Complete Guide to Sleep Peptides: DSIP, Cortistatin, and Growth Hormone Secretagogues

Introduction#
Sleep is the single most important recovery process in human physiology. During sleep, the body executes tissue repair, consolidates memory, regulates immune function, and releases the majority of its daily growth hormone. When sleep quality declines -- whether from aging, stress, or disrupted circadian rhythms -- these recovery processes are impaired across the board.
A growing area of research interest involves peptides that may influence sleep quality, sleep architecture, or the biological processes that occur during sleep. These peptides fall into two broad categories: direct sleep-modulating peptides that act on neural circuits controlling sleep-wake transitions, and indirect sleep-enhancing peptides that amplify the recovery processes occurring during sleep, particularly growth hormone secretion.
This guide provides a comprehensive overview of all major peptides studied for sleep-related effects, covering their mechanisms, evidence quality, and important limitations. Understanding the distinction between direct and indirect sleep peptides is essential for evaluating where the science actually stands.
Important disclaimer: No peptide discussed here is FDA-approved for sleep disorders. Sleep disorders require proper medical evaluation. This guide reviews research findings, not treatment recommendations.
Two Categories of Sleep Peptides#
Before examining individual peptides, it is important to understand that "sleep peptides" is an imprecise term that encompasses two fundamentally different types of compounds:
Direct Sleep-Modulating Peptides#
These peptides act on neural circuits that control sleep architecture -- the transitions between wakefulness, light sleep, deep sleep (slow-wave sleep), and REM sleep. They directly influence how the brain generates and maintains sleep states.
- DSIP (Delta Sleep-Inducing Peptide)
- Cortistatin (CST-14)
- Pinealon (proposed melatonin pathway)
Indirect Sleep-Enhancing Peptides (GH Secretagogues)#
These peptides do not directly modulate sleep circuits. Instead, they enhance growth hormone release during the natural nocturnal GH pulse that occurs at sleep onset. Their sleep-recovery connection operates through the well-established bidirectional relationship between GH and deep sleep.
This distinction matters because the evidence standards differ. A direct sleep peptide should demonstrate measurable changes in sleep architecture (polysomnography, EEG). An indirect sleep peptide needs to demonstrate meaningful GH amplification during the sleep window, with the sleep-recovery connection inferred from established GH physiology.
DSIP (Delta Sleep-Inducing Peptide)#
Category: Direct sleep-modulating peptide Evidence Level: Mixed clinical data; primarily older research (1970s-1990s) FDA Status: Not approved; not FDA-evaluated Administration: Subcutaneous or intravenous injection
Background#
DSIP is a 9-amino-acid peptide (Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu, MW ~849 Da) first isolated in 1977 by the Schoenenberger-Monnier research group from the cerebral venous blood of rabbits during electrically induced sleep. It was named for its observed ability to induce delta-wave sleep -- the deepest stage of non-REM sleep -- when infused into the cerebral ventricles of recipient animals.
DSIP is an endogenous neuropeptide synthesized in the hypothalamus. Brain and plasma concentrations exhibit diurnal variation, with lower levels in the morning and higher levels in the afternoon, suggesting a physiological role in circadian rhythm regulation.
