5 Most Promising Peptides for Weight Loss (Evidence-Based)

Introduction#
The landscape of peptide-based weight loss research has transformed dramatically since 2020. What began with single-receptor agonists has evolved into a pipeline of dual and triple receptor agonists, each pushing the boundaries of what pharmacological weight management can achieve.
This evidence-based review examines five peptides with the strongest clinical evidence for weight loss, ranked by the quality and recency of their research data. All weight loss percentages cited come from peer-reviewed clinical trials.
Important: This article is for educational purposes only. Only two of these peptides (semaglutide and tirzepatide) are currently FDA-approved. The others remain investigational.
1. Tirzepatide (Zepbound / Mounjaro)#
Mechanism: Dual GIP/GLP-1 receptor agonist FDA Status: Approved for type 2 diabetes (Mounjaro) and chronic weight management (Zepbound) Evidence Level: High (Phase 3 completed, FDA-approved)
Tirzepatide has emerged as the most effective FDA-approved peptide for weight loss based on head-to-head clinical trial data.
Key Clinical Evidence#
The SURMOUNT-5 trial (2025) directly compared tirzepatide against semaglutide in adults with obesity. At 72 weeks, participants on tirzepatide achieved -20.2% body weight loss compared to -13.7% with semaglutide 1. This 6.5 percentage point difference was statistically significant.
A 2025 systematic review and meta-analysis confirmed tirzepatide's superiority, finding a mean difference of 4.23 percentage points greater weight loss compared to semaglutide (P < 0.01) 2.
How It Works#
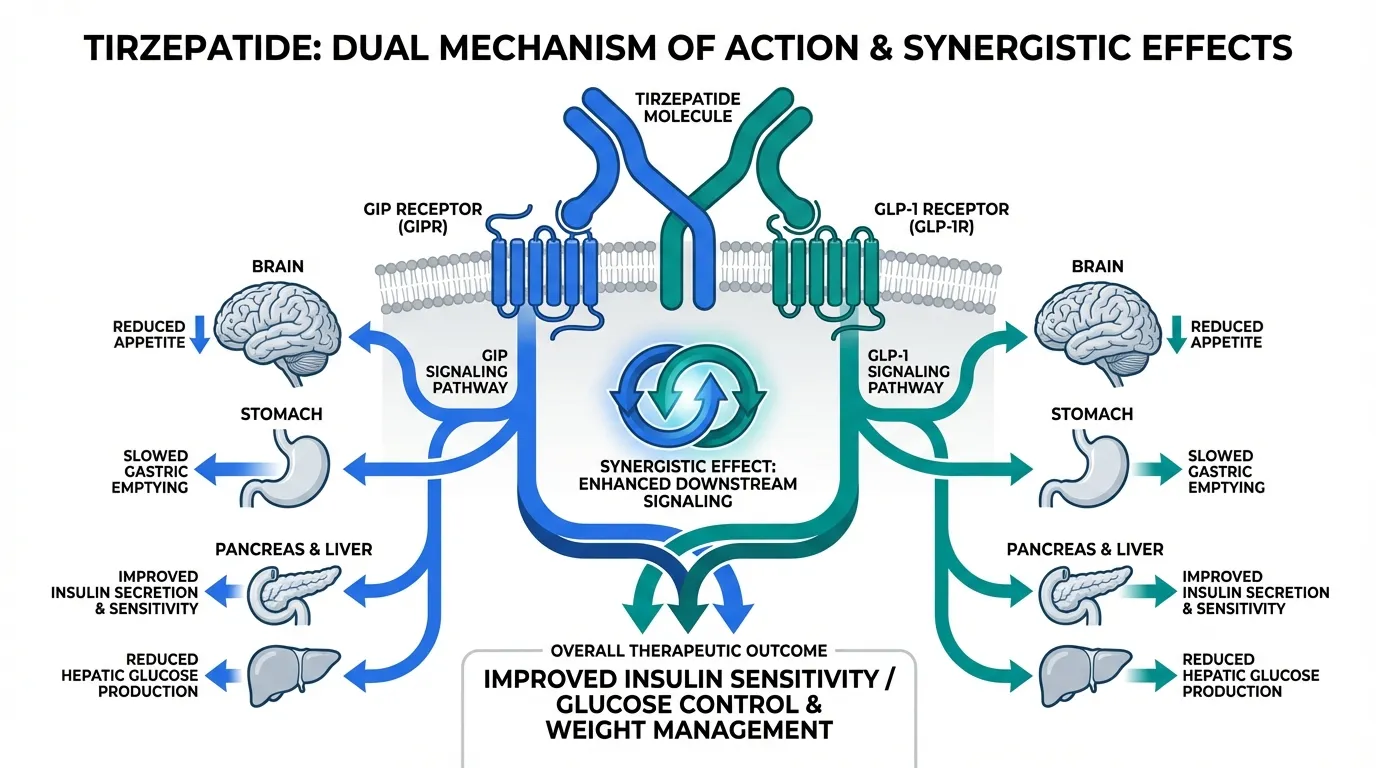
Tirzepatide activates both GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1) receptors. This dual mechanism reduces appetite through hypothalamic signaling, slows gastric emptying, and improves insulin sensitivity.
