Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained

Introduction#
GLP-1 receptor agonists have transformed the treatment of obesity and type 2 diabetes over the past decade. What started with single-target injectable peptides has evolved into a diverse pipeline spanning dual agonists, triple agonists, antibody-peptide conjugates, and oral small molecules. As of early 2026, two GLP-1-based drugs are approved for obesity (semaglutide and tirzepatide), with at least eight more in Phase 2 or Phase 3 development.
This guide covers every major GLP-1 receptor agonist in clinical development, organized by mechanism, with clinical data from published trials.
Important: This article is for educational purposes only. Only semaglutide and tirzepatide are currently FDA-approved for weight management. All other agents discussed are investigational.
How GLP-1 Receptor Agonists Work#
GLP-1 (glucagon-like peptide-1) is a hormone released by the gut after eating. It stimulates insulin secretion, suppresses glucagon, slows gastric emptying, and acts on brain appetite centers to reduce hunger. GLP-1 receptor agonists mimic and amplify these effects.
The field has evolved through three generations:
- First generation -- Selective GLP-1 agonists (exenatide, liraglutide, semaglutide)
- Second generation -- Dual agonists combining GLP-1 with GIP, glucagon, or amylin activity
- Third generation -- Triple agonists, antibody conjugates, and oral small molecules
FDA-Approved GLP-1 Drugs#
Semaglutide (Wegovy / Ozempic)#
Mechanism: Selective GLP-1 receptor agonist Route: Weekly SC injection (Wegovy/Ozempic) or daily oral tablet (Rybelsus/oral Wegovy) FDA Status: Approved for T2D (2017), obesity (2021), CV risk reduction (2024), oral obesity (2025)
Semaglutide remains the most extensively studied GLP-1 agonist. Key clinical results:
- STEP 1: 14.9% weight loss at 68 weeks (SC 2.4 mg weekly)
- OASIS 1: 15.1% weight loss at 68 weeks (oral 50 mg daily)
- OASIS 4: 13.6% weight loss at 64 weeks (oral 25 mg daily, the approved dose)
- SELECT: 20% reduction in MACE events, establishing cardiovascular benefit
Semaglutide's acylated peptide structure enables albumin binding and a 7-day half-life. The oral formulation uses the SNAC absorption enhancer to achieve systemic delivery from a tablet.
Tirzepatide (Zepbound / Mounjaro)#
Mechanism: Dual GIP/GLP-1 receptor agonist Route: Weekly SC injection FDA Status: Approved for T2D (2022) and obesity (2023)
Tirzepatide demonstrated that dual incretin receptor agonism produces superior weight loss compared to GLP-1 alone:
- SURMOUNT-1: 20.9% weight loss at 72 weeks (15 mg dose)
- SURMOUNT-5: 20.2% weight loss vs 13.7% for semaglutide (head-to-head)
- SURPASS trials: Superior HbA1c reduction versus semaglutide in T2D
Tirzepatide's 4.8 kDa acylated peptide activates both GIP and GLP-1 receptors with a C20 fatty diacid enabling a 5-day half-life and weekly dosing.
Phase 3 Pipeline#
Retatrutide (Eli Lilly)#
Mechanism: Triple GIP/GLP-1/glucagon receptor agonist Route: Weekly SC injection Phase: Phase 3 (TRIUMPH program)
Retatrutide has produced the highest weight loss of any obesity drug in clinical trials:
- TRIUMPH-4: 28.7% weight loss at 68 weeks (12 mg dose) and 26.4% (9 mg dose)
- Significant knee OA pain relief alongside weight loss
- Systolic blood pressure reduction of 14.0 mmHg at 12 mg
- Seven additional Phase 3 readouts expected in 2026
The addition of glucagon receptor agonism to the GIP/GLP-1 backbone increases energy expenditure and promotes hepatic fat oxidation, contributing to the greater weight loss observed versus dual agonists.
