Peptides for Muscle Growth and Preservation: Research Guide

Introduction#
Muscle growth and preservation involve three primary pharmacological strategies: removing the biological brake on muscle growth (myostatin inhibition), stepping on the growth accelerator (IGF-1 pathway), and modulating the hormonal environment (growth hormone axis). Each strategy has distinct mechanisms, evidence levels, and clinical applications.
This guide covers 10 peptides and biologics across these three pathways, including newly profiled myostatin inhibitors (bimagrumab, trevogrumab, apitegromab) that are reshaping the field through combination strategies with GLP-1 receptor agonists.
For broader muscle recovery coverage including BPC-157 and TB-500, see Top Peptides for Muscle Recovery and Growth. For myostatin inhibitor clinical trial details, see Next-Generation Myostatin Inhibitors Compared.
Important note: No myostatin inhibitor is FDA-approved for muscle growth. HGH-191aa is approved only for GH deficiency and related conditions. This article is for educational and research purposes only.
Pathway 1: Myostatin Inhibition (Removing the Brake)#
Myostatin (GDF-8) is an endogenous protein that acts as a powerful negative regulator of muscle growth. Animals and humans with natural myostatin deficiency develop extraordinary muscle mass. The therapeutic challenge has been inhibiting myostatin safely and achieving functional improvement, not just mass increase.
GDF-8 (Myostatin) -- The Target#
GDF-8 signals through activin type II receptors (ActRIIA/B) to activate Smad2/3, which suppresses satellite cell proliferation and inhibits mTOR-mediated protein synthesis. Multiple therapeutic approaches target this pathway at different points.
Follistatin -- Natural Myostatin Inhibitor#
Evidence Level: Gene therapy trials | FDA Status: Investigational
Follistatin is the body's endogenous myostatin inhibitor, a glycoprotein that binds myostatin and prevents receptor activation. It also inhibits activins, making it a broader TGF-beta family regulator.
- AAV-mediated follistatin gene therapy has been tested in clinical trials for inclusion body myositis (IBM) and Becker muscular dystrophy
- Follistatin overexpression in animals produces 15-30% increases in muscle mass
- Challenges include short half-life as an injectable, large size (300+ amino acids), and off-target reproductive effects
ACE-031 -- Receptor Decoy (Discontinued)#
Evidence Level: Phase 2 (discontinued) | FDA Status: Development halted
ACE-031 was a soluble ActRIIB fusion protein that trapped myostatin in the bloodstream. A Phase 2 trial in Duchenne muscular dystrophy showed increased lean body mass and bone mineral density, but was halted due to vascular side effects (nosebleeds, telangiectasias) caused by inhibition of BMP9/10 -- demonstrating that broad TGF-beta trapping is too non-selective.
Bimagrumab -- Receptor Blockade#
Evidence Level: Phase 2b | FDA Status: Investigational
Bimagrumab blocks activin type II receptors with greater selectivity than ACE-031. The Phase 2b BELIEVE trial (507 participants) produced landmark body composition results:
- Bimagrumab + semaglutide: 22.1% weight loss with 92.8% from fat mass
- Semaglutide alone: 15.7% weight loss with 71.8% from fat
- Bimagrumab alone: 10.8% weight loss with +2.5% lean mass increase
Bimagrumab is the only agent shown to simultaneously increase lean mass while reducing fat mass. Administered as IV infusion every 12 weeks.
Trevogrumab -- Selective Myostatin Antibody#
Evidence Level: Phase 2 | FDA Status: Investigational
Trevogrumab (REGN-1033) directly binds mature GDF-8, offering greater selectivity than receptor-level blockade. Regeneron is evaluating it in combination with semaglutide, with and without garetosmab (anti-activin A), for muscle preservation during GLP-1-induced weight loss. Phase 2 results were announced in September 2025.
