Growth Hormone and Sleep: How GH Secretagogues Enhance Recovery

Introduction#
The relationship between growth hormone and sleep is one of the best-characterized phenomena in endocrinology. Approximately 75% of daily growth hormone secretion occurs during slow-wave sleep (SWS), the deepest and most restorative phase of the sleep cycle. This is not coincidental -- GH release and SWS are mechanistically linked through shared hypothalamic circuitry, creating a bidirectional relationship where sleep promotes GH release and GH-releasing hormone (GHRH) promotes sleep.
This relationship provides the scientific foundation for using growth hormone secretagogues to enhance sleep-related recovery. By amplifying the natural nocturnal GH pulse, secretagogues such as ipamorelin, sermorelin, CJC-1295, and GHRP-6 may support the protein synthesis, tissue repair, immune function, and metabolic processes that peak during sleep.
This article reviews the evidence for the GH-sleep connection, examines how different GH secretagogues interact with nocturnal sleep physiology, and evaluates the strengths and limitations of the current evidence base.
The GH-Sleep Connection: Established Physiology#
Nocturnal GH Release Patterns#
Growth hormone is secreted in a pulsatile pattern throughout the day, but the largest and most physiologically significant pulse occurs during the first period of slow-wave sleep, typically within the first 60-90 minutes of sleep onset. Key characteristics of this nocturnal GH surge:
- Magnitude -- the sleep-onset GH pulse accounts for approximately 60-70% of total 24-hour GH secretion in young adults
- Timing -- GH release begins before the onset of SWS and peaks during the first SWS episode, suggesting a shared hypothalamic trigger rather than SWS causing GH release
- Hormonal permissiveness -- the nocturnal GH pulse occurs during the cortisol nadir (lowest cortisol levels of the day), which creates a permissive environment for GH release and GH-mediated anabolic processes
- GHRH dependence -- the sleep-onset GH pulse is driven by hypothalamic GHRH release, which is itself regulated by the circadian clock and sleep-wake homeostasis
GHRH as a Sleep-Promoting Factor#
A critical insight for understanding GH secretagogues and sleep is that GHRH is not merely a trigger for GH release -- it is itself a sleep-promoting substance. Human studies have demonstrated:
- GHRH promotes SWS -- intravenous GHRH administration increases the amount of slow-wave sleep in both young and elderly subjects
- GHRH antagonists reduce SWS -- blocking GHRH with a competitive antagonist reduces SWS duration, confirming GHRH's role in sleep maintenance
- Somatostatin opposes sleep -- somatostatin (the endogenous GH release inhibitor) has been shown to reduce SWS, creating a GHRH/somatostatin balance that regulates both GH release and sleep depth
- Age-related parallel decline -- the simultaneous age-related decline in both nocturnal GH secretion and SWS duration is consistent with a shared GHRH-dependent mechanism
This dual role of GHRH -- as both a GH releaser and a sleep promoter -- is particularly relevant for GHRH-class secretagogues like sermorelin and CJC-1295, which activate the same pathway.
What Happens During Sleep-Related Recovery#
The biological processes driven by nocturnal GH during SWS include:
- Protein synthesis -- GH stimulates amino acid uptake and protein synthesis in skeletal muscle, facilitating the repair of exercise-induced damage and supporting lean mass
- Tissue repair -- GH/IGF-1 signaling drives repair of tendons, ligaments, bone, and skin, with these processes peaking during sleep
- Lipolysis -- GH promotes fatty acid oxidation during the fasting sleep period, supporting body composition regulation
- Immune function -- GH supports immune cell proliferation and cytokine production, with immune surveillance most active during sleep
- Glycogen replenishment -- hepatic and muscle glycogen stores are restored during sleep, partially mediated by GH-driven metabolic shifts
When nocturnal GH release is impaired -- whether by aging, sleep disruption, elevated cortisol, or other factors -- these recovery processes are compromised proportionally.
