Cortistatin vs DSIP: Direct Sleep Peptides Compared
Cortistatin vs DSIP comparison — two direct sleep-modulating neuropeptides with distinct mechanisms. Cortical synchronization versus delta wave promotion, evidence levels, and research applications.
Verdict at a Glance
Cortistatin has the superior mechanistic profile, with a well-defined receptor pharmacology, clear sleep-promoting mechanism through cortical synchronization, and endogenous homeostatic sleep factor properties. DSIP has more human data, but that data is old, inconsistent, and methodologically limited. Neither peptide has undergone modern clinical development for sleep. For research into sleep mechanisms, cortistatin offers a more tractable pharmacological target. For practical accessibility, DSIP is currently more available but with weaker mechanistic understanding. Both remain investigational with insufficient evidence for clinical sleep applications.
| Best for | Pick | Why |
|---|---|---|
| Understanding Sleep Mechanisms | Cortistatin | Well-defined receptor pharmacology (sst1-5 plus GHSR-1a) and clear mechanism of cortical synchronization make cortistatin a more tractable research target for sleep neurobiology |
| Human Data Availability | DSIP | DSIP has been administered to humans in multiple studies dating to the 1980s, providing at least some clinical data. Cortistatin has zero human studies for any indication |
| Current Practical Access | DSIP | DSIP can be administered subcutaneously and is available from research peptide suppliers. Cortistatin sleep studies used intracerebroventricular administration, limiting practical applicability |
| Anti-Inflammatory Co-Benefits | Cortistatin | Cortistatin has potent anti-inflammatory activity demonstrated in models of IBD, sepsis, and arthritis. This may be relevant for sleep disrupted by systemic inflammation |
| Stress-Related Sleep Disruption | DSIP | DSIP has been shown to suppress stress-induced cortisol and ACTH elevation, which may address stress-related sleep onset difficulties. Cortistatin has not been specifically studied for stress modulation |
| Category | Cortistatin | DSIP | Advantage |
|---|---|---|---|
| Mechanism of Action | Cortistatin (CST-14) is a 14-amino-acid cyclic neuropeptide that promotes slow-wave sleep through EEG synchronization and antagonism of acetylcholine-mediated cortical excitation. It has a defined dual receptor profile, binding all five somatostatin receptors (sst1-5) and uniquely activating the ghrelin receptor (GHSR-1a). Its expression follows a circadian rhythm and is upregulated after sleep deprivation, suggesting a role as a homeostatic sleep factor. | DSIP is a 9-amino-acid linear nonapeptide that promotes delta-wave (slow-wave) sleep through multiple poorly characterized pathways, including NMDA receptor modulation, serotonergic and GABAergic neurotransmission, and corticotropin-releasing factor suppression. No specific receptor has been identified for DSIP despite decades of research. Its mechanism has been described as 'a still unresolved riddle' in the literature. | Cortistatin |
