of three principal publications:
- Coskun et al. (2022) in Molecular Metabolism: Preclinical characterization and Phase 1 first-in-human study establishing pharmacology, pharmacokinetics, and initial safety
- Jastreboff et al. (2023) in NEJM: Phase 2 obesity trial (n=338) demonstrating dose-dependent weight loss up to 24.2% at 48 weeks
- Rosenstock et al. (2023) in The Lancet: Phase 2 T2D trial showing significant HbA1c reductions and body weight loss, with exploratory liver fat reduction data
Evidence level: Low (Phase 2 only). Phase 3 trials are ongoing with estimated completion in 2025-2026.
Semaglutide Research#
Semaglutide has one of the largest clinical evidence bases in metabolic medicine:
- SUSTAIN program: 7 Phase 3 trials in T2D (n>4,000) including CV outcomes (SUSTAIN-6)
- PIONEER program: 10 Phase 3 trials of oral formulation in T2D (n>9,000)
- STEP program: 5+ Phase 3 trials in obesity (n>5,000)
- SELECT trial: Cardiovascular outcomes in obesity (n=17,604), demonstrating 20% MACE reduction
- Additional studies: FLOW (renal outcomes), STEP-NASH (liver disease), HFpEF studies
Evidence level: High. FDA-approved for three indications with multiple active-comparator trials, cardiovascular outcomes data, and extensive post-marketing surveillance.
Evidence Asymmetry#
The fundamental challenge in this comparison is the vast asymmetry in evidence maturity. Semaglutide's efficacy and safety are established through tens of thousands of participant-years of exposure across diverse populations. Retatrutide's data come from approximately 338 obesity trial participants followed for 48 weeks. This asymmetry means that while retatrutide's Phase 2 numbers are numerically impressive, they carry substantially more uncertainty than semaglutide's Phase 3 results.
Liver Fat and MASLD#
One area where retatrutide may hold a mechanistic advantage is liver fat reduction. Glucagon receptor activation directly promotes hepatic fatty acid oxidation, a pathway not engaged by GLP-1 alone. In the Phase 2 T2D trial, exploratory analyses showed significant reductions in liver fat content with retatrutide.
Semaglutide has also shown benefits for hepatic steatosis. The STEP-NASH trial demonstrated improvement in NASH resolution and fibrosis. However, semaglutide's liver effects are largely indirect, mediated through weight loss and improved metabolic parameters rather than direct hepatic lipid oxidation.
Dedicated MASLD/MASH trials for both compounds will clarify whether retatrutide's glucagon-mediated hepatic fat clearance translates into superior histological outcomes.
Key Differences Summary#
| Feature | Retatrutide | Semaglutide |
|---|---|---|
| Receptor targets | GIP + GLP-1 + Glucagon | GLP-1 only |
| Development stage | Phase 2 complete, Phase 3 ongoing | FDA-approved (3 indications) |
| Weight loss (best reported) | 24.2% at 48 weeks (Phase 2) | 14.9-16.0% at 68 weeks (Phase 3) |
| CV outcomes data | None | SELECT (20% MACE reduction, n=17,604) |
| Evidence level | Low | High |
| Total trial participants | ~700 (Phase 1-2) | >25,000 |
| Liver fat mechanism | Direct (glucagon receptor) | Indirect (weight loss mediated) |
| Formulation options | SC injection only (investigational) | SC injection + oral tablet |
| Post-marketing data | None | 7+ years |
| Energy expenditure | Increased (glucagon) | Not significantly affected |
| Dose escalation period | 12-24 weeks | 16 weeks (Wegovy) |
| Manufacturer | Eli Lilly | Novo Nordisk |
Conclusion#
Semaglutide is the established standard of care with an unmatched evidence base in metabolic therapeutics. Its three FDA approvals, proven cardiovascular benefit in the SELECT trial, oral formulation option, and extensive post-marketing data make it the reference against which all next-generation compounds must be measured. For patients needing treatment today, semaglutide offers a thoroughly validated option with well-understood benefits and risks.