Apitegromab -- Latent Myostatin Inhibitor#
Evidence Level: Phase 3 | FDA Status: BLA submitted
Apitegromab binds pro/latent myostatin, preventing its activation. The Phase 3 SAPPHIRE trial (188 patients, SMA Types 2/3) met its primary endpoint:
- Mean HFMSE improvement of +1.8 points vs placebo (p=0.0192)
- 30.4% achieved 3+ point improvement vs 12.5% placebo
- Published in The Lancet Neurology
Apitegromab is the first myostatin-targeted therapy to demonstrate functional motor improvement in a pivotal trial, overcoming the historical mass-function disconnect. BLA was submitted but deferred for manufacturing remediation (not efficacy/safety concerns).
Myostatin Inhibitor Comparison#
| Compound | Target | Selectivity | Phase | Key Result | Route |
|---|---|---|---|---|---|
| Follistatin | Myostatin + activins | Low | Gene therapy | 15-30% muscle mass (animal) | Gene therapy |
| ACE-031 | ActRIIB ligands | Low | Discontinued | Lean mass increase; vascular AEs | SC |
| Bimagrumab | ActRII receptor | Moderate | Phase 2b | 22.1% WL + 92.8% from fat | IV q12w |
| Trevogrumab | Mature GDF-8 | High | Phase 2 | Data pending | SC |
| Apitegromab | Latent myostatin | High | Phase 3 | HFMSE +1.8 pts (p=0.019) | IV q4w |
Pathway 2: IGF-1 Signaling (Pressing the Accelerator)#
While myostatin inhibition removes the brake on muscle growth, IGF-1 pathway peptides directly stimulate the anabolic signaling cascades that drive muscle protein synthesis and satellite cell activation.
IGF-1 LR3#
Evidence Level: Well-characterized pharmacology | FDA Status: Not approved for muscle
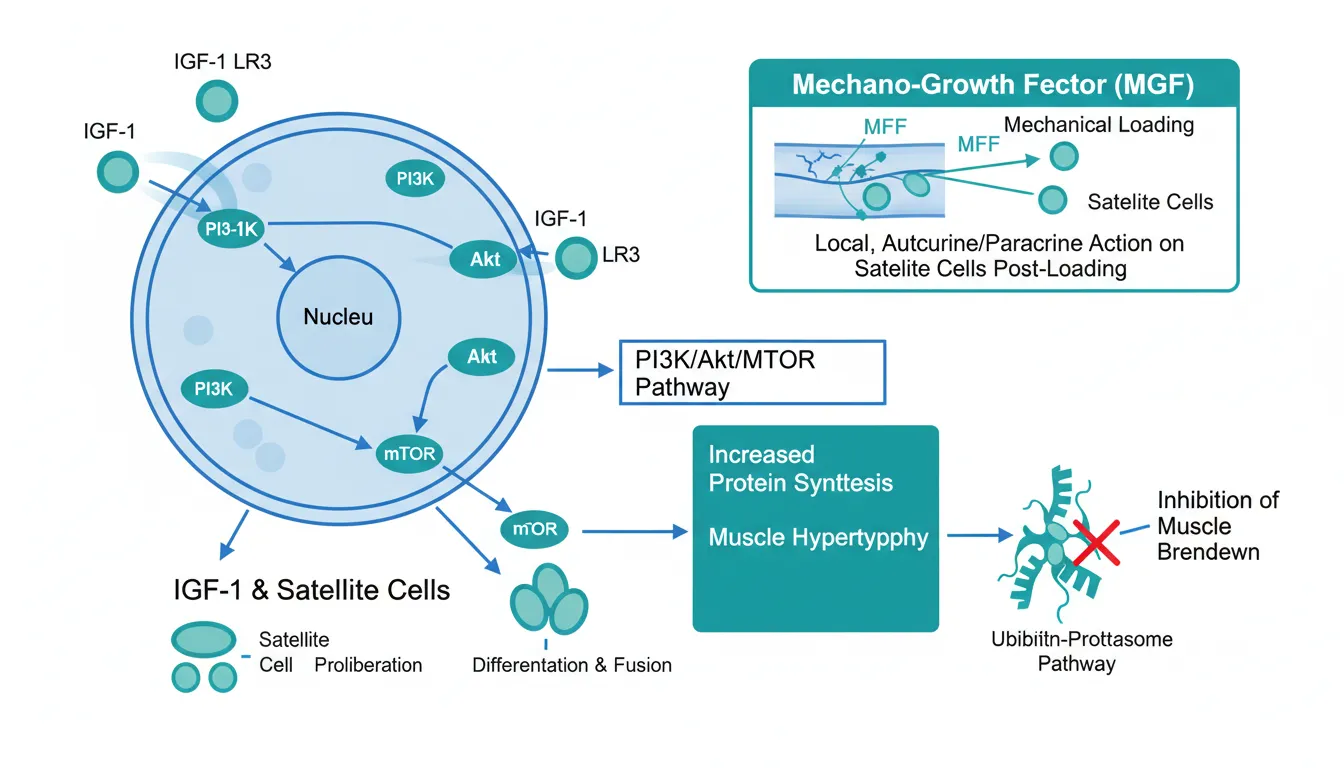
IGF-1 LR3 is a modified insulin-like growth factor 1 with a 13-amino-acid N-terminal extension and Arg3 substitution that reduces IGFBP binding, extending its effective half-life to 20-30 hours (vs hours for native IGF-1).
- Activates the PI3K/Akt/mTOR pathway, the primary signaling cascade for muscle protein synthesis
- Stimulates satellite cell proliferation and differentiation
- Inhibits muscle protein breakdown through suppression of the ubiquitin-proteasome pathway