| Research Evidence | All cortistatin research remains preclinical. The original 1996 Nature paper by de Lecea et al. established its sleep-promoting effects via intracerebroventricular administration in rats. Additional preclinical studies confirmed selective SWS promotion and anti-inflammatory effects. No human clinical trials for sleep or any other indication have been conducted. The evidence is mechanistically strong but clinically unvalidated. | DSIP has been studied in humans, including a 1992 double-blind study in chronic insomniacs showing improved sleep efficiency and a 1987 study showing acute sleep-inducing effects. However, clinical studies are primarily from the 1980s-1990s with small sample sizes and inconsistent results. No modern regulatory-quality trials exist. A 2024 fusion peptide study represents renewed interest. DSIP has more human data but of lower quality. | DSIP |
| Side Effect Profile | Cortistatin safety data is limited to preclinical models. As a somatostatin analog, it could theoretically suppress GH release, insulin secretion, and glucagon release through shared somatostatin receptor binding. Its short in vivo half-life may limit systemic exposure. No human adverse event data exists because no human trials have been conducted. | DSIP has limited human safety data from small clinical studies. Reported side effects include occasional headache and morning grogginess. No systematic adverse event reporting, long-term safety data, or immunogenicity testing exists. Generally described as well-tolerated in the limited studies conducted, but the evidence base is insufficient for meaningful safety characterization. | Comparable |
| Mechanism Specificity | Cortistatin has a well-defined receptor pharmacology. It binds sst1-5 and GHSR-1a with known affinities. Its sleep-promoting effect is specifically attributed to cortical synchronization via cholinergic antagonism. BDNF regulates its expression in an activity-dependent manner, providing a clear molecular link to sleep homeostasis. The mechanism is specific and reproducible in preclinical models. | DSIP's mechanism remains poorly defined after more than 45 years of research. No specific receptor has been identified. Effects appear to involve multiple pathways simultaneously, making it difficult to predict responses or optimize dosing. The multi-target mechanism may explain the inconsistency of clinical results across different studies and populations. | Cortistatin |
| Practical Applicability | Cortistatin has significant practical limitations. All sleep studies used intracerebroventricular administration, a route not applicable outside research settings. Its short in vivo half-life limits direct clinical use. Significant pharmacological overlap with somatostatin complicates therapeutic development. Structure-based analogs with improved selectivity are under investigation but remain preclinical. | DSIP can be administered subcutaneously, a practical route for clinical use. It is available from research peptide suppliers. However, its very short half-life (~7-8 minutes) raises questions about pharmacological utility. No standardized dosing protocol exists. Typical reported doses range from 100-500 mcg administered 30-60 minutes before sleep. More practically accessible than cortistatin but still limited. | DSIP |