Mechanism of Action#
DSIP's mechanism remains what the scientific literature has called "a still unresolved riddle." Unlike most neuroactive peptides, DSIP does not appear to act through a single identified receptor. Instead, its effects are mediated through multiple pathways:
- Delta wave promotion -- increases the proportion of slow-wave sleep characterized by high-amplitude delta rhythms on EEG
- Serotonergic and GABAergic modulation -- sleep-promoting effects appear to involve modulation of serotonin and GABA neurotransmission
- NMDA receptor modulation -- may influence glutamatergic signaling involved in sleep-wake transitions
- CRF suppression -- reduces corticotropin-releasing factor, potentially lowering stress-related arousal and facilitating sleep onset
- Neuroendocrine effects -- modulates LH, GH, and ACTH release, suggesting hypothalamic-level activity
Research Evidence#
DSIP's research history spans several decades but is characterized by inconsistency:
- Schneider-Helmert (1987) -- reported acute sleep-inducing effects of IV DSIP in normal subjects, with sleep increased 59% within a 130-minute observation window
- Schneider-Helmert & Schoenenberger (1992) -- double-blind study in chronic insomniacs showed DSIP improved sleep efficiency, though sample size was small
- Animal studies -- DSIP has demonstrated sleep-promoting effects in rabbits, mice, rats, cats, and humans across multiple studies
- Stress modulation -- DSIP suppresses stress-induced rises in cortisol and ACTH, suggesting anti-stress properties that could indirectly support sleep
- Opioid withdrawal -- small studies explored DSIP as an adjunct in withdrawal management, based on its sleep-promoting and stress-modulating properties
Limitations#
DSIP's evidence base has significant weaknesses. The absence of an identified specific receptor makes its pharmacology difficult to characterize. Most clinical studies were conducted in the 1980s-1990s with small sample sizes and before modern sleep study methodology was standardized. Results have been inconsistent across studies -- some find clear sleep-promoting effects while others show no significant benefit. The peptide's very short half-life (approximately 7-8 minutes) raises questions about its pharmacological utility, as it degrades rapidly after injection. No large-scale, placebo-controlled RCTs have been conducted by modern standards.
Cortistatin (CST-14)#
Category: Direct sleep-modulating peptide Evidence Level: Preclinical only; no human clinical trials FDA Status: Not approved; not FDA-evaluated Administration: Research-grade peptide (intracerebroventricular in studies)
Background#
Cortistatin is a 14-amino-acid cyclic neuropeptide discovered in 1996 by Luis de Lecea and colleagues at The Scripps Research Institute. It was identified through a subtractive hybridization screen for genes selectively expressed in the cerebral cortex. The name reflects its cortical expression and its ability to depress (stasis) cortical neuronal activity.
Cortistatin shares 11 of 14 residues with somatostatin-14 but is encoded by a separate gene (CORT) and has distinct physiological functions. It is expressed predominantly in a subset of GABAergic interneurons in the cerebral cortex and hippocampus.
Mechanism of Action#
Cortistatin's sleep-promoting mechanism is better characterized than DSIP's:
- Cortical synchronization -- promotes EEG synchronization that characterizes slow-wave sleep, selectively enhancing deep sleep without affecting REM sleep or total sleep time
- Cholinergic antagonism -- reduces cortical arousal by antagonizing acetylcholine-mediated excitation, effectively dampening the wake-promoting cholinergic system
- Homeostatic sleep regulation -- preprocortistatin mRNA expression follows a circadian rhythm and is upregulated after sleep deprivation, suggesting cortistatin functions as an endogenous homeostatic sleep factor
- BDNF-dependent expression -- brain-derived neurotrophic factor regulates cortistatin expression in an activity-dependent manner, linking it to sleep homeostasis
Cortistatin has a unique dual receptor profile. It binds all five somatostatin receptors (sst1-5) with affinities comparable to somatostatin, but uniquely also activates the ghrelin receptor (GHSR-1a), which somatostatin does not. This dual pharmacology may contribute to its distinct sleep-promoting and anti-inflammatory effects.
Research Evidence#
All cortistatin research remains preclinical:
- de Lecea et al. (Nature, 1996) -- the original discovery paper establishing cortistatin as a selective slow-wave sleep promoter when administered intracerebroventricularly in rats
- Eur J Neurosci (2007) -- further characterization of cortistatin's role in sleep neurobiology
- Anti-inflammatory activity -- potent effects in animal models of IBD, sepsis, and arthritis, which may be relevant because systemic inflammation disrupts sleep
- Cortical excitability -- anticonvulsant activity through reduction of cortical excitability
Limitations#
Cortistatin's primary limitation is the complete absence of human clinical data. All sleep-related findings come from animal models using intracerebroventricular administration, a route not applicable in clinical practice. The peptide's short half-life in vivo limits direct clinical application without structural modification. Its significant pharmacological overlap with somatostatin also complicates therapeutic development, as somatostatin receptor activation carries metabolic and endocrine effects (GH suppression, insulin regulation) that could be problematic.