GH Secretagogues: Two Pathways to the Same Goal#
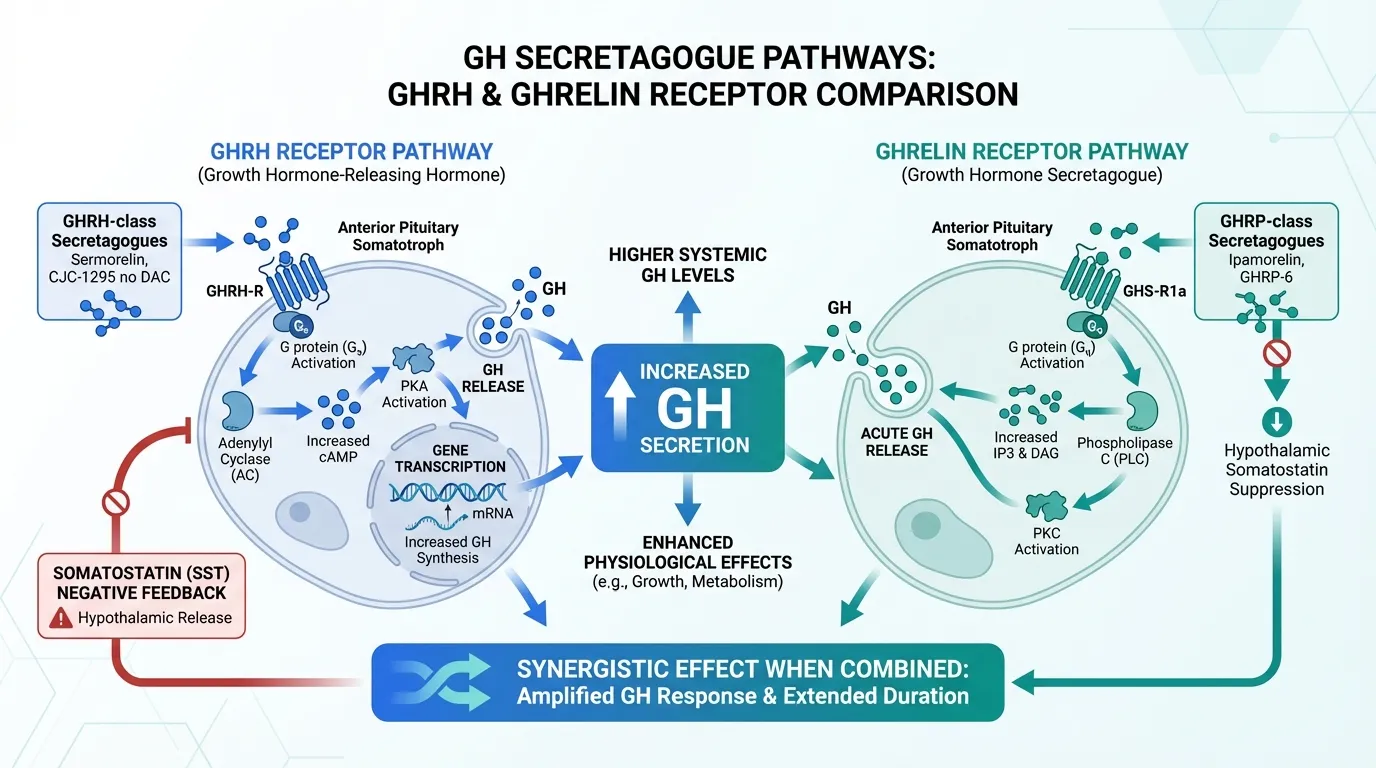
GH secretagogues relevant to sleep operate through two distinct receptor systems that converge on pituitary GH release. Understanding these pathways is essential for evaluating which secretagogue might best support nocturnal GH physiology.
GHRH Receptor Pathway (Sermorelin, CJC-1295)#
GHRH-class secretagogues bind the GHRH receptor (GHRH-R) on anterior pituitary somatotrophs, activating the cAMP/PKA signaling cascade. This pathway:
- Triggers release of stored GH granules
- Stimulates GH gene transcription (increasing pituitary GH reserve capacity)
- Maintains physiological pulsatile GH patterns
- Is regulated by somatostatin negative feedback (preventing supraphysiological GH levels)
- May share the sleep-promoting properties of endogenous GHRH
Ghrelin Receptor Pathway (Ipamorelin, GHRP-6)#
GHRP-class secretagogues bind the growth hormone secretagogue receptor 1a (GHS-R1a, the ghrelin receptor) on pituitary somatotrophs, activating the PLC/PKC pathway. This pathway:
- Triggers acute GH release through calcium mobilization
- Suppresses hypothalamic somatostatin release (reducing the brake on GH secretion)
- Does not directly stimulate GH gene transcription
- Complements the GHRH pathway, producing synergistic GH release when combined
Synergy Between Pathways#
Co-administration of a GHRH agonist and a GHRP agonist consistently produces GH release substantially greater than either agent alone. This synergy operates through complementary mechanisms: the GHRH pathway activates cAMP/PKA signaling while the GHRP pathway activates PLC/PKC signaling, and both converge on calcium mobilization for GH exocytosis. Simultaneously, GHRP-mediated somatostatin suppression removes the primary brake on GHRH-stimulated GH release.