Introduction#
Cortistatin and DSIP represent two distinct approaches to direct sleep modulation through neuropeptide signaling. Unlike growth hormone secretagogues that enhance sleep indirectly through nocturnal GH amplification, both cortistatin and DSIP act on neural circuits that control sleep architecture, making them the only two peptides in current research that can be considered direct sleep-modulating neuropeptides.
Cortistatin (CST-14) is a 14-amino-acid cyclic neuropeptide discovered in 1996, produced by GABAergic interneurons in the cerebral cortex and hippocampus. DSIP (Delta Sleep-Inducing Peptide) is a 9-amino-acid linear nonapeptide isolated in 1977 from the cerebral venous blood of rabbits during electrically induced sleep. Despite both targeting slow-wave sleep, their mechanisms, evidence quality, and practical status differ substantially.
This comparison examines how these two peptides approach sleep modulation, where the evidence stands for each, and what their respective strengths and limitations mean for sleep research.
Mechanism of Action Comparison#
Cortistatin#
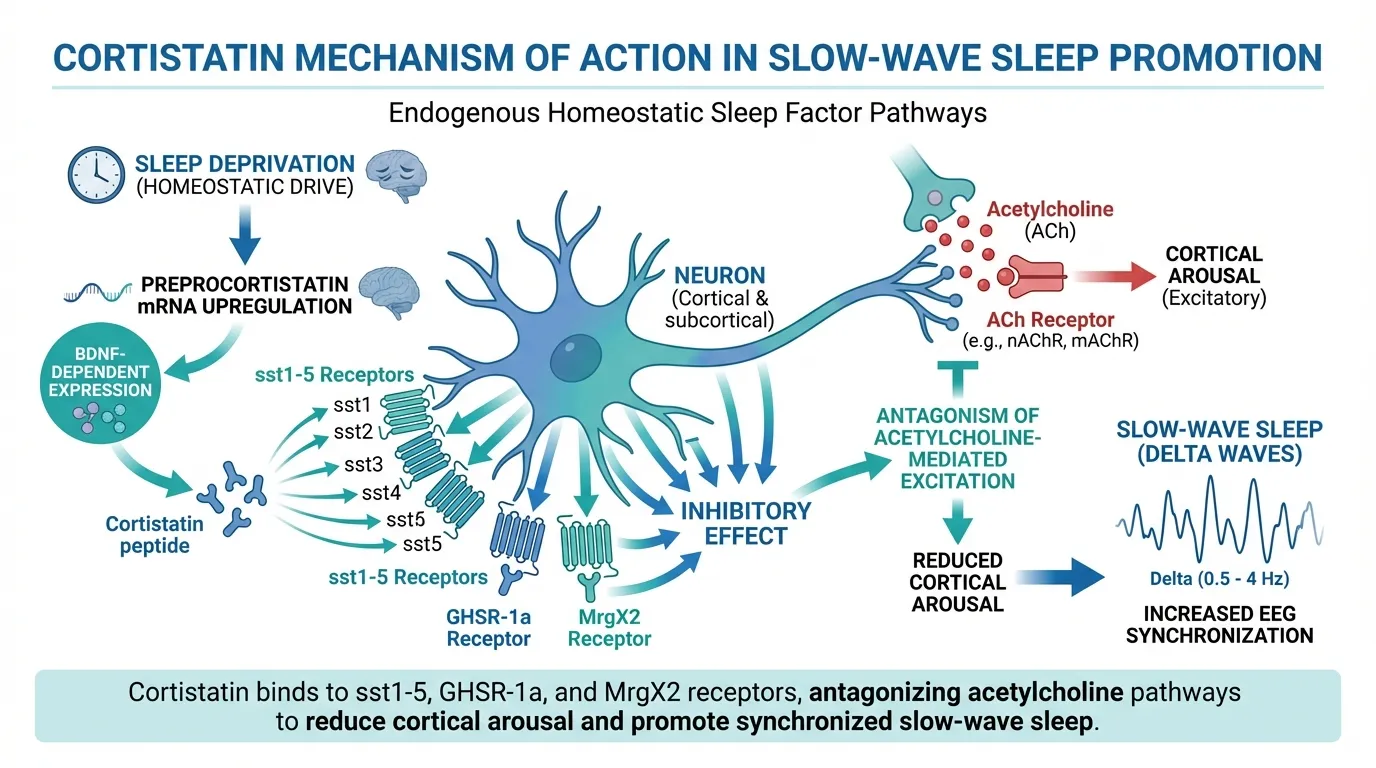
Cortistatin promotes slow-wave sleep through a well-characterized mechanism centered on cortical synchronization. When administered intracerebroventricularly in animal models, cortistatin selectively enhances deep slow-wave sleep (SWS) without affecting REM sleep or total sleep time. The mechanism involves:
- Cholinergic antagonism -- cortistatin reduces cortical arousal by antagonizing acetylcholine-mediated excitation, effectively dampening the wake-promoting cholinergic system that maintains cortical desynchronization during wakefulness
- EEG synchronization -- the transition from wakefulness to SWS is characterized by increasingly synchronized, high-amplitude delta waves on EEG. Cortistatin promotes this synchronization directly
- Homeostatic regulation -- preprocortistatin mRNA is upregulated after sleep deprivation and follows a circadian rhythm, indicating that cortistatin functions as an endogenous homeostatic sleep factor
- BDNF-dependent expression -- brain-derived neurotrophic factor regulates cortistatin expression in an activity-dependent manner, linking neuronal activity during wakefulness to subsequent sleep drive
Cortistatin's receptor pharmacology is well-defined. It binds all five somatostatin receptors (sst1-5) with affinities comparable to somatostatin, but uniquely also activates the ghrelin receptor (GHSR-1a). This dual pharmacology distinguishes it from somatostatin and may contribute to its distinct sleep-promoting and anti-inflammatory functions. Additionally, cortistatin activates the MrgX2 receptor, a Mas-related G protein-coupled receptor potentially involved in immune regulation.