For a head-to-head comparison of these two direct sleep peptides, see Cortistatin vs DSIP.
Ipamorelin#
Category: Indirect sleep-enhancing peptide (GH secretagogue) Evidence Level: Clinical data for GH release; indirect evidence for sleep recovery FDA Status: Not FDA-approved; investigational Administration: Subcutaneous injection
Background#
Ipamorelin is a selective pentapeptide growth hormone secretagogue that acts on the ghrelin receptor (GHS-R1a). Its relevance to sleep centers on the intimate physiological relationship between growth hormone and deep sleep -- approximately 75% of daily GH secretion occurs during slow-wave sleep, and enhancing this nocturnal GH pulse may support sleep-related recovery processes.
Sleep-Recovery Connection#
Ipamorelin's connection to sleep operates through GH physiology rather than direct sleep modulation:
- Nocturnal GH amplification -- when administered before sleep, ipamorelin amplifies the natural sleep-onset GH pulse, the largest GH release event of the day
- No cortisol elevation -- unlike less selective GH secretagogues (GHRP-2, hexarelin), ipamorelin does not stimulate ACTH or cortisol release, making it appropriate for evening use without disrupting the low-cortisol environment that permits GH release during early sleep
- No prolactin elevation -- ipamorelin also does not raise prolactin, another advantage for sleep-window administration
- Recovery support -- elevated GH during sleep drives protein synthesis, tissue repair, lipolysis, and immune function -- the primary recovery processes of the sleep period
Evidence and Limitations#
Ipamorelin has clinical data supporting its GH-releasing effects but has not been specifically studied for sleep quality outcomes. The sleep-recovery rationale is based on the well-established relationship between GH and deep sleep, not on direct evidence of ipamorelin improving sleep parameters such as sleep latency, duration, or architecture. Some users report subjective improvements in sleep quality, but this has not been validated in controlled studies.
For detailed comparisons with other GH secretagogues, see Ipamorelin vs Sermorelin and Growth Hormone Secretagogues Compared.
Sermorelin#
Category: Indirect sleep-enhancing peptide (GH secretagogue) Evidence Level: Clinical data for GH stimulation; indirect sleep evidence via GHRH-sleep link FDA Status: Previously FDA-approved (discontinued commercial production) Administration: Subcutaneous injection
Background#
Sermorelin is a synthetic GHRH(1-29) analog -- the shortest fragment of growth hormone-releasing hormone that retains full biological activity at the GHRH receptor. It stimulates GH release through the same pathway as the body's own GHRH. Among sleep-related peptides, sermorelin occupies a unique position because endogenous GHRH itself has documented sleep-promoting properties.
Sleep-Recovery Connection#
Sermorelin's connection to sleep is both indirect (through GH) and partially direct (through the GHRH pathway):
- GHRH and slow-wave sleep -- endogenous GHRH has been shown to promote slow-wave sleep in human studies. GHRH administration increased time spent in deep sleep and enhanced the amplitude of nocturnal GH pulses. As a GHRH analog, sermorelin may share these properties, though this has not been specifically confirmed
- Physiological GH release -- sermorelin stimulates GH in a pulsatile pattern that mimics natural physiology, preserving the normal sleep-onset GH surge
- Pituitary reserve enhancement -- unlike GHRP-class peptides, sermorelin stimulates GH gene transcription via the cAMP/PKA/CREB pathway, increasing the pituitary's capacity to produce GH over time
- Age-related relevance -- both GH secretion and sleep quality decline simultaneously with age, and sermorelin has been studied in older adults for GH restoration
Evidence and Limitations#
The direct sleep-promoting effects of GHRH are better documented than those of sermorelin specifically. Studies by Steiger and colleagues demonstrated that GHRH administration promotes slow-wave sleep in humans, but sermorelin is a truncated 29-amino-acid analog that may not perfectly replicate all GHRH effects. Sermorelin's short half-life (~10-20 minutes) limits its duration of action, though this may actually be appropriate for pre-sleep administration where a brief pulse mimicking physiological GHRH release is the goal.
