How to Switch Between GLP-1 Medications: A Practical Guide

Introduction#
As the number of available GLP-1-based medications grows, switching between agents is becoming increasingly common. Patients may switch for several reasons: inadequate weight loss, intolerable side effects, insurance or cost changes, preference for oral over injectable administration, or the desire to try a newer, more effective agent.
However, switching GLP-1 medications is not as simple as substituting one for another. Different agents have different receptor targets, different dose-response relationships, and different titration requirements. This guide covers the evidence-based principles of transitioning between GLP-1 medications, including practical dose guidance, timing considerations, and the new ATTAIN-MAINTAIN data supporting injectable-to-oral maintenance strategies.
Important: This guide is for educational purposes. All medication transitions should be supervised by a qualified healthcare provider.
Common Reasons for Switching#
Inadequate Efficacy#
Patients on semaglutide who have plateaued at 12-15% weight loss may benefit from switching to tirzepatide, which achieves approximately 21% weight loss through its additional GIP receptor activation.
Side Effect Intolerance#
GI side effects vary between agents. Some patients who cannot tolerate semaglutide may do better with tirzepatide (which has lower GI rates at equivalent efficacy in SURPASS-2) or vice versa.
Cost or Access Issues#
Insurance coverage, drug shortages, or formulary changes may necessitate switching. The growing availability of multiple agents provides more options.
Preference for Oral Administration#
Patients who have achieved their weight loss goals with injectable agents may wish to transition to oral maintenance with orforglipron (pending approval) or oral semaglutide.
Stepping Up to Multi-Receptor Agents#
As dual and triple agonists become available, patients on GLP-1-only agents may switch to multi-receptor agents for greater efficacy.
Switching from Semaglutide to Tirzepatide#
This is currently the most common switch and the best-studied transition.
Key Principles#
-
Always start tirzepatide at 2.5 mg regardless of the semaglutide dose you are coming from. Tirzepatide activates both GIP and GLP-1 receptors, making dose equivalence with a GLP-1-only agent impossible to predict.
-
Wait 7 days after your last semaglutide injection before starting tirzepatide. Both are once-weekly injections, so the transition naturally aligns with weekly dosing schedules.
-
Follow the standard titration of 2.5 mg for 4 weeks, then increase by 2.5 mg every 4 weeks (5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg maximum).
Approximate Dose Relationship#
| Semaglutide Dose | Suggested Tirzepatide Starting Approach |
|---|---|
| 0.25-0.5 mg | Start tirzepatide 2.5 mg, standard titration |
| 1.0 mg | Start tirzepatide 2.5 mg, standard titration |
| 1.7-2.4 mg | Start tirzepatide 2.5 mg, standard titration |
The starting dose is always 2.5 mg. This is not negotiable, regardless of the prior semaglutide dose. Skipping the starting dose or accelerating titration significantly increases GI side effect risk.
What to Expect During Transition#
- Weeks 1-4: GI side effects may recur even if you had adapted to semaglutide. The GIP receptor activation is new to your body.
- Weeks 4-8: Most patients see side effects diminish as they titrate to 5 mg.
- Weight plateau interruption: Many patients who had plateaued on semaglutide experience renewed weight loss with tirzepatide, particularly at 10+ mg doses.
Switching from Tirzepatide to Semaglutide#
Less common but sometimes necessary for cost, access, or tolerability reasons.
Key Principles#
- Start semaglutide at 0.25 mg for 4 weeks, then titrate per label despite prior tirzepatide exposure.
- Wait 7 days after the last tirzepatide injection.
- Expect possible weight regain during the transition period, as semaglutide generally produces less weight loss than tirzepatide at maximum doses.
Managing Expectations#
Patients switching from tirzepatide 10-15 mg to semaglutide should understand that the maximum semaglutide dose (2.4 mg for obesity) typically produces approximately 15% weight loss versus tirzepatide's approximately 21%. Some weight regain during and after transition is expected.
Injectable to Oral Transition: ATTAIN-MAINTAIN Evidence#
The ATTAIN-MAINTAIN trial provided the first Phase 3 evidence that patients can switch from injectable GLP-1 agents to oral orforglipron and maintain their previously achieved weight loss.
Trial Design#
- 376 patients who completed SURMOUNT-5 (tirzepatide vs semaglutide)
- Randomized 3:2 to orforglipron (24 or 36 mg daily) or placebo
- 52-week treatment period
Key Results#
| Transition | Orforglipron | Placebo |
|---|---|---|
| From semaglutide | -0.1 kg change | +9.4 kg regain |
| From tirzepatide | +5 kg regain | Larger regain |
Patients switching from semaglutide to orforglipron maintained their weight essentially unchanged (-0.1 kg at 24 weeks), while placebo patients regained 9.4 kg. Patients switching from tirzepatide to orforglipron experienced modest regain (5 kg) but substantially less than placebo.