Common Side Effects#
Gastrointestinal effects are most common: nausea (20-30%), diarrhea (15-25%), and constipation (10-15%). These typically diminish with dose titration.
2. Semaglutide (Wegovy / Ozempic)#
Mechanism: GLP-1 receptor agonist FDA Status: Approved for type 2 diabetes (Ozempic) and chronic weight management (Wegovy) Evidence Level: High (Phase 3 completed, FDA-approved)
Semaglutide was the first GLP-1 receptor agonist to gain FDA approval specifically for weight management and remains one of the most extensively studied weight loss peptides.
Key Clinical Evidence#
The STEP trials established semaglutide 2.4 mg weekly as an effective weight loss treatment. In the landmark STEP 1 trial, participants lost an average of 14.9% of body weight at 68 weeks compared to 2.4% with placebo.
A 2025 systematic review of GLP-1 receptor agonists for weight loss in adults without diabetes confirmed semaglutide's efficacy across multiple populations 3.
How It Works#
Semaglutide mimics the natural hormone GLP-1, activating receptors in the brain's appetite control centers (particularly the hypothalamus and brainstem). It reduces hunger, increases satiety, and slows gastric emptying.
Common Side Effects#
Nausea (20-40%), diarrhea (15-35%), and vomiting (10-21%) are the most frequently reported adverse events across Phase 3 trials. Gradual dose escalation over 16-20 weeks helps minimize GI effects.
3. Retatrutide#
Mechanism: Triple GIP/GLP-1/glucagon receptor agonist FDA Status: Investigational (Phase 3 trials ongoing) Evidence Level: Moderate (Phase 2 completed, Phase 3 in progress)
Retatrutide represents the next frontier in receptor agonist therapy, targeting three receptors simultaneously. Its Phase 2 trial results showed the highest weight loss percentages ever observed in an obesity clinical trial.
Key Clinical Evidence#
The TRIUMPH-4 Phase 3 trial reported -28.7% body weight loss at 68 weeks with the 12 mg dose and -26.4% with the 9 mg dose, compared to -2.1% with placebo.
A 2025 systematic review and meta-analysis of retatrutide randomized controlled trials confirmed its efficacy and characterized its safety profile.
How It Works#
Retatrutide activates GIP, GLP-1, and glucagon receptors simultaneously. The addition of glucagon receptor agonism to the GIP/GLP-1 combination is hypothesized to increase energy expenditure and promote hepatic fat oxidation, contributing to the greater weight loss observed.
Common Side Effects#
The triple agonist mechanism produces higher rates of GI side effects: nausea (38-43%), diarrhea (33-35%), constipation (21-25%), and vomiting (20-21%). These rates are higher than those seen with tirzepatide or semaglutide.
Note: Retatrutide is NOT FDA-approved. It should not be described as a treatment. All efficacy data comes from clinical trials.
4. Survodutide#
Mechanism: Dual GLP-1/glucagon receptor agonist FDA Status: Investigational (Phase 3 trials ongoing) Evidence Level: Moderate (Phase 2 completed)
Survodutide (developed by Boehringer Ingelheim) takes a different approach from tirzepatide by combining GLP-1 with glucagon (rather than GIP) receptor agonism.
Key Clinical Evidence#
Phase 2 trial data showed survodutide achieving up to 18.7% body weight loss at 46 weeks. The glucagon component may provide additional metabolic benefits including improved hepatic fat metabolism. Phase 3 trials are currently enrolling.
How It Works#
By combining GLP-1 and glucagon receptor activation, survodutide reduces appetite while simultaneously increasing energy expenditure through glucagon's thermogenic effects. The glucagon component is also being investigated for its effects on liver fat (MASLD/NASH).
Common Side Effects#
Similar GI profile to other incretin-based therapies. Nausea, diarrhea, and vomiting are most common. Long-term safety data from Phase 3 trials is pending.
5. Mazdutide#
Mechanism: Dual GLP-1/glucagon receptor agonist FDA Status: Investigational (Phase 2/3 trials, primarily in China) Evidence Level: Moderate (Phase 2 completed)
Mazdutide (developed by Innovent Biologics with Eli Lilly licensing) is a dual GLP-1/glucagon receptor agonist being developed primarily for the Chinese market, with expanding global trials.