CagriSema (Novo Nordisk)#
Mechanism: Cagrilintide (amylin analog) + semaglutide (GLP-1 agonist) co-formulation Route: Weekly SC injection (single pen) Phase: Phase 3 complete, NDA filed
CagriSema combines two complementary appetite-regulating pathways in a single weekly injection:
- REDEFINE 1: 22.7% weight loss at 68 weeks (trial product estimand) in adults without T2D
- REDEFINE 2: 15.7% weight loss at 68 weeks in adults with T2D
- CagriSema outperformed both cagrilintide alone (11.5%) and semaglutide alone (14.9%)
- NDA filed with FDA; decision expected 2026-2027
Orforglipron (Eli Lilly)#
Mechanism: Oral non-peptide small molecule GLP-1 receptor agonist Route: Daily oral tablet Phase: Phase 3 (ATTAIN program)
Orforglipron is the first non-peptide GLP-1 agonist in late-stage development, potentially transforming access:
- ATTAIN-1: 11.2% weight loss at 72 weeks (36 mg dose) vs 2.1% placebo
- 54.6% of patients achieved at least 10% weight loss at 36 mg
- No food or fasting requirements (unlike oral semaglutide)
- CYP enzyme-independent metabolism
As a small molecule (MW 883 Da), orforglipron does not require the SNAC absorption enhancer and has no food timing restrictions, potentially making it more convenient than oral semaglutide.
Survodutide (Boehringer Ingelheim)#
Mechanism: Dual GLP-1/glucagon receptor agonist Route: Weekly SC injection Phase: Phase 3 (SYNCHRONIZE program)
Survodutide targets a different receptor combination than tirzepatide, pairing GLP-1 with glucagon rather than GIP:
- Phase 2: Up to 18.7% weight loss at 46 weeks
- SYNCHRONIZE-1 and -2: Phase 3 results expected mid-to-late 2026
- Breakthrough therapy designation for MASH
- Glucagon component provides hepatic fat reduction and increased energy expenditure
Mazdutide (Innovent Biologics)#
Mechanism: Dual GLP-1/glucagon receptor agonist Route: Weekly SC injection Phase: Phase 3 (approved in China)
Mazdutide is the first dual GLP-1/glucagon agonist approved in any market:
- GLORY-1: 14.3% weight loss at 48 weeks (6 mg dose) in Chinese adults
- GLORY-2: 20.1% weight loss at 60 weeks (9 mg dose) among those without T2D
- DREAMS-3: Superiority over semaglutide in glycemic control (head-to-head)
- Approved in China for obesity; global development ongoing
VK2735 (Viking Therapeutics)#
Mechanism: Dual GLP-1/GIP receptor agonist Route: Weekly SC injection and daily oral tablet Phase: Phase 3 planned for SC; Phase 2 complete for oral