For sleep applications, this synergy means that combining a GHRH analog (sermorelin or CJC-1295 no DAC) with a GHRP (ipamorelin) may produce a substantially larger nocturnal GH pulse than either peptide alone.
Individual GH Secretagogues and Sleep#
Ipamorelin#
Ipamorelin is a selective pentapeptide GHS-R1a agonist that offers what may be the most favorable profile for pre-sleep use among GHRP-class peptides.
Advantages for sleep applications:
- No cortisol elevation -- unlike GHRP-2 and GHRP-6, ipamorelin does not stimulate ACTH or cortisol release in preclinical studies. This is critical for sleep, as cortisol elevation during the early sleep period would antagonize the low-cortisol environment required for optimal GH release and SWS quality
- No prolactin elevation -- elevated prolactin can disrupt sleep architecture and has hormonal implications. Ipamorelin's selectivity avoids this issue
- Clean GH pulse -- produces a discrete GH pulse suitable for amplifying the natural sleep-onset surge
Limitations:
- No published human studies specifically measuring sleep outcomes (sleep latency, SWS duration, sleep architecture) with ipamorelin
- Phase II clinical trial (postoperative ileus) failed its primary endpoint; development was discontinued
- Human subcutaneous bioavailability data have not been published
- The sleep-recovery rationale is based on GH physiology inference, not direct sleep evidence
Sermorelin#
Sermorelin (GHRH(1-29)NH2) is a truncated GHRH analog that retains full biological activity at the GHRH receptor. It has the strongest theoretical rationale for sleep effects among GH secretagogues because it acts through the GHRH pathway, and GHRH itself has documented sleep-promoting properties.
Advantages for sleep applications:
- GHRH-sleep connection -- endogenous GHRH promotes SWS, and sermorelin activates the same receptor. This raises the possibility (not yet confirmed) that sermorelin may share some of GHRH's direct sleep-promoting effects
- Pituitary reserve building -- sermorelin stimulates GH gene transcription, potentially increasing the pituitary's capacity to produce GH during subsequent sleep cycles
- Physiological GH pattern -- preserves pulsatile GH release with intact somatostatin feedback
- Former FDA approval -- as Geref (1997-2008), sermorelin has a longer safety track record than most research peptides. Withdrawal was due to manufacturing issues, not safety concerns
- Clinical data in elderly -- studies by Vittone et al. showed significant IGF-1 increases with nightly GHRH(1-29) administration in older adults
Limitations:
- Short half-life (~10-20 minutes) means effects are transient, though this may be appropriate for pre-sleep use
- The sleep-promoting effects of full-length GHRH have not been specifically confirmed with the truncated 29-amino-acid sermorelin analog
- No published studies measuring sleep architecture changes with sermorelin specifically
For direct comparison, see Ipamorelin vs Sermorelin.
CJC-1295 no DAC (Modified GRF 1-29)#
CJC-1295 no DAC is a modified GHRH analog with four amino acid substitutions that improve resistance to enzymatic degradation, giving it a longer effective duration than sermorelin while still producing discrete GH pulses.
Advantages for sleep applications:
- Improved stability compared to sermorelin
- Preserves pulsatile GH release pattern compatible with natural sleep physiology
- Same GHRH receptor pathway, retaining the theoretical sleep-promoting connection
Limitations:
- Less clinical data than sermorelin
- No specific sleep outcome studies
- Not FDA-approved
CJC-1295 DAC#
CJC-1295 DAC includes a Drug Affinity Complex that binds to albumin, extending the half-life to approximately 6-8 days. This creates fundamentally different pharmacokinetics.
Considerations for sleep applications:
- Produces sustained GH elevation rather than discrete pulses, which alters the natural pulsatile pattern that characterizes physiological nocturnal GH release
- The continuous stimulation may downregulate GH responsiveness over time through receptor desensitization
- For sleep applications specifically, the non-DAC version may be more appropriate because it better mimics the discrete sleep-onset GH surge
For a detailed comparison, see CJC-1295 DAC vs CJC-1295 no DAC.
GHRP-6#
GHRP-6 is a hexapeptide ghrelin receptor agonist and one of the earliest GH secretagogues studied. It potently stimulates GH release but with a less selective profile than ipamorelin.