Sermorelin's former FDA approval (as Geref, 1997-2008) provides a longer safety track record than most research peptides. The drug was withdrawn due to manufacturing difficulties, not safety concerns.
Pinealon#
Category: Proposed direct sleep-modulating peptide (speculative) Evidence Level: Very limited; primarily from a single research group FDA Status: Not approved; not FDA-evaluated Administration: Oral or subcutaneous
Background#
Pinealon is a synthetic tripeptide (Glu-Asp-Arg) developed by Professor Vladimir Khavinson's research group in Russia as part of the bioregulator peptide framework. It is proposed to specifically target the pineal gland, the endocrine organ responsible for melatonin production.
Proposed Mechanism#
Pinealon's theoretical relevance to sleep operates through the melatonin pathway:
- Pineal gland regulation -- proposed to regulate gene expression in pinealocytes (pineal gland cells), supporting melatonin synthesis
- Melatonin restoration -- theoretically restores age-related declines in melatonin production by modulating pineal gland gene activity
- Circadian rhythm support -- through proposed effects on melatonin, pinealon is theoretically relevant to circadian rhythm regulation
Evidence and Limitations#
Pinealon's evidence base is extremely limited. The research comes almost exclusively from the Khavinson group, the bioregulator peptide framework has not been widely validated by independent researchers, and the mechanism by which a simple tripeptide specifically targets pineal gland gene expression has not been convincingly demonstrated. No clinical trials for sleep or melatonin-related outcomes have been published. Some in vitro data suggests neuroprotective effects on neuronal cells under oxidative stress, but this does not constitute sleep evidence. Pinealon should be considered highly speculative for sleep applications.
Other GH Secretagogues Relevant to Sleep#
Beyond ipamorelin and sermorelin, several other GH secretagogues have sleep-recovery relevance through the GH amplification pathway:
CJC-1295 (with and without DAC)#
CJC-1295 no DAC (also called Modified GRF 1-29) is a GHRH analog with improved stability compared to sermorelin. CJC-1295 DAC includes a Drug Affinity Complex that extends its half-life to approximately 6-8 days. For sleep applications, the non-DAC version may be more appropriate because it produces discrete GH pulses similar to natural physiology, whereas the DAC version creates sustained elevation that alters the normal pulsatile pattern. The relevance to sleep is the same as sermorelin -- amplification of sleep-onset GH release.
GHRP-6#
GHRP-6 is a hexapeptide ghrelin receptor agonist that potently stimulates GH release. Unlike ipamorelin, GHRP-6 also significantly stimulates appetite (through ghrelin pathway activation) and may modestly elevate cortisol at higher doses. The cortisol effect makes GHRP-6 less ideal for pre-sleep use compared to ipamorelin, since cortisol elevation during the early sleep period would antagonize the low-cortisol environment that facilitates optimal GH release and deep sleep.
For more on GH secretagogues and their comparative profiles, see Growth Hormone and Sleep: How GH Secretagogues Enhance Recovery.