VK2735 is notable for having both injectable and oral formulations in development:
- VENTURE (SC): 14.7% weight loss at 13 weeks
- VENTURE-Oral: 12.2% weight loss at 13 weeks (oral tablet)
- Phase 3 (VANQUISH-1) initiated for SC formulation
- Oral Phase 3 expected to begin Q3 2026
Phase 2 Pipeline#
Amycretin (Novo Nordisk)#
Mechanism: Unimolecular GLP-1/amylin receptor co-agonist Route: Weekly SC injection and daily oral tablet (SNAC) Phase: Phase 2
Amycretin produced the highest weight loss of any single-molecule drug in Phase 1/2:
- SC Phase 1b/2a: 24.3% weight loss at 36 weeks (60 mg dose)
- Oral Phase 1: 13.1% weight loss at 12 weeks
- Phase 2 in T2D with 448 patients underway
- Single 68-amino acid peptide combining both activities in one molecule
CT-388 (Roche / Carmot Therapeutics)#
Mechanism: Signal-biased dual GLP-1/GIP receptor agonist Route: Weekly SC injection Phase: Phase 2
CT-388 uses a signal-biased approach that preferentially activates cAMP over beta-arrestin signaling:
- Phase 2: 22.5% weight loss at 48 weeks (24 mg dose)
- Phase 1b: 83.3% of participants experienced GI TEAEs, but only 5.9% discontinued in Phase 2
- Signal bias may improve tolerability by reducing beta-arrestin-mediated receptor desensitization
- Acquired by Roche for $5.3 billion
Aleniglipron (Structure Therapeutics)#
Mechanism: Oral small molecule GLP-1 receptor agonist Route: Daily oral tablet Phase: Phase 2 (Phase 3 planned mid-2026)
Aleniglipron is the most advanced oral small molecule GLP-1 agonist after orforglipron:
- ACCESS Phase 2b: 11.3% placebo-adjusted weight loss at 36 weeks (120 mg)
- ACCESS II: Up to 15.3% placebo-adjusted weight loss at 36 weeks (240 mg)
- Phase 3 planned for mid-2026
- No food timing restrictions
MariTide (Amgen)#
Mechanism: Antibody-peptide conjugate (GLP-1 agonist + GIPR antagonist) Route: Monthly SC injection Phase: Phase 3 (MARITIME program)
MariTide is unique in combining GLP-1 agonism with GIPR antagonism (the opposite approach to tirzepatide):
- Phase 2: Approximately 20% weight loss at 52 weeks (NEJM publication)
- Monthly dosing enabled by the 153.5 kDa antibody format and 21-day half-life
- No weight loss plateau at 52 weeks
- Phase 3 MARITIME program evaluating 72-week treatment
Summary Comparison Table#
| Drug | Mechanism | Route | Dosing | Peak Weight Loss | Phase | Company |
|---|---|---|---|---|---|---|