DSIP#
DSIP promotes delta-wave sleep through multiple pathways, none of which are fully characterized:
- Delta wave promotion -- increases the proportion of slow-wave sleep characterized by high-amplitude delta rhythms on EEG, the phenomenon for which it was named
- Serotonergic and GABAergic modulation -- sleep effects appear to involve modulation of both serotonin and GABA neurotransmission, the two major inhibitory systems involved in sleep initiation and maintenance
- NMDA receptor modulation -- may influence glutamatergic signaling involved in sleep-wake transitions
- CRF suppression -- reduces corticotropin-releasing factor, potentially lowering stress-related arousal that prevents sleep onset
- Neuroendocrine modulation -- affects the release of LH, GH, and ACTH at the hypothalamic level
The fundamental distinction is that DSIP's mechanism remains undefined after more than 45 years of research. No specific receptor for DSIP has been identified. The peptide appears to act as a broad neuromodulator rather than through a discrete pharmacological target. This multi-pathway activity may explain both its diverse effects (sleep, stress modulation, analgesia, anticonvulsant activity) and the inconsistency of clinical results across studies.
Structural Comparison#
| Feature | Cortistatin | DSIP |
|---|---|---|
| Amino acids | 14 (cyclic, disulfide-bridged) | 9 (linear) |
| Molecular weight | ~1721 Da | ~849 Da |
| Structure | Cyclic via Cys2-Cys13 disulfide bond | Linear nonapeptide |
| Gene | CORT (chromosome 1) | Not definitively characterized |
| Expression site | Cortical/hippocampal GABAergic interneurons | Hypothalamus, widely distributed |
| Known receptors | sst1-5, GHSR-1a, MrgX2 | None identified |
| Mechanism clarity | Well-defined | Poorly defined |
| Endogenous role | Homeostatic sleep factor (confirmed) | Proposed sleep factor (debated) |
Research Evidence Comparison#
Cortistatin Research#
Cortistatin's sleep evidence is mechanistically strong but entirely preclinical:
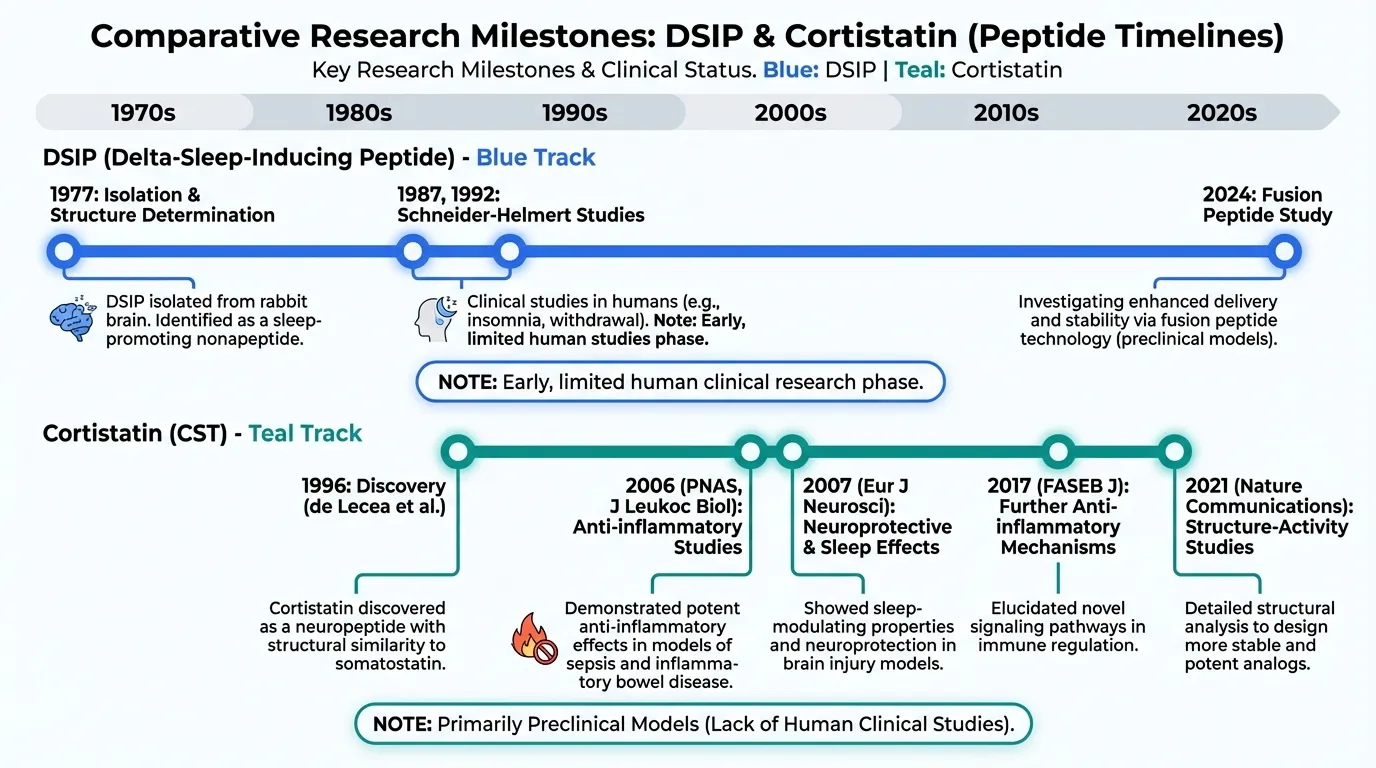
- de Lecea et al. (Nature, 1996) -- the foundational paper establishing cortistatin's discovery and its selective promotion of SWS when administered intracerebroventricularly in rats. This landmark study remains one of the strongest demonstrations of a neuropeptide's sleep-promoting activity in preclinical models
- Eur J Neurosci (2007) -- further characterization of cortistatin's sleep neurobiology, confirming the initial findings
- Anti-inflammatory studies -- cortistatin has demonstrated potent anti-inflammatory effects in multiple preclinical models (IBD: PNAS 2006, sepsis: J Leukoc Biol 2006, arthritis, atherosclerosis). While not directly sleep-related, systemic inflammation is a well-established disruptor of sleep quality
- Autoimmune myocarditis (FASEB J, 2017) -- attenuation of disease via Treg generation, further establishing anti-inflammatory potential
- Structure-activity studies (Nature Communications, 2021) -- investigation of analogs with improved selectivity, suggesting potential future clinical development
No human studies have been conducted for cortistatin in any indication, including sleep. The intracerebroventricular route used in all sleep studies is not clinically applicable.
