Cagrilintide + Semaglutide (CagriSema): Dual-Agonist Weight Management Research

Introduction#
The combination of cagrilintide and semaglutide -- branded CagriSema -- represents one of the most significant developments in peptide-based weight management research. Unlike the empirical "stacking" approaches common with other peptide combinations, CagriSema is a pharmaceutical-grade, fixed-dose combination that has undergone rigorous Phase 3 clinical testing with thousands of participants.
The REDEFINE clinical trial program, with results published in the New England Journal of Medicine in 2025, demonstrated weight loss exceeding 20% in the majority of treated patients, establishing CagriSema as a potential next-generation obesity treatment combining two distinct hormonal pathways.
This guide reviews the clinical evidence, explains the dual-mechanism rationale, and examines the implications for the broader field of peptide-based metabolic research.
The Two Components#
Semaglutide: GLP-1 Receptor Agonist#
Semaglutide is a well-established GLP-1 (glucagon-like peptide-1) receptor agonist already FDA-approved for both type 2 diabetes (Ozempic) and chronic weight management (Wegovy) at the 2.4 mg weekly dose.
Mechanism of action:
- Activates GLP-1 receptors in the pancreas, gut, and brain
- Enhances glucose-dependent insulin secretion
- Suppresses glucagon release
- Slows gastric emptying, promoting satiety
- Acts on hypothalamic appetite centers to reduce food intake
Established efficacy: The STEP clinical trial program demonstrated that semaglutide 2.4 mg weekly produces approximately 15-17% weight loss from baseline over 68 weeks in adults with obesity.
Semaglutide's role in CagriSema builds on this proven foundation, providing the GLP-1 pathway component of the dual-agonist approach.
Cagrilintide: Long-Acting Amylin Analog#
Cagrilintide is a long-acting analog of amylin, a 37-amino-acid peptide hormone co-secreted with insulin from pancreatic beta cells. While amylin analogs are not new -- pramlintide (Symlin) was FDA-approved in 2005 for diabetes -- cagrilintide represents a significant pharmacokinetic advance that enables once-weekly dosing.
Mechanism of action:
- Activates amylin receptors (calcitonin receptor + RAMP complexes) in the area postrema and other brainstem regions
- Slows gastric emptying through vagal pathways
- Suppresses postprandial glucagon secretion
- Reduces food intake through central appetite-regulating circuits
- May influence reward-based eating behavior through brainstem-to-limbic signaling
The amylin deficit in obesity: Amylin secretion is often dysregulated in obesity and type 2 diabetes. In advanced diabetes, beta-cell dysfunction leads to reduced amylin output, which may contribute to impaired satiety signaling and postprandial glucose excursions.