- Has insulin-like metabolic activity (hypoglycemia risk)
Safety concern: Chronic IGF-1 elevation is epidemiologically associated with increased cancer risk. IGF-1 is a potent growth factor affecting multiple tissue types, not just muscle.
MGF (Mechano-Growth Factor)#
Evidence Level: Preclinical only | FDA Status: Not evaluated
MGF is a splice variant of the IGF-1 gene produced locally in skeletal muscle after mechanical loading (exercise). Unlike systemic IGF-1, MGF acts primarily through autocrine/paracrine signaling within the muscle tissue where it is produced.
- Upregulated following resistance exercise, particularly eccentric contractions
- Activates satellite cells for muscle repair and adaptation
- Expression declines with age, potentially contributing to sarcopenia
- Synthetic MGF has a very short half-life (minutes); PEGylated MGF (PEG-MGF) extends this but differs from the endogenous form
Limitations: No clinical trials. Injected MGF's pharmacology differs fundamentally from locally-produced endogenous MGF.
Pathway 3: Growth Hormone Axis (Hormonal Environment)#
Growth hormone (GH) and its downstream mediator IGF-1 play central roles in body composition, muscle protein synthesis, and tissue repair. Several peptides modulate this axis.
Ibutamoren (MK-677)#
Evidence Level: Phase 2 clinical trials | FDA Status: Not approved (investigational)
Ibutamoren is an oral GH secretagogue that mimics ghrelin at the GH secretagogue receptor (GHSR), stimulating pituitary GH release. It increases both GH and IGF-1 levels without suppressing endogenous GH pulsatility.
- Body composition: Clinical studies show increases in lean mass and decreases in fat mass with sustained IGF-1 elevation
- Oral dosing: Unlike injectable GH peptides, ibutamoren is taken orally (typically 25 mg/day)
- Sustained effect: Does not desensitize the GH axis with chronic use in most studies
- Sarcopenia: Studied in elderly populations for age-related muscle loss
Side effects: Increased appetite (ghrelin mimetic), water retention, potential insulin resistance with chronic use. Not approved for any indication.