DSIP Research#
DSIP has a larger but lower-quality evidence base that includes human data:
- Schneider-Helmert (1987) -- reported acute sleep-inducing effects of IV DSIP in normal subjects, with sleep increased 59% within a 130-minute observation window
- Schneider-Helmert & Schoenenberger (1992) -- double-blind study in chronic insomniacs showing improved sleep efficiency. This represents the best-quality clinical evidence for DSIP, though the sample size was small
- Multi-species animal data -- DSIP has demonstrated sleep-promoting effects in rabbits, mice, rats, cats, and humans
- Stress modulation -- DSIP suppresses stress-induced cortisol and ACTH rises, potentially relevant for stress-related insomnia
- Opioid and alcohol withdrawal -- small studies explored DSIP as an adjunct in withdrawal management
- 2024 fusion peptide study -- published in Frontiers in Pharmacology, research on DSIP-BBB fusion peptides in insomnia mouse models represents renewed interest in DSIP
Important limitations of DSIP's clinical evidence:
- Most studies are from the 1980s-1990s, conducted before modern polysomnography and sleep study methodology were standardized
- Sample sizes are consistently small
- Results are inconsistent across studies -- some show clear sleep effects while others do not
- No large-scale, placebo-controlled RCTs have been conducted
- Publication bias (positive results more likely published) may inflate the apparent evidence
Side Effects Comparison#
Cortistatin Side Effects#
No human safety data exists. Theoretical concerns based on pharmacology include:
- Somatostatin-like effects -- binding sst1-5 could theoretically suppress GH release, insulin secretion, and glucagon release, though cortistatin's short half-life may limit systemic exposure
- Ghrelin receptor activation -- GHSR-1a activation could theoretically influence appetite and metabolism
- Unknown systemic effects -- the absence of any human administration data means that unexpected adverse effects cannot be excluded
DSIP Side Effects#
Limited human safety data from small studies:
- Headache -- occasionally reported
- Morning grogginess -- reported at higher doses, consistent with a sleep-promoting effect persisting beyond the intended sleep period
- Generally well-tolerated -- across the limited studies conducted, no serious adverse events have been attributed to DSIP
- No systematic safety characterization -- the absence of formal adverse event reporting, long-term follow-up, and immunogenicity testing means the safety profile is incompletely characterized
Practical Applicability Comparison#
Cortistatin#
Cortistatin faces substantial practical barriers to sleep application:
- Route of administration -- all sleep studies used intracerebroventricular injection, which is only feasible in controlled research settings
- Short half-life -- rapid degradation in vivo limits duration of effect
- Somatostatin receptor cross-reactivity -- binding sst1-5 introduces potential metabolic and endocrine effects that complicate clinical development
- Research-grade only -- available only as a research peptide, not manufactured for clinical use
- Analog development -- structure-based analogs with improved selectivity and pharmacokinetics are being investigated but remain preclinical