Clinical Implications#
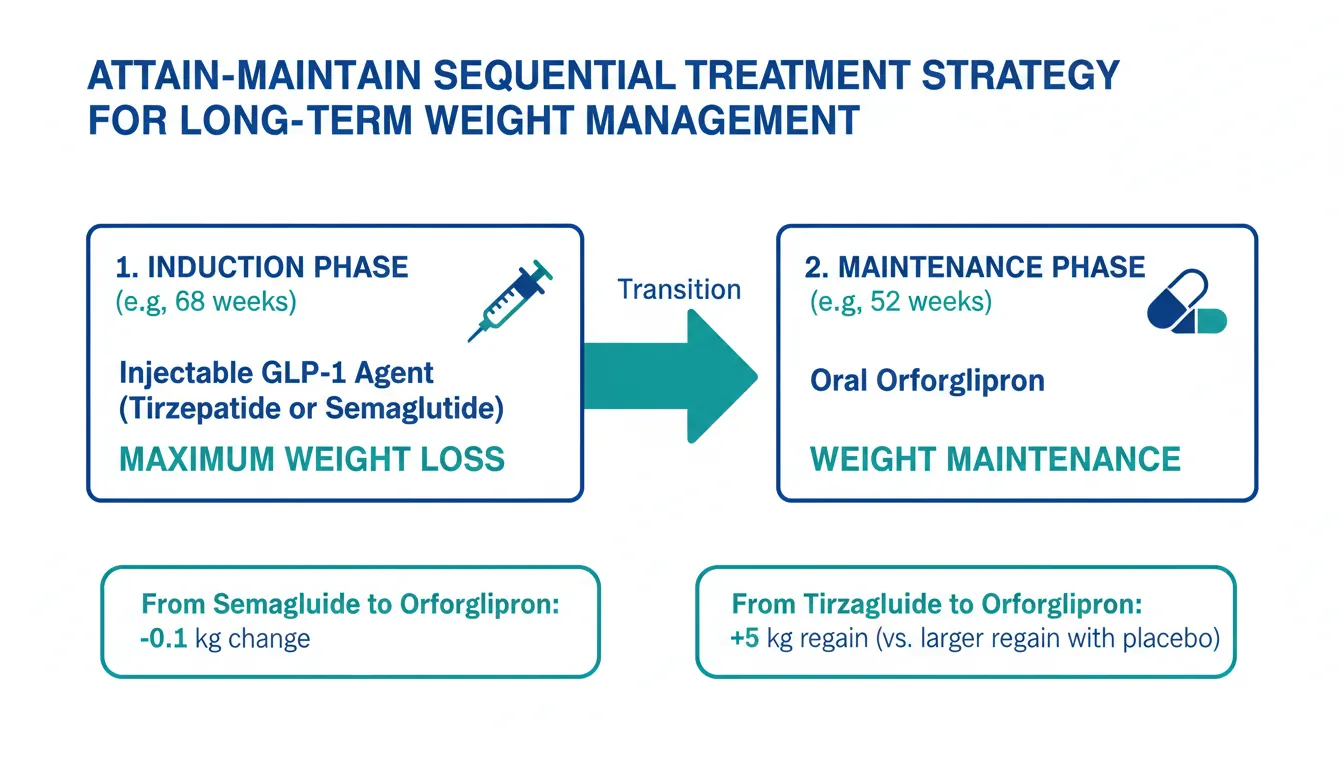
ATTAIN-MAINTAIN validates a sequential treatment strategy:
- Induction phase: Use injectable tirzepatide or semaglutide for maximum weight loss
- Maintenance phase: Switch to oral orforglipron for long-term weight maintenance without injections
This approach addresses one of the key challenges in obesity treatment: the indefinite duration of therapy and patient preference for oral medications.
Switching Between Oral Agents#
Oral Semaglutide (Rybelsus) to Orforglipron#
For patients on Rybelsus (oral semaglutide 7 or 14 mg) switching to orforglipron:
- Stop Rybelsus and start orforglipron the next day (no washout needed for daily oral agents)
- Start at the lowest orforglipron dose and titrate per protocol
- Orforglipron does not require fasting restrictions, unlike Rybelsus
ACHIEVE-3 Head-to-Head Data#
ACHIEVE-3 compared orforglipron 36 mg to oral semaglutide 14 mg head-to-head in T2D:
- HbA1c: Orforglipron -2.2% vs semaglutide -1.4%
- Weight loss: Orforglipron -9.2% vs semaglutide -5.3%
- Orforglipron was statistically superior for both endpoints
This provides direct evidence for the benefit of switching from oral semaglutide to orforglipron for patients seeking greater efficacy.