Considerations for sleep applications:
- Strong GH release -- GHRP-6 produces robust GH secretion, well-documented in clinical studies
- Appetite stimulation -- GHRP-6 strongly activates the ghrelin pathway, causing significant hunger. This is undesirable for pre-sleep administration when eating is counterproductive (elevated glucose/insulin blunts GH release)
- Modest cortisol elevation -- at higher doses, GHRP-6 may modestly elevate cortisol and ACTH, which could interfere with the low-cortisol sleep environment
- Prolactin elevation -- GHRP-6 can increase prolactin levels, unlike ipamorelin
For sleep-recovery applications, GHRP-6's profile is generally considered less favorable than ipamorelin's due to the cortisol, appetite, and prolactin effects. However, its potent GH-releasing ability is well-established.
Evidence Assessment#
What Is Well-Established#
The following aspects of the GH-sleep relationship are supported by strong evidence from decades of endocrinology research:
- The largest GH pulse occurs during the first SWS episode (replicated across numerous studies)
- GHRH promotes slow-wave sleep in humans (demonstrated in controlled studies)
- Somatostatin antagonism reduces SWS (confirming the GHRH/somatostatin balance model)
- GH secretagogues increase total GH output (clinical data for all agents discussed)
- Nocturnal GH drives recovery processes including protein synthesis, tissue repair, and immune function
- Both GH secretion and SWS decline with age in parallel
What Is Inferred but Not Directly Proven#
The following aspects are mechanistically logical but lack direct experimental confirmation:
- That sermorelin shares the sleep-promoting effects of full-length GHRH
- That amplifying the nocturnal GH pulse with any secretagogue translates into measurably improved recovery outcomes
- That ipamorelin's selectivity (no cortisol) produces meaningful sleep quality advantages over less selective secretagogues
- That pre-sleep GH secretagogue administration produces better recovery outcomes than other timing protocols
- That the subjective improvements in sleep quality reported by some secretagogue users reflect genuine changes in sleep architecture
What Remains Unknown#
- Whether any GH secretagogue directly improves polysomnographic sleep parameters
- The optimal dose, timing, and duration of GH secretagogue use for sleep-recovery applications
- Whether chronic use maintains, diminishes, or enhances sleep-related GH effects
- Whether the combination of GHRH + GHRP secretagogues provides better sleep-recovery outcomes than either alone
- Long-term safety data for pre-sleep secretagogue protocols in healthy adults
Age-Related Decline: Why This Matters#
The clinical relevance of the GH-sleep connection is amplified by the parallel age-related decline in both systems:
| Age Range | Approximate GH Decline | SWS Decline |
|---|---|---|
| 20-30 | Baseline | Baseline |
| 30-40 | ~15% decline | ~25-30% decline |
| 40-50 | ~30-40% decline | ~50-60% decline |
| 50-60 | ~50-60% decline | ~70-80% decline |
| 60+ | ~75%+ decline | ~80-90% decline |
By age 50, many adults have lost the majority of their youthful SWS and nocturnal GH output. These are not independent phenomena -- they reflect a shared decline in GHRH signaling and pituitary responsiveness. This parallel decline provides the strongest rationale for GH secretagogue use in aging populations: restoring the nocturnal GH pulse may support the recovery capacity that declines alongside sleep quality.
However, this rationale remains largely inferential. No large-scale clinical trial has demonstrated that GH secretagogue-mediated restoration of nocturnal GH translates into measurable improvements in sleep quality, recovery markers, or health outcomes in aging adults.
Practical Considerations for Sleep-Recovery Protocols#
Timing#
Administration timing is critical for GH secretagogues intended to support nocturnal recovery:
- 30-60 minutes before sleep is the standard timing for pre-sleep secretagogue administration
- Fasting state is preferred -- elevated blood glucose and insulin blunt GH release. A minimum of 2 hours after the last meal is generally recommended
- Consistency matters -- the circadian system responds to regular timing, and consistent pre-sleep administration may optimize the hypothalamic response
Selectivity Matters at Night#
The hormonal environment during early sleep is specifically optimized for recovery: low cortisol, low insulin, high GH, and low sympathetic tone. Any secretagogue that disrupts this environment -- by elevating cortisol (GHRP-6 at high doses), stimulating appetite (GHRP-6, leading to late-night eating and insulin elevation), or raising prolactin -- works against the goal of optimizing nocturnal recovery. This is why ipamorelin's selectivity profile is specifically valued for evening use.