DSIP#
DSIP is more practically accessible but still limited:
- Subcutaneous administration -- a clinically feasible route, unlike cortistatin's ICV requirement
- Available from research suppliers -- can be obtained, though quality varies between sources
- Very short half-life -- approximately 7-8 minutes, raising questions about whether meaningful sleep effects can be achieved given the rapid degradation
- No standardized protocol -- typical doses of 100-500 mcg pre-sleep are empirically derived, not established through dose-finding studies
- Stability concerns -- DSIP degrades in solution, adding practical challenges to preparation and storage
Mechanism Specificity Comparison#
This category highlights a fundamental scientific difference between the two peptides.
Cortistatin has a specific, reproducible mechanism: it promotes cortical EEG synchronization through cholinergic antagonism, selectively enhancing SWS. Its receptor binding profile is fully characterized. Its expression is regulated by circadian rhythms and BDNF in a manner consistent with homeostatic sleep regulation. This mechanistic clarity makes cortistatin a tractable pharmacological target for sleep research.
DSIP, despite decades more research time, lacks a defined mechanism. The absence of an identified receptor means that dose-response relationships, structure-activity relationships, and therapeutic optimization are all fundamentally limited. The multi-pathway activity may be intrinsic to DSIP's biology rather than a gap in knowledge -- it may genuinely function as a broad neuromodulator rather than a discrete pharmacological agent. This makes DSIP scientifically interesting but therapeutically challenging.
Key Differences Summary#
| Feature | Cortistatin | DSIP |
|---|---|---|
| Discovery | 1996 (de Lecea, Scripps) | 1977 (Schoenenberger-Monnier, Basel) |
| Structure | 14-AA cyclic peptide | 9-AA linear peptide |
| Known receptor | sst1-5, GHSR-1a, MrgX2 | None identified |
| Sleep mechanism | Cortical synchronization, cholinergic antagonism | Multi-pathway, poorly characterized |
| SWS selectivity | Selective for SWS (no REM effect) | Primarily delta wave promotion |
| Human sleep data | None | Limited (1980s-1990s studies) |
| Study route | Intracerebroventricular | Subcutaneous/intravenous |
| Half-life | Short (in vivo) | ~7-8 minutes |
| Anti-inflammatory | Potent (preclinical) | Not characterized |
| Stress modulation | Not specifically studied | Suppresses cortisol/ACTH |
| Availability | Research-grade only | Research peptide suppliers |
| Clinical development | No human trials | Small clinical studies (old) |
Conclusion#
Cortistatin and DSIP represent two fundamentally different approaches to direct sleep modulation. Cortistatin offers mechanistic clarity -- a well-defined receptor pharmacology, a specific mechanism of cortical synchronization, and validated homeostatic sleep factor properties -- but is limited to preclinical research with no human data and an impractical administration route. DSIP offers historical human data and subcutaneous administration but suffers from an undefined mechanism, inconsistent clinical results, and decades of research that have failed to identify its specific pharmacological target.