The Rationale for Dual-Agonist Combination#
Complementary Satiety Pathways#
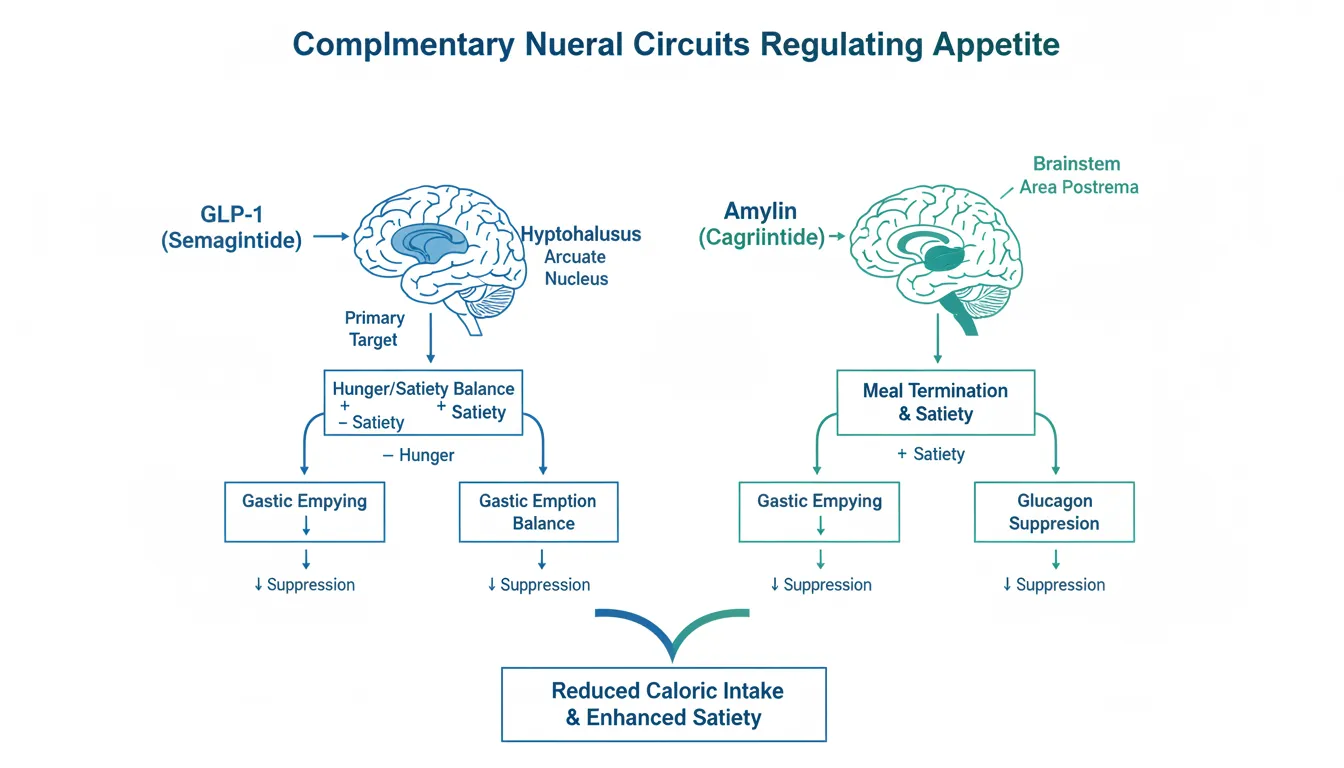
While both GLP-1 and amylin reduce appetite, they do so through partially distinct neural circuits:
| Feature | Semaglutide (GLP-1) | Cagrilintide (Amylin) |
|---|---|---|
| Primary brain target | Hypothalamus (arcuate nucleus) | Area postrema / brainstem |
| Appetite mechanism | Reduces hunger drive | Enhances meal-ending satiety |
| Gastric emptying | Slows moderately | Slows significantly |
| Glucagon effect | Suppresses fasting glucagon | Suppresses postprandial glucagon |
| Insulin effect | Enhances glucose-dependent secretion | Co-secreted with insulin |
| Reward eating | Some evidence of reduction | Emerging evidence of brainstem-limbic effects |
The key insight is that GLP-1 and amylin act on different nodes of the appetite-regulation network. GLP-1 primarily influences the hypothalamic hunger/satiety balance, while amylin acts through brainstem circuits that control meal termination. Targeting both simultaneously may produce a more complete suppression of excess caloric intake than either pathway alone.
Beyond Additive Effects#
The REDEFINE trials demonstrated that CagriSema produced weight loss (20.4%) that exceeded what would be expected from simple addition of semaglutide monotherapy (~17%) and cagrilintide monotherapy (~6-8%). This suggests genuine pharmacological synergism between the two pathways, though the mechanisms underlying this supra-additive effect are still being characterized.
REDEFINE Clinical Trial Results#
REDEFINE 1: Adults with Obesity (No Diabetes)#
Published in the New England Journal of Medicine in 2025 1.
Trial design:
- Phase 3a, randomized, double-blind, placebo-controlled
- 68-week treatment duration
- 3,417 adults with BMI 30 or higher, or BMI 27 or higher with at least one obesity-related complication
- Arms: CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg), semaglutide alone, cagrilintide alone, or placebo
- All groups received lifestyle intervention
Primary weight loss results:
- CagriSema: -20.4% mean body weight change from baseline
- Placebo: -3.0% mean body weight change from baseline
- Treatment difference: -17.4 percentage points (p < 0.001)
Weight loss thresholds achieved with CagriSema:
- 60% of participants lost at least 20% of body weight
- 23% of participants lost 30% or more of body weight
- These thresholds approach the range previously achievable only through bariatric surgery
Metabolic improvements:
- Significant reductions in systolic blood pressure
- Improved waist circumference
- Improved lipid profiles
- 88% of participants with prediabetes at baseline returned to normoglycemia
REDEFINE 2: Adults with Obesity and Type 2 Diabetes#
Also published in the New England Journal of Medicine in 2025 2.