Transitioning to Multi-Receptor Agents#
As dual and triple agonists enter the market, patients on GLP-1-only agents may wish to switch to agents with additional receptor targets.
GLP-1 to GLP-1/GIP (Tirzepatide, Ribupatide)#
Starting principles are the same: begin at the lowest dose and titrate. The GIP receptor component is novel and requires independent dose optimization.
GLP-1 to GLP-1/Glucagon (Survodutide, Mazdutide, Pemvidutide)#
The addition of glucagon receptor activation requires particular caution in patients with type 2 diabetes due to glucagon's hyperglycemic effects. Close glucose monitoring during transition is essential, and the GLP-1 component's glucose-lowering effect must be sufficient to counteract glucagon's glycemic impact.
GLP-1 to Triple Agonist (Retatrutide)#
Retatrutide activates GLP-1, GIP, and glucagon receptors simultaneously. No direct switching data exist, but the general principle of starting at the lowest dose with gradual titration applies.
General Switching Principles#
Timing and Washout#
| Transition Type | Recommended Approach |
|---|---|
| Weekly injectable to weekly injectable | Wait 7 days after last dose |
| Daily oral to daily oral | Switch the next day |
| Weekly injectable to daily oral | Start oral on the day the next injection would be due |
| Daily oral to weekly injectable | Start injection 1 day after last oral dose |
Managing GI Side Effects During Switches#
- Always start at the lowest dose of the new agent, regardless of prior tolerance
- Eat smaller, more frequent meals during the first 2-4 weeks
- Stay hydrated as GI side effects can cause fluid loss
- Avoid high-fat meals which exacerbate GI symptoms
- Be patient -- most GI effects resolve within 4-8 weeks of stable dosing
Monitoring During Transitions#
- Weight: Weekly for the first 12 weeks
- Blood glucose: Daily if diabetic, especially when adding or removing glucagon-active agents
- GI symptoms: Track severity and frequency to guide dose titration
- Mental health: Monitor mood and well-being, as weight changes can affect psychological health
Conclusion#
Switching between GLP-1 medications is increasingly common and, when done correctly, can improve outcomes for patients who need different efficacy levels, better tolerability, or more convenient administration. The key principles are universal: always start the new agent at its lowest dose, allow adequate time between agents, and follow the standard titration schedule. The ATTAIN-MAINTAIN data have opened a new paradigm of injectable-to-oral sequential therapy that could transform long-term obesity management. As more agents enter the market, understanding how to transition between them will become an essential clinical skill.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Orforglipron Overview and Research Guide
- Orforglipron Dosing Protocols
- Orforglipron Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Mazdutide Overview and Research Guide
- Mazdutide Dosing Protocols
- Mazdutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About How to Switch Between GLP-1 Medications: A Practical Guide
What does this article cover?
Practical guide for transitioning between GLP-1 medications including semaglutide, tirzepatide, and orforglipron, covering dose equivalences, timing, side effect management, and ATTAIN-MAINTAIN oral maintenance data. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, Orforglipron, Retatrutide, Mazdutide. Key context: Semaglutide (Most commonly used GLP-1 agonist (Ozempic/Wegovy/Rybelsus). The medication patients most frequent...); Tirzepatide (Dual GIP/GLP-1 agonist (Mounjaro/Zepbound) that patients commonly switch to for greater weight lo...); Orforglipron (Oral GLP-1 small molecule validated by ATTAIN-MAINTAIN as a maintenance option after injectable t...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "How to Switch Between GLP-1 Medications: A Practical Guide." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Most commonly used GLP-1 agonist (Ozempic/Wegovy/Rybelsus). The medication patients most frequent.... Dual GIP/GLP-1 agonist (Mounjaro/Zepbound) that patients commonly switch to for greater weight lo.... Oral GLP-1 small molecule validated by ATTAIN-MAINTAIN as a maintenance option after injectable t.... These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: Most commonly used GLP-1 agonist (Ozempic/Wegovy/Rybelsus). The medication patients most frequently switch from, and the benchmark for dose equivalence comparisons.. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.

GLP-1 Drugs Ranked by Weight Loss: 2026 Data Comparison
Every GLP-1 and incretin drug ranked by clinical weight loss data as of 2026, from retatrutide at 28.7% to oral orforglipron at 11.2%, with comparison tables and trial details.
Peptides in Clinical Trials 2026: The Most Promising Pipeline
A research-focused overview of the most promising peptides in clinical trials as of 2026, including Retatrutide Phase 3 TRIUMPH data, Survodutide, Mazdutide, Ecnoglutide, and other emerging compounds reshaping metabolic medicine.
You Might Also Like
Related content you may find interesting