For basic sleep research, cortistatin is the more scientifically tractable compound, with a clear molecular pathway that can be studied, modulated, and potentially optimized through analog development. For practical investigation, DSIP's subcutaneous route and existing human data provide a starting point, limited as that data may be.
Neither peptide is ready for clinical sleep applications. The path forward for cortistatin likely requires development of selective analogs with improved pharmacokinetics and a clinically feasible administration route. The path forward for DSIP requires identification of its receptor and mechanism, followed by modern clinical trials with adequate sample sizes and standardized sleep outcome measures.
For a broader overview of all sleep-related peptides including GH secretagogues, see Complete Guide to Sleep Peptides. For related comparisons, see DSIP vs Oveporexton.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Understanding Sleep Mechanisms
Cortistatin
Well-defined receptor pharmacology (sst1-5 plus GHSR-1a) and clear mechanism of cortical synchronization make cortistatin a more tractable research target for sleep neurobiology
Human Data Availability
DSIP
DSIP has been administered to humans in multiple studies dating to the 1980s, providing at least some clinical data. Cortistatin has zero human studies for any indication
Current Practical Access
DSIP
DSIP can be administered subcutaneously and is available from research peptide suppliers. Cortistatin sleep studies used intracerebroventricular administration, limiting practical applicability
Anti-Inflammatory Co-Benefits
Cortistatin
Cortistatin has potent anti-inflammatory activity demonstrated in models of IBD, sepsis, and arthritis. This may be relevant for sleep disrupted by systemic inflammation
Stress-Related Sleep Disruption
DSIP
DSIP has been shown to suppress stress-induced cortisol and ACTH elevation, which may address stress-related sleep onset difficulties. Cortistatin has not been specifically studied for stress modulation
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Cortistatin vs DSIP: Direct Sleep Peptides Compared
Which is better, Cortistatin or DSIP?
Cortistatin has the superior mechanistic profile, with a well-defined receptor pharmacology, clear sleep-promoting mechanism through cortical synchronization, and endogenous homeostatic sleep factor properties. DSIP has more human data, but that data is old, inconsistent, and methodologically limited. Neither peptide has undergone modern clinical development for sleep. For research into sleep mechanisms, cortistatin offers a more tractable pharmacological target. For practical accessibility, ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Cortistatin and DSIP?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Cortistatin; Research Evidence: advantage goes to DSIP; Side Effect Profile: advantage goes to neither (tie). 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Cortistatin over DSIP?
For the scenario of "Understanding Sleep Mechanisms," research data suggests Cortistatin may be more relevant. Well-defined receptor pharmacology (sst1-5 plus GHSR-1a) and clear mechanism of cortical synchronization make cortistatin a more tractable research target for sleep neurobiology. This is based on currently available evidence and individual circumstances may differ.
How do Cortistatin and DSIP differ in their mechanisms of action?
Cortistatin: Cortistatin (CST-14) is a 14-amino-acid cyclic neuropeptide that promotes slow-wave sleep through EEG synchronization and antagonism of acetylcholine-mediated cortical excitation. It has a defined .... DSIP: DSIP is a 9-amino-acid linear nonapeptide that promotes delta-wave (slow-wave) sleep through multiple poorly characterized pathways, including NMDA receptor modulation, serotonergic and GABAergic n....
Which has fewer side effects, Cortistatin or DSIP?
In terms of side effects and tolerability, the advantage goes to neither (comparable). Cortistatin: Cortistatin safety data is limited to preclinical models. As a somatostatin analog, it could theoretically suppress GH release, insulin secretion, .... DSIP: DSIP has limited human safety data from small clinical studies. Reported side effects include occasional headache and morning grogginess. No system....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.