GHRH + GHRP Combinations#
The combination of a GHRH-class peptide (sermorelin or CJC-1295 no DAC) with a GHRP-class peptide (ipamorelin) for pre-sleep use leverages the documented synergy between these pathways. The GHRH component may additionally carry some direct sleep-promoting activity through the GHRH receptor, while the GHRP component suppresses somatostatin to amplify the GHRH signal.
Sleep Hygiene Foundation#
GH secretagogues should complement, not replace, fundamental sleep optimization:
- Consistent sleep-wake schedule
- Cool, dark sleeping environment
- Evening light restriction (supports melatonin)
- Stress management (cortisol reduction)
- Regular physical activity (increases SWS and GH responsiveness)
Poor sleep hygiene undermines the very physiological systems that GH secretagogues aim to support. A well-optimized sleep environment maximizes the effectiveness of both endogenous and exogenous GH release.
Conclusion#
The relationship between growth hormone and sleep is well-established in endocrinology: the largest GH pulse occurs during slow-wave sleep, GHRH promotes SWS, and both systems decline together with age. GH secretagogues offer a pharmacological approach to amplifying this nocturnal GH pulse, with the goal of supporting the recovery processes that peak during deep sleep.
Among available secretagogues, ipamorelin offers the most selective profile for evening use (no cortisol, prolactin, or appetite effects), while sermorelin has the strongest theoretical rationale through its connection to the GHRH-sleep pathway. The combination of both pathways (GHRH + GHRP) produces synergistic GH release that may be greater than either alone.
The critical limitation is that no GH secretagogue has been directly studied for sleep quality outcomes in controlled trials. The sleep-recovery rationale is built on solid physiological foundations but remains inferential. Until clinical trials specifically measure sleep architecture, recovery markers, and health outcomes with pre-sleep secretagogue protocols, these applications remain evidence-informed but unproven.
For a comprehensive overview of all sleep-related peptides including direct sleep modulators, see Complete Guide to Sleep Peptides. For comparisons, see Ipamorelin vs Sermorelin and Growth Hormone Secretagogues Compared.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- Sermorelin Overview and Research Guide
- Sermorelin Dosing Protocols
- Sermorelin Side Effects and Safety
- CJC-1295 DAC Overview and Research Guide
- CJC-1295 DAC Dosing Protocols
- CJC-1295 DAC Side Effects and Safety
- CJC-1295 no DAC Overview and Research Guide
- CJC-1295 no DAC Dosing Protocols
- CJC-1295 no DAC Side Effects and Safety
- GHRP-6 Overview and Research Guide
- GHRP-6 Dosing Protocols
- GHRP-6 Side Effects and Safety

{kind=link}
Frequently Asked Questions About Growth Hormone and Sleep: How GH Secretagogues Enhance Recovery
What does this article cover?
How growth hormone secretagogues enhance sleep recovery through nocturnal GH amplification. Covers ipamorelin, sermorelin, CJC-1295, and GHRP-6. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Ipamorelin, Sermorelin, CJC-1295 DAC, CJC-1295 no DAC, GHRP-6. Key context: Ipamorelin (Selective GH secretagogue that amplifies nocturnal GH pulses without elevating cortisol or prolac...); Sermorelin (GHRH analog that stimulates physiological GH release through the same pathway as endogenous GHRH,...); CJC-1295 DAC (Long-acting GHRH analog with extended half-life that produces sustained GH elevation rather than ...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Selective GH secretagogue that amplifies nocturnal GH pulses without elevating cortisol or prolac.... GHRH analog that stimulates physiological GH release through the same pathway as endogenous GHRH,.... Long-acting GHRH analog with extended half-life that produces sustained GH elevation rather than .... These takeaways are based on the research data available at the time of publication.
What is Ipamorelin and why is it significant?
Ipamorelin is a peptide discussed in this article because: Selective GH secretagogue that amplifies nocturnal GH pulses without elevating cortisol or prolactin, making it well-suited for pre-sleep use.. For a complete profile of Ipamorelin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?
A beginner-friendly guide to growth hormone secretagogues including ipamorelin, sermorelin, CJC-1295, and more. Learn how GH peptides work, compare options, and understand which secretagogue may fit your research goals.

GHRH vs GHRP: Two Pathways to Growth Hormone Release Explained
Understand the two pathways to growth hormone release — GHRH analogs and GHRPs — how they work, differ, and combine for synergistic pulsatile GH secretion.

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
You Might Also Like
Related content you may find interesting