| Semaglutide | GLP-1 | SC / Oral | Weekly / Daily | 15.1% (68wk) | Approved | Novo Nordisk |
| Tirzepatide | GLP-1/GIP | SC | Weekly | 20.9% (72wk) | Approved | Eli Lilly |
| Retatrutide | GLP-1/GIP/GCG | SC | Weekly | 28.7% (68wk) | Phase 3 | Eli Lilly |
| CagriSema | GLP-1 + Amylin | SC | Weekly | 22.7% (68wk) | NDA filed | Novo Nordisk |
| Orforglipron | GLP-1 | Oral | Daily | 11.2% (72wk) | Phase 3 | Eli Lilly |
| Survodutide | GLP-1/GCG | SC | Weekly | 18.7% (46wk) | Phase 3 | Boehringer |
| Mazdutide | GLP-1/GCG | SC | Weekly | 20.1% (60wk) | Phase 3 / Approved (CN) | Innovent |
| VK2735 | GLP-1/GIP | SC / Oral | Weekly / Daily | 14.7% (13wk) | Phase 2/3 | Viking |
| Amycretin | GLP-1/Amylin | SC / Oral | Weekly / Daily | 24.3% (36wk) | Phase 2 | Novo Nordisk |
| CT-388 | GLP-1/GIP (biased) | SC | Weekly | 22.5% (48wk) | Phase 2 | Roche |
| Aleniglipron | GLP-1 | Oral | Daily | 15.3% (36wk) | Phase 2 | Structure |
| MariTide | GLP-1 + anti-GIPR | SC | Monthly | ~20% (52wk) | Phase 2/3 | Amgen |
Key Themes and Trends#
Multi-Receptor Targeting Increases Efficacy#
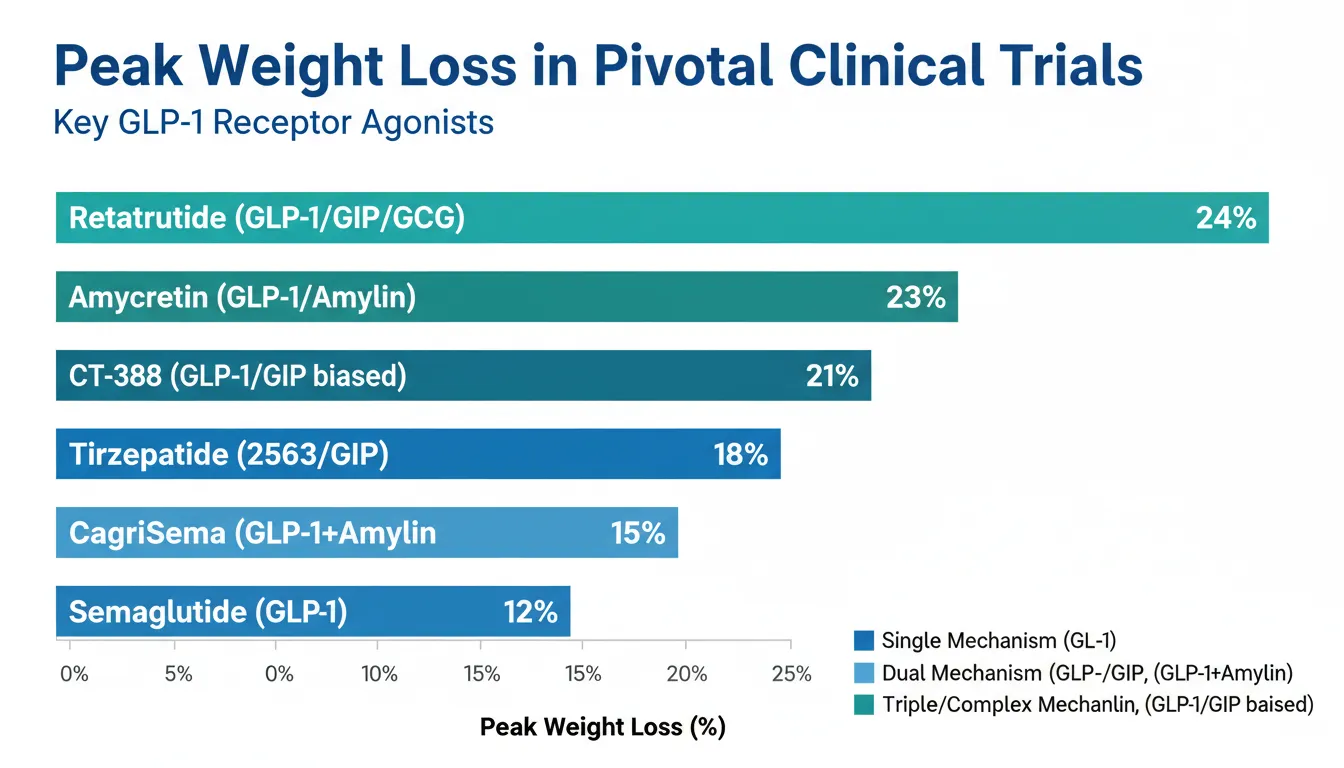
The data consistently show that targeting more receptors produces greater weight loss. Semaglutide (GLP-1 alone) achieves ~15%, tirzepatide (GLP-1 + GIP) reaches ~21%, and retatrutide (GLP-1 + GIP + glucagon) achieves up to 28.7%. However, tolerability challenges also increase with more potent agents.
The GIP Paradox#
Tirzepatide (GIPR agonist) and MariTide (GIPR antagonist) both achieve approximately 20% weight loss when combined with GLP-1 agonism. This paradox suggests that GIP pathway modulation in either direction enhances GLP-1-mediated weight loss, though through potentially different mechanisms. Head-to-head data will be needed to resolve this question.
The Oral Revolution#
At least five oral GLP-1 drugs are in development: oral semaglutide (approved), orforglipron (Phase 3), aleniglipron (Phase 2), oral VK2735 (Phase 2), and oral amycretin (Phase 1). Oral formulations could dramatically expand access by eliminating the need for injection training, cold chain storage, and needle anxiety.
Beyond Weight Loss#
The field is expanding beyond pure weight loss into metabolic health. Survodutide has breakthrough designation for MASH. Retatrutide showed significant OA pain relief. CagriSema demonstrated HbA1c improvements. Cardiovascular outcomes trials are underway for multiple agents.