Trial design:
- Phase 3a, double-blind, randomized, placebo-controlled
- 68-week treatment duration
- Adults with BMI 27 or higher, HbA1c 7-10%, and type 2 diabetes
- CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg) vs. placebo, 3:1 randomization
Weight loss results:
- CagriSema: -13.7% mean body weight change from baseline
- Placebo: -3.4% mean body weight change from baseline
Glycemic control:
- 73.5% of CagriSema patients achieved HbA1c of 6.5% or less
- 15.9% of placebo patients achieved HbA1c of 6.5% or less
- The dual pathway approach provided both weight loss and significant glycemic improvement
Why less weight loss than REDEFINE 1: The lower weight loss in the diabetes population (13.7% vs. 20.4%) is consistent with the known phenomenon of reduced weight loss efficacy of GLP-1 agonists in patients with type 2 diabetes, likely related to insulin resistance and metabolic adaptation.
Safety and Tolerability#
Gastrointestinal Events#
The most common adverse effects were gastrointestinal in nature, consistent with the mechanisms of both components:
- CagriSema group: 79.6% reported GI adverse events
- Placebo group: 39.9% reported GI adverse events
- Events were predominantly mild to moderate in severity
- Most events occurred during the dose-escalation phase and were transient
- Nausea, diarrhea, and vomiting were the most frequently reported events
Comparison with Semaglutide Alone#
The GI adverse event rate with CagriSema was higher than with semaglutide alone, which is expected given the additive gastric emptying effects of both components. However, the rate of treatment discontinuation due to adverse events was not dramatically higher, suggesting that the tolerability profile remains manageable.
Other Safety Considerations#
- No new safety signals beyond those known for GLP-1 and amylin agonists individually
- Cardiovascular outcomes data from dedicated CVOT trials are pending
- Long-term (multi-year) safety data is not yet available
- The theoretical risk of pancreatitis associated with GLP-1 agonists applies to the combination
- Effects on muscle mass and bone density during weight loss warrant monitoring
How CagriSema Compares to Other Approaches#
| Treatment | Mechanism | Mean Weight Loss | Phase | Status |
|---|---|---|---|---|
| CagriSema | GLP-1 + Amylin | ~20% (68 wk) | Phase 3 | NDA submitted |
| Semaglutide 2.4 mg | GLP-1 | ~17% (68 wk) | Approved | FDA-approved (Wegovy) |
| Tirzepatide 15 mg | GLP-1 + GIP | ~20.9% (72 wk) | Approved | FDA-approved (Zepbound) |
| Retatrutide | GLP-1 + GIP + Glucagon | ~24% (48 wk) | Phase 3 | In trials |
| Survodutide | GLP-1 + Glucagon | ~19% (46 wk) | Phase 3 | In trials |
| Orforglipron (oral) | GLP-1 (oral) | ~14.7% (72 wk) | Phase 3 | In trials |
| Bariatric surgery | Mechanical + hormonal | ~25-35% (long-term) | Established | Standard of care |
CagriSema occupies a unique position as the first dual GLP-1/amylin combination. While tirzepatide and retatrutide target incretin receptors (GIP, glucagon), CagriSema targets amylin -- a fundamentally different hormonal pathway. This may make CagriSema particularly relevant for patients who have plateaued on GLP-1 monotherapy.
Implications for Peptide Research#
Validation of Combination Approaches#
CagriSema represents perhaps the strongest validation of peptide combination therapy in any field. Unlike most "stacks" discussed in the peptide research community, CagriSema has:
- Randomized, placebo-controlled Phase 3 data with thousands of participants
- Publication in the New England Journal of Medicine
- Regulatory submission (NDA) filed with the FDA
- Manufacturing under pharmaceutical-grade conditions
- Head-to-head data against monotherapy components
This sets a standard for what rigorous combination testing looks like and highlights the gap between pharmaceutical-grade evidence and the anecdotal data available for most other peptide combinations.