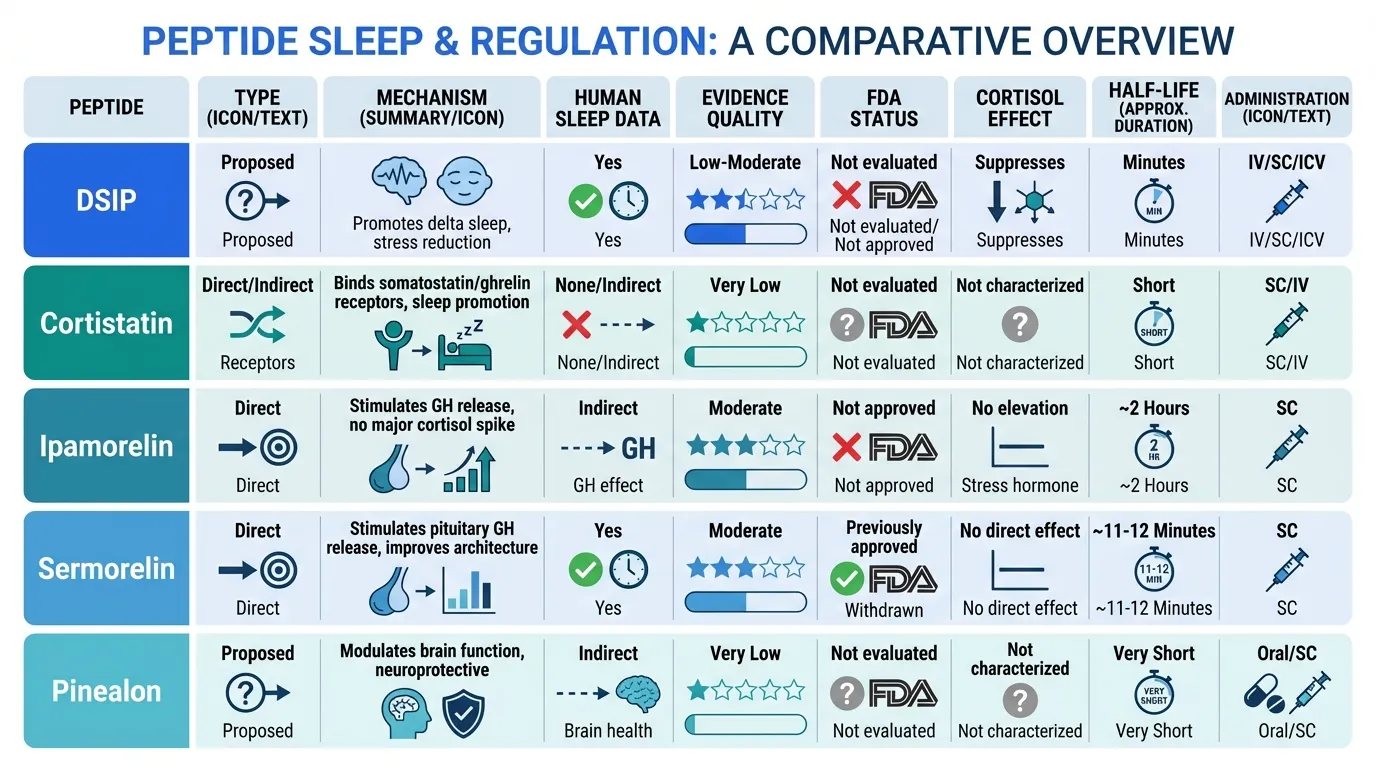
Comparative Overview#
| Feature | DSIP | Cortistatin | Ipamorelin | Sermorelin | Pinealon |
|---|---|---|---|---|---|
| Type | Direct sleep modulator | Direct sleep modulator | Indirect (GH secretagogue) | Indirect (GH secretagogue) | Proposed melatonin modulator |
| Mechanism | Multi-pathway delta wave promotion | Cortical synchronization, cholinergic antagonism | GHS-R1a agonist, nocturnal GH amplification | GHRH receptor agonist, GH pulse amplification | Proposed pineal gland gene regulation |
| Human sleep data | Yes (limited, inconsistent) | None (preclinical only) | None (GH data only) | Indirect (GHRH-sleep link) | None |
| Evidence quality | Low-moderate (old, small studies) | Low (preclinical only) | Moderate (for GH, not sleep) | Moderate (for GH, not sleep) | Very low (single research group) |
| FDA status | Not evaluated | Not evaluated | Not approved | Previously approved | Not evaluated |
| Cortisol effect | Suppresses cortisol | Not characterized | No elevation | No direct effect | Not characterized |
| Half-life | ~7-8 minutes | Short (in vivo) | ~2 hours (IV) | ~10-20 minutes | Unknown |
| Administration | SC/IV injection | ICV (research) | SC injection | SC injection | Oral/SC |
| Timing | Pre-sleep | N/A (research) | Pre-sleep | Pre-sleep | Variable |
The Science of Sleep Architecture and Peptides#
Understanding why these peptides matter for sleep requires a brief overview of sleep architecture:
Slow-Wave Sleep (SWS) and Recovery#
Slow-wave sleep (stages N3, characterized by high-amplitude delta waves on EEG) is the most restorative phase of sleep. During SWS:
- Growth hormone release -- approximately 75% of daily GH secretion occurs during the first SWS period, typically within the first 90 minutes of sleep
- Protein synthesis -- muscle and tissue repair processes peak during SWS, driven by GH/IGF-1 signaling
- Immune function -- cytokine production and immune surveillance are upregulated
- Cortisol nadir -- cortisol levels reach their lowest point during early SWS, creating a permissive hormonal environment for GH release and tissue repair
- Memory consolidation -- declarative memory consolidation is particularly linked to SWS
Both DSIP and cortistatin target SWS specifically -- DSIP by promoting delta wave activity and cortistatin by promoting EEG synchronization through cholinergic antagonism. GH secretagogues enhance the hormonal output of SWS rather than SWS itself.