Key Clinical Evidence#
Phase 2 trials in Chinese patients with obesity showed dose-dependent weight loss up to approximately 15% at 24 weeks. The peptide is also being studied for type 2 diabetes.
How It Works#
Like survodutide, mazdutide combines GLP-1 receptor agonism (for appetite suppression and glycemic control) with glucagon receptor agonism (for increased energy expenditure and hepatic fat metabolism).
Common Side Effects#
GI adverse events are most common, consistent with the incretin-based mechanism. Dose titration strategies are being optimized in ongoing trials.
Comparison Table#
| Peptide | Mechanism | Max Weight Loss | FDA Status | Evidence Level |
|---|---|---|---|---|
| Tirzepatide | Dual GIP/GLP-1 | -20.2% (72 wk) | Approved | High |
| Semaglutide | GLP-1 | -14.9% (68 wk) | Approved | High |
| Retatrutide | Triple GIP/GLP-1/Glucagon | -28.7% (68 wk) | Phase 3 | Moderate |
| Survodutide | Dual GLP-1/Glucagon | -18.7% (46 wk) | Phase 3 | Moderate |
| Mazdutide | Dual GLP-1/Glucagon | ~15% (24 wk) | Phase 2/3 | Moderate |
What This Means for Research#
The incretin-based weight loss field is rapidly evolving. Several key trends are emerging:
-
Dual and triple agonists outperform single agonists -- tirzepatide's superiority over semaglutide, and retatrutide's even greater efficacy, suggest that multi-receptor targeting is the future of this field.
-
Glucagon receptor agonism adds metabolic benefits -- both survodutide and mazdutide leverage glucagon for energy expenditure and liver fat reduction, distinct from GIP-based approaches.
-
GI tolerability remains the primary challenge -- all five peptides share GI side effects as their most common adverse events, with more potent agents generally showing higher rates.
-
Long-term data is still emerging -- while semaglutide and tirzepatide have years of safety data, the investigational agents require longer follow-up.
Conclusion#
For researchers evaluating the peptide weight loss landscape, the evidence clearly shows a progression from single to multi-receptor agonists with increasing efficacy. Tirzepatide currently offers the best combination of proven efficacy and FDA approval, while retatrutide may set new benchmarks if Phase 3 results confirm Phase 2 findings.
All weight loss peptides require medical supervision and are prescription medications (for approved agents) or investigational compounds (for those in clinical trials). This article does not constitute medical advice.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Survodutide Overview and Research Guide
- Survodutide Dosing Protocols
- Survodutide Side Effects and Safety
- Mazdutide Overview and Research Guide
- Mazdutide Dosing Protocols
- Mazdutide Side Effects and Safety
Footnotes#
-
Tirzepatide as Compared with Semaglutide for the Treatment of Obesity (SURMOUNT-5). PMID: 40353578. 2025. ↩
-
Comparative Efficacy of Tirzepatide vs Semaglutide: Systematic Review and Meta-Analysis. PMID: 40503067. 2025. ↩
-
Efficacy and Safety of GLP-1 RAs for Weight Loss Among Adults Without Diabetes: Systematic Review. PMID: 39761578. 2025. ↩

{kind=link}
Frequently Asked Questions About 5 Most Promising Peptides for Weight Loss (Evidence-Based)
What does this article cover?
An evidence-based review of the five most promising peptides for weight loss research, including semaglutide, tirzepatide, retatrutide, survodutide, and mazdutide, with clinical trial data and mechanisms of action. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, Retatrutide, Survodutide, Mazdutide. Key context: Semaglutide (FDA-approved GLP-1 receptor agonist with extensive weight loss clinical data); Tirzepatide (Dual GIP/GLP-1 agonist showing superior weight loss in head-to-head trials); Retatrutide (Investigational triple agonist with the highest weight loss observed in clinical trials). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "5 Most Promising Peptides for Weight Loss (Evidence-Based)." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: FDA-approved GLP-1 receptor agonist with extensive weight loss clinical data. Dual GIP/GLP-1 agonist showing superior weight loss in head-to-head trials. Investigational triple agonist with the highest weight loss observed in clinical trials. These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: FDA-approved GLP-1 receptor agonist with extensive weight loss clinical data. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Peptides in Clinical Trials 2026: The Most Promising Pipeline
A research-focused overview of the most promising peptides in clinical trials as of 2026, including Retatrutide Phase 3 TRIUMPH data, Survodutide, Mazdutide, Ecnoglutide, and other emerging compounds reshaping metabolic medicine.
Weight Loss Peptides: Mechanisms, Evidence, and How They Compare
A mechanism-focused guide to weight loss peptides — how GLP-1, GIP, and glucagon pathways drive fat loss, how single, dual, and triple agonists compare, and what the clinical evidence actually shows.

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.
You Might Also Like
Related content you may find interesting