HGH-191aa (Recombinant Human Growth Hormone)#
Evidence Level: FDA-approved (for GH deficiency) | FDA Status: Approved (limited indications)
HGH-191aa is recombinant human growth hormone identical to the endogenous 191-amino-acid protein. It is FDA-approved for GH deficiency in adults and children, Turner syndrome, chronic renal insufficiency, and other conditions.
- Increases lean mass and reduces fat mass through direct lipolytic and anabolic effects
- Stimulates IGF-1 production from the liver
- Well-documented effects on body composition from decades of clinical use
- Daily subcutaneous injection required
Limitations: Not approved for muscle building or anti-aging. Significant side effects with supraphysiological dosing (joint pain, carpal tunnel, insulin resistance, potential tumor growth). Cost is substantial ($500-$3,000+/month).
The GLP-1 Body Recomposition Connection#
The most commercially significant development in muscle-related peptide research is the convergence with GLP-1 receptor agonists for body recomposition. Semaglutide and tirzepatide produce substantial weight loss, but 25-40% typically comes from lean mass -- a problem that myostatin inhibitors may solve.
Current Combination Strategies#
- Bimagrumab + semaglutide (BELIEVE trial): 22.1% weight loss with 92.8% from fat
- Trevogrumab + semaglutide +/- garetosmab (Regeneron Phase 2): Targeting muscle preservation
- Pemvidutide (lean mass data): GLP-1/glucagon dual agonist with only 21.9% of weight loss from lean mass
The "quality of weight loss" -- maximizing fat loss while preserving muscle -- is emerging as a critical differentiator in the obesity therapeutics market. See Non-GLP-1 Weight Loss Peptides for broader context.
Evidence Comparison#
| Peptide | Pathway | Evidence Level | Human Data | Muscle Effect |
|---|---|---|---|---|
| Follistatin | Myostatin inhibition | Gene therapy trials | Limited | Mass increase (gene therapy) |
| GDF-8 | Target protein | Well-characterized | Observational | N/A (target) |
| ACE-031 | Receptor decoy | Phase 2 (discontinued) | Phase 2 | Lean mass increase |
| Bimagrumab | Receptor blockade | Phase 2b | BELIEVE (507 pts) | +2.5% lean mass; 93% fat loss |
| Trevogrumab | Anti-myostatin Ab | Phase 2 | Phase 2 | Data pending |
| Apitegromab | Anti-latent myostatin | Phase 3 | SAPPHIRE (188 pts) | Motor function improvement |
| IGF-1 LR3 | Anabolic signaling | Pharmacology data | Limited | Protein synthesis activation |
| MGF | Local growth factor | Preclinical | None | Satellite cell activation |
| Ibutamoren | GH secretagogue | Phase 2 | Clinical trials | Lean mass increase |
| HGH-191aa | GH replacement | FDA-approved | Extensive | Lean mass increase, fat reduction |
Key Lessons#
-
Mass is not function: The historical failure of myostatin inhibitors to translate increased muscle mass into improved function was a major setback. Apitegromab's SAPPHIRE success shows this gap can be overcome.
-
Selectivity matters: ACE-031's vascular side effects from broad TGF-beta trapping drove development toward more selective approaches (bimagrumab, trevogrumab, apitegromab).
-
Combinations win: The most compelling data comes from combining anti-myostatin approaches with GLP-1 agonists, not from standalone muscle-building therapies.
-
Body composition > weight: The shift from "how much weight" to "what kind of weight" represents a fundamental evolution in obesity and muscle therapeutics.
Conclusion#
The muscle growth and preservation landscape has evolved from single-mechanism approaches to sophisticated combination strategies. The myostatin pathway has overcome its historical challenges -- bimagrumab's body composition data with semaglutide and apitegromab's functional improvement in SMA demonstrate that this mechanism class can deliver clinically meaningful outcomes.
For researchers and clinicians, the most actionable development is the GLP-1 combination strategy, where anti-myostatin antibodies address the lean mass loss limitation of incretin-based weight loss. The IGF-1 and GH pathways remain relevant but carry more significant safety concerns with long-term use.