Lean Mass Preservation#
A critical emerging question is body composition. Standard GLP-1 weight loss is approximately 25-40% lean mass. Pemvidutide's 21.9% lean mass ratio and retatrutide's glucagon-mediated energy expenditure both suggest that different receptor combinations may produce different body composition outcomes.
What to Watch in 2026#
- Retatrutide TRIUMPH readouts -- Seven Phase 3 results expected, potentially setting new weight loss benchmarks
- CagriSema FDA decision -- NDA filed; potential approval would give Novo Nordisk a next-generation option
- Orforglipron additional Phase 3 data -- ATTAIN program continues with T2D and CV outcomes studies
- Survodutide Phase 3 results -- SYNCHRONIZE data expected mid-to-late 2026
- Aleniglipron Phase 3 initiation -- Structure Therapeutics plans mid-2026 start
- Amycretin Phase 2 T2D data -- 448-patient study readout expected
Conclusion#
The GLP-1 receptor agonist landscape has evolved from a single-mechanism approach into a richly diverse pipeline of multi-receptor therapies. With two approved drugs achieving 15-21% weight loss and investigational agents reaching up to 28.7%, the field continues to push the boundaries of pharmacological weight management.
The next two years will be pivotal, with multiple Phase 3 readouts, potential new approvals, and the emergence of oral options that could make these therapies accessible to millions more patients worldwide.
This article is for educational and informational purposes only. It does not constitute medical advice. Consult a healthcare provider for treatment decisions.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Mazdutide Overview and Research Guide
- Mazdutide Dosing Protocols
- Mazdutide Side Effects and Safety
- Survodutide Overview and Research Guide
- Survodutide Dosing Protocols
- Survodutide Side Effects and Safety
- Orforglipron Overview and Research Guide
- Orforglipron Dosing Protocols
- Orforglipron Side Effects and Safety
- Amycretin Overview and Research Guide
- Amycretin Dosing Protocols
- Amycretin Side Effects and Safety
- CagriSema Overview and Research Guide
- CagriSema Dosing Protocols
- CagriSema Side Effects and Safety
- VK2735 Overview and Research Guide
- VK2735 Dosing Protocols
- VK2735 Side Effects and Safety
- CT-388 Overview and Research Guide
- CT-388 Dosing Protocols
- CT-388 Side Effects and Safety

{kind=link}
Frequently Asked Questions About Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
What does this article cover?
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, Retatrutide, Mazdutide, Survodutide, Orforglipron, Amycretin, CagriSema, VK2735, CT-388. Key context: Semaglutide (FDA-approved GLP-1 agonist for T2D and obesity, the benchmark comparator for all newer agents); Tirzepatide (FDA-approved dual GIP/GLP-1 agonist with superior weight loss versus semaglutide); Retatrutide (Phase 3 triple GIP/GLP-1/glucagon agonist with highest weight loss in clinical trials). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: FDA-approved GLP-1 agonist for T2D and obesity, the benchmark comparator for all newer agents. FDA-approved dual GIP/GLP-1 agonist with superior weight loss versus semaglutide. Phase 3 triple GIP/GLP-1/glucagon agonist with highest weight loss in clinical trials. These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: FDA-approved GLP-1 agonist for T2D and obesity, the benchmark comparator for all newer agents. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

GLP-1 Drugs Ranked by Weight Loss: 2026 Data Comparison
Every GLP-1 and incretin drug ranked by clinical weight loss data as of 2026, from retatrutide at 28.7% to oral orforglipron at 11.2%, with comparison tables and trial details.

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.
Peptides in Clinical Trials 2026: The Most Promising Pipeline
A research-focused overview of the most promising peptides in clinical trials as of 2026, including Retatrutide Phase 3 TRIUMPH data, Survodutide, Mazdutide, Ecnoglutide, and other emerging compounds reshaping metabolic medicine.
You Might Also Like
Related content you may find interesting