The GH-Sleep Bidirectional Relationship#
The relationship between growth hormone and sleep is bidirectional:
- Sleep promotes GH -- the sleep-onset SWS period triggers the largest GH pulse of the day via GHRH release from the hypothalamus
- GH promotes sleep -- GHRH itself has been shown to promote SWS in human studies, creating a positive feedback loop
- Aging disrupts both -- age-related declines in GH secretion and SWS occur in parallel, suggesting a shared mechanism. By age 50, nocturnal GH release may decline by 75% compared to young adulthood
This bidirectional relationship provides the mechanistic rationale for using GH secretagogues to support sleep-related recovery: by amplifying the nocturnal GH pulse, these peptides may enhance the recovery processes that naturally peak during deep sleep.
Practical Considerations#
Administration Timing#
For peptides targeting the sleep window, timing is critical:
- GH secretagogues (ipamorelin, sermorelin, CJC-1295 no DAC) -- typically administered 30-60 minutes before sleep to coincide with the natural sleep-onset GH pulse
- DSIP -- administered pre-sleep, typically 30-60 minutes before bed
- Fasting state -- GH release is blunted by elevated blood glucose and insulin. For GH secretagogues, administration on an empty stomach (at least 2 hours after the last meal) may be important for optimal GH response
Cortisol Considerations#
Any peptide that significantly elevates cortisol would be counterproductive for sleep. Cortisol is the body's primary stress hormone, and its suppression during early sleep is essential for the GH pulse and for SWS quality. This is why ipamorelin's selectivity -- no cortisol or ACTH elevation -- is specifically relevant for evening use, distinguishing it from less selective GH secretagogues like GHRP-2 or hexarelin that may raise cortisol.
Complementary Approaches#
Peptides should not be considered in isolation from fundamental sleep hygiene:
- Consistent sleep schedule -- stabilizes circadian rhythm and optimizes the timing of endogenous hormone release
- Light exposure management -- morning bright light and evening darkness support natural melatonin production
- Temperature -- core body temperature decline facilitates sleep onset; a cool sleeping environment supports this process
- Stress management -- chronic stress elevates evening cortisol, suppressing the sleep-onset GH pulse and reducing SWS
Improving sleep through non-peptide interventions may enhance the efficacy of GH-related peptides, just as GH amplification may enhance the recovery benefits of improved sleep.
Evidence Hierarchy#
When evaluating sleep peptides, it is important to recognize the vast differences in evidence quality:
- Strongest evidence -- GH secretagogues' ability to increase GH release is well-established in clinical studies, and the GH-sleep relationship is one of the best-characterized phenomena in endocrinology
- Moderate evidence -- DSIP has human sleep data showing effects on delta wave activity, but studies are old, small, and inconsistent
- Mechanistic evidence only -- cortistatin has a clear and well-characterized sleep mechanism but zero human data
- Highly speculative -- pinealon's sleep claims rest on a theoretical mechanism from a single research group with no sleep-specific studies
No peptide in this guide has undergone the kind of rigorous clinical trial program that would be required for FDA approval as a sleep therapeutic.