Retatrutide's triple agonist mechanism represents the next potential frontier. Its Phase 2 weight loss data (24.2% at 48 weeks) and mechanistic advantages in hepatic fat reduction through glucagon receptor activation suggest it could surpass semaglutide's efficacy if Phase 3 results confirm the Phase 2 findings. The addition of energy expenditure enhancement via glucagon agonism addresses a limitation inherent to GLP-1-only approaches, which reduce energy intake but do not meaningfully increase energy output.
However, the evidence gap between these compounds cannot be overstated. Semaglutide's data are built on over 25,000 participants across more than 20 randomized controlled trials, including the largest cardiovascular outcomes trial ever conducted for an anti-obesity medication. Retatrutide's data come from a single Phase 2 trial of 338 participants. Until Phase 3 data are available, and particularly until head-to-head comparisons and cardiovascular outcomes trials are completed, retatrutide's apparent advantages remain preliminary and unconfirmed.
The metabolic therapeutics field will be shaped significantly by whether retatrutide's Phase 3 results validate its Phase 2 promise, potentially establishing triple agonism as the next evolution beyond semaglutide's proven single-agonist approach.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Currently available treatment with proven outcomes
Semaglutide
FDA-approved for diabetes (Ozempic), obesity (Wegovy), and CV risk reduction with 7+ years of clinical and post-marketing data
Cardiovascular risk reduction
Semaglutide
SELECT trial demonstrated 20% MACE reduction in 17,604 patients -- the first anti-obesity drug with proven cardiovascular benefit
Maximum weight loss potential
Retatrutide
Phase 2 data showed 24.2% weight loss at 48 weeks with weight curves still declining, though Phase 3 confirmation is required
Metabolic liver disease (MASLD/MASH)
Retatrutide
Glucagon receptor agonism directly promotes hepatic fat oxidation, a mechanistic advantage for liver-specific outcomes
Oral administration preference
Semaglutide
Only incretin-class drug available as an oral tablet (Rybelsus), with higher-dose oral formulations under development
Type 2 diabetes with established treatment guidelines
Semaglutide
Integrated into clinical guidelines with multiple approved doses and formulations, extensive comparative data, and guideline positioning
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Retatrutide vs Semaglutide: Triple vs Single Agonist Comparison
Which is better, Retatrutide or Semaglutide?
Semaglutide is the established gold standard with FDA approval, proven cardiovascular benefit, extensive clinical data, and multiple formulation options. Retatrutide's triple agonism shows promise for greater weight loss and liver fat reduction, but remains investigational with Phase 2 data only. Phase 3 results will determine whether retatrutide's early advantages translate into meaningful clinical superiority. Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Retatrutide and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Retatrutide; Weight Loss Efficacy: advantage goes to Retatrutide; Cardiovascular Evidence: advantage goes to Semaglutide. 3 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Retatrutide?
For the scenario of "Currently available treatment with proven outcomes," research data suggests Semaglutide may be more relevant. FDA-approved for diabetes (Ozempic), obesity (Wegovy), and CV risk reduction with 7+ years of clinical and post-marketing data. This is based on currently available evidence and individual circumstances may differ.
How do Retatrutide and Semaglutide differ in their mechanisms of action?
Retatrutide: Triple agonist targeting GIP, GLP-1, and glucagon receptors simultaneously. Glucagon receptor activation adds energy expenditure and hepatic fat oxidation pathways not available with GLP-1 alone.. Semaglutide: Selective GLP-1 receptor agonist. Well-characterized mechanism including appetite suppression, glucose-dependent insulin secretion, and gastric emptying delay..
In what scenario might Semaglutide be preferred?
For "Cardiovascular risk reduction," Semaglutide may be more appropriate. SELECT trial demonstrated 20% MACE reduction in 17,604 patients -- the first anti-obesity drug with proven cardiovascular benefit. Individual factors and clinical context should guide any decisions.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.