For related reading, see Next-Generation Myostatin Inhibitors Compared, Top Peptides for Muscle Recovery and Growth, Myostatin Inhibitors and Muscle Growth Peptides, and the GDF-8 (Myostatin) peptide profile.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Follistatin Overview and Research Guide
- Follistatin Dosing Protocols
- Follistatin Side Effects and Safety
- GDF-8 Overview and Research Guide
- GDF-8 Dosing Protocols
- GDF-8 Side Effects and Safety
- ACE-031 Overview and Research Guide
- ACE-031 Dosing Protocols
- ACE-031 Side Effects and Safety
- Bimagrumab Overview and Research Guide
- Bimagrumab Dosing Protocols
- Bimagrumab Side Effects and Safety
- Trevogrumab Overview and Research Guide
- Trevogrumab Dosing Protocols
- Trevogrumab Side Effects and Safety
- Apitegromab Overview and Research Guide
- Apitegromab Dosing Protocols
- Apitegromab Side Effects and Safety
- IGF-1 LR3 Overview and Research Guide
- IGF-1 LR3 Dosing Protocols
- IGF-1 LR3 Side Effects and Safety
- MGF Overview and Research Guide
- MGF Dosing Protocols
- MGF Side Effects and Safety
- Ibutamoren Overview and Research Guide
- Ibutamoren Dosing Protocols
- Ibutamoren Side Effects and Safety
- HGH-191aa Overview and Research Guide
- HGH-191aa Dosing Protocols
- HGH-191aa Side Effects and Safety

{kind=link}
Frequently Asked Questions About Peptides for Muscle Growth and Preservation: Research Guide
What does this article cover?
Comprehensive guide to peptides for muscle growth and preservation — myostatin inhibitors (follistatin, bimagrumab, trevogrumab, apitegromab), IGF-1 pathway (IGF-1 LR3, MGF), and growth hormone secretagogues (ibutamoren, HGH) with clinical evidence and body recomp strategies. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Follistatin, GDF-8, ACE-031, Bimagrumab, Trevogrumab, Apitegromab, IGF-1 LR3, MGF, Ibutamoren, HGH-191aa. Key context: Follistatin (Endogenous glycoprotein that inhibits myostatin and activins, studied via gene therapy for muscle...); GDF-8 (Myostatin (GDF-8) is the biological target of myostatin inhibitor strategies and the negative reg...); ACE-031 (Soluble activin receptor decoy that demonstrated muscle mass increases but was discontinued due t...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Peptides for Muscle Growth and Preservation: Research Guide." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Endogenous glycoprotein that inhibits myostatin and activins, studied via gene therapy for muscle.... Myostatin (GDF-8) is the biological target of myostatin inhibitor strategies and the negative reg.... Soluble activin receptor decoy that demonstrated muscle mass increases but was discontinued due t.... These takeaways are based on the research data available at the time of publication.
What is Follistatin and why is it significant?
Follistatin is a peptide discussed in this article because: Endogenous glycoprotein that inhibits myostatin and activins, studied via gene therapy for muscle-wasting diseases. For a complete profile of Follistatin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptides for Sarcopenia: Research on Preserving Muscle Mass with Aging
Research review of peptides targeting sarcopenia and age-related muscle loss, including myostatin inhibitors, growth factors, and GH secretagogues with clinical trial data.

Next-Generation Myostatin Inhibitors: Bimagrumab, Trevogrumab, and Apitegromab Compared
A research review comparing bimagrumab, trevogrumab, and apitegromab — three anti-myostatin antibodies in clinical development for muscle preservation, obesity, and spinal muscular atrophy.

Myostatin Inhibitors and Muscle Growth Peptides: The Research Frontier
Myostatin inhibitors and muscle growth peptides — follistatin, ACE-031, GDF-8, IGF-1 LR3, and MGF — mechanisms and clinical evidence.
You Might Also Like
Related content you may find interesting