Conclusion#
Sleep peptides represent a spectrum from direct neural sleep modulation (DSIP, cortistatin) to indirect recovery enhancement through the GH-sleep axis (ipamorelin, sermorelin). The strongest mechanistic rationale for sleep-recovery benefits exists with GH secretagogues administered before sleep, leveraging the well-established and extensively documented relationship between growth hormone and slow-wave sleep.
Among direct sleep peptides, cortistatin has the clearest mechanism but only preclinical data, while DSIP has limited human data but an unclear mechanism and inconsistent results. Pinealon remains highly speculative with insufficient evidence to evaluate.
The sleep peptide field illustrates a common challenge in peptide research: biologically plausible mechanisms do not always translate into reliable clinical effects. Until adequately powered, well-designed clinical trials are conducted for any of these compounds specifically targeting sleep outcomes, all sleep-related applications should be considered investigational.
For related content, see 5 Best Peptides for Sleep and Recovery and Cortistatin vs DSIP. For dose calculations, visit the Dosing Calculator.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- DSIP Overview and Research Guide
- DSIP Dosing Protocols
- DSIP Side Effects and Safety
- Cortistatin Overview and Research Guide
- Cortistatin Dosing Protocols
- Cortistatin Side Effects and Safety
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- Sermorelin Overview and Research Guide
- Sermorelin Dosing Protocols
- Sermorelin Side Effects and Safety
- Pinealon Overview and Research Guide
- Pinealon Dosing Protocols
- Pinealon Side Effects and Safety

{kind=link}
Frequently Asked Questions About Complete Guide to Sleep Peptides: DSIP, Cortistatin, and Growth Hormone Secretagogues
What does this article cover?
Complete guide to peptides for sleep optimization — DSIP, cortistatin, ipamorelin, sermorelin, and pinealon with mechanisms, evidence, and practical considerations. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers DSIP, Cortistatin, Ipamorelin, Sermorelin, Pinealon. Key context: DSIP (The original sleep peptide, discovered for its ability to induce delta wave sleep. Direct sleep-m...); Cortistatin (Brain-specific neuropeptide that selectively promotes slow-wave sleep through cortical synchroniz...); Ipamorelin (Selective GH secretagogue that enhances nocturnal growth hormone pulses during deep sleep without...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Complete Guide to Sleep Peptides: DSIP, Cortistatin, and Growth Hormone Secretagogues." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: The original sleep peptide, discovered for its ability to induce delta wave sleep. Direct sleep-m.... Brain-specific neuropeptide that selectively promotes slow-wave sleep through cortical synchroniz.... Selective GH secretagogue that enhances nocturnal growth hormone pulses during deep sleep without.... These takeaways are based on the research data available at the time of publication.
What is DSIP and why is it significant?
DSIP is a peptide discussed in this article because: The original sleep peptide, discovered for its ability to induce delta wave sleep. Direct sleep-modulating neuropeptide with decades of research.. For a complete profile of DSIP, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptides for Better Sleep: DSIP, Epitalon, and Growth Hormone Peptides Explained
A deep dive into peptides that influence sleep architecture and nocturnal recovery, including DSIP, epitalon, pinealon, and growth hormone secretagogues like ipamorelin and sermorelin. Mechanisms, evidence levels, and research status explained.

5 Best Peptides for Sleep and Recovery: What the Research Shows
Peptides for sleep and recovery — DSIP, ipamorelin, sermorelin, BPC-157, and pinealon — with evidence levels and practical considerations.

Peptides for Athletic Recovery: Beyond BPC-157 and TB-500
A comprehensive guide to peptides researched for athletic recovery, covering BPC-157, TB-500, GH secretagogues, MGF, GHK-Cu, and DSIP. Includes WADA anti-doping considerations, evidence levels, and recovery-focused protocol rationale.
You Might Also Like
Related content you may find interesting