The Amylin Pathway#
CagriSema has renewed interest in amylin biology. While pramlintide (Symlin) was approved in 2005, it never achieved widespread adoption due to its short half-life requiring multiple daily injections. Cagrilintide's once-weekly pharmacokinetics solved this practical limitation, demonstrating that delivery optimization can revive a therapeutically relevant but pharmacologically inconvenient pathway.
Combination Design Principles#
The CagriSema program illustrates key principles for effective peptide combinations:
- Target distinct but converging pathways: GLP-1 and amylin act through different receptor systems but converge on appetite regulation
- Complementary, not redundant, mechanisms: The two agents reduce food intake through different neural circuits
- Matched pharmacokinetics: Both components are formulated for once-weekly administration
- Rigorous dose optimization: Each component was separately optimized before combination testing
- Systematic comparison: The REDEFINE program included monotherapy arms to quantify the combination benefit
Regulatory Status and Timeline#
Novo Nordisk submitted a New Drug Application (NDA) to the FDA for CagriSema in 2025 for the indication of excess body weight reduction in adults with obesity or overweight with at least one weight-related comorbid condition 3.
If approved, CagriSema would become the first injectable combination of a GLP-1 receptor agonist and an amylin analog available for weight management. The fixed-dose combination in a single pen would offer convenience over separate injections of each component.
Key Takeaways for Researchers#
-
CagriSema has the strongest clinical evidence of any peptide combination discussed in the weight management space, with Phase 3 data from thousands of participants published in the New England Journal of Medicine.
-
The dual GLP-1/amylin approach produces supra-additive weight loss. The 20.4% mean weight loss exceeds what would be expected from adding the individual effects, suggesting genuine pharmacological synergism.
-
Amylin and GLP-1 target different appetite circuits. GLP-1 primarily acts on hypothalamic hunger/satiety centers, while amylin acts through brainstem meal-termination pathways. This complementarity explains the enhanced efficacy.
-
GI tolerability is the primary trade-off. Nearly 80% of participants experienced gastrointestinal side effects, though most were transient and manageable.
-
CagriSema sets the evidence standard for peptide combination therapy. The contrast between this program's rigor and the anecdotal evidence base for most other peptide "stacks" is instructive for the field.
-
Long-term data is still pending. Multi-year safety outcomes, cardiovascular event data, and durability of weight loss after treatment cessation are not yet established.
-
Competition in the obesity peptide space is intense. Tirzepatide, retatrutide, survodutide, and oral GLP-1 agonists are all advancing, making this a rapidly evolving field where comparative data will be critical.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
Footnotes#
-
Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity (REDEFINE 1). New England Journal of Medicine. DOI: 10.1056/NEJMoa2502081. 2025. ↩
-
Cagrilintide-Semaglutide in Adults with Overweight or Obesity and Type 2 Diabetes (REDEFINE 2). New England Journal of Medicine. PMID: 40544432. 2025. ↩
-
Novo Nordisk files for FDA approval of CagriSema, the first once-weekly combination of GLP-1 and amylin analogues for weight management. Novo Nordisk Press Release. 2025. ↩

{kind=link}
Frequently Asked Questions About Cagrilintide + Semaglutide (CagriSema): Dual-Agonist Weight Management Research
What does this article cover?
A comprehensive review of the cagrilintide and semaglutide combination (CagriSema), covering the REDEFINE Phase 3 trial results, dual amylin-GLP-1 mechanisms, weight loss efficacy data, and regulatory status. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide. Key context: Semaglutide (FDA-approved GLP-1 receptor agonist and core component of the CagriSema combination). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Cagrilintide + Semaglutide (CagriSema): Dual-Agonist Weight Management Research." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: FDA-approved GLP-1 receptor agonist and core component of the CagriSema combination. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.

Retatrutide Canada Guide
Retatrutide in Canada: Everything You Need to Know — part of the Next-Gen Weight Loss content cluster.
You Might Also Like
Related content you may find interesting