Myostatin Inhibitors and Muscle Growth Peptides: The Research Frontier

Introduction#
Myostatin — also known as GDF-8 (growth differentiation factor 8) — is one of the most fascinating targets in muscle biology. Discovered in 1997, myostatin is an endogenous protein that acts as a powerful negative regulator of muscle growth. Animals and humans with natural myostatin deficiency develop extraordinary muscle mass, which has made myostatin inhibition one of the most actively researched approaches to treating muscle-wasting conditions.
This research review covers the current landscape of myostatin-targeted therapeutics and related muscle growth peptides, from follistatin's role as a natural myostatin inhibitor to synthetic approaches like ACE-031. We also examine IGF-1 LR3 and MGF, which promote muscle growth through complementary IGF-1-mediated pathways.
Important note: No myostatin inhibitor is FDA-approved for any indication. The clinical development history in this field includes significant setbacks that illustrate the challenges of translating biological discoveries into therapies.
Understanding Myostatin Biology#
What Is Myostatin?#
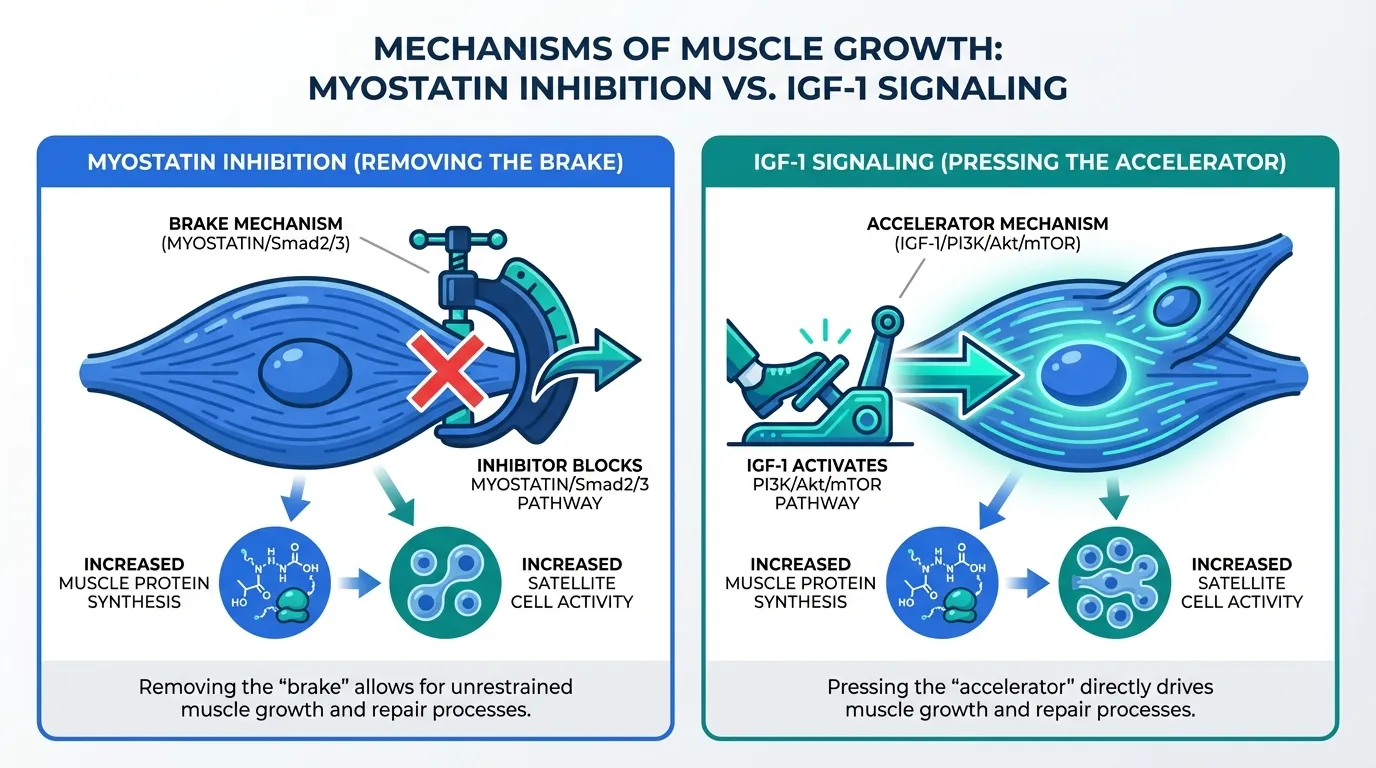
Myostatin (GDF-8) is a member of the TGF-beta superfamily of growth factors. It is primarily produced by skeletal muscle cells and acts as a brake on muscle growth through two mechanisms:
- Inhibition of satellite cell proliferation — myostatin suppresses the activation and proliferation of muscle stem cells (satellite cells) that are necessary for muscle hypertrophy and repair
- Suppression of protein synthesis — myostatin activates the Smad2/3 signaling pathway, which inhibits the mTOR pathway responsible for muscle protein synthesis
Natural Myostatin Deficiency#
The dramatic effects of myostatin loss were first demonstrated in Belgian Blue cattle — a breed with a natural myostatin gene mutation that produces extreme muscular hypertrophy (double muscling). Similar mutations have been identified in other species, including a notable case published in the New England Journal of Medicine of a human child with a homozygous myostatin mutation who displayed extraordinary muscle mass at birth.
These natural experiments prove that myostatin inhibition can produce dramatic increases in muscle mass. The challenge has been achieving this pharmacologically in a safe, controlled manner.
1. Follistatin#
Evidence Level: Gene therapy trials (limited); preclinical data extensive Primary Mechanism: Endogenous myostatin and activin inhibitor; binds and neutralizes multiple TGF-beta family members FDA Status: Not approved; gene therapy approaches in clinical trials
Follistatin is the body's own myostatin inhibitor — an endogenous glycoprotein that binds myostatin and prevents it from activating its receptor. Follistatin also inhibits activins (other TGF-beta family members involved in muscle regulation), making it a broader regulator of muscle growth than myostatin-specific approaches.
Research Findings#
Follistatin research spans preclinical and early clinical applications:
- Gene therapy — AAV-mediated follistatin gene therapy has been studied in clinical trials for inclusion body myositis (IBM) and Becker muscular dystrophy. Early results showed increased muscle volume and modest functional improvements
- Muscle hypertrophy — follistatin overexpression in animal models consistently produces significant muscle hypertrophy, with increases of 15-30% or more in muscle mass
- Dual inhibition — because follistatin inhibits both myostatin and activins, it may produce greater muscle growth effects than myostatin-only inhibition
- Reproductive effects — follistatin also plays roles in reproductive biology (it was originally discovered as a follicle-stimulating hormone inhibitor), which complicates its therapeutic development
Important Considerations#
Exogenous follistatin as an injectable peptide faces significant challenges: it is a large glycoprotein (over 300 amino acids) with a short half-life and limited bioavailability. The most promising follistatin approaches use gene therapy rather than direct protein administration. Follistatin's broad inhibition of TGF-beta family members raises concerns about off-target effects, particularly in reproductive tissues and cardiac muscle.
2. ACE-031#
Evidence Level: Phase 2 clinical trial (discontinued due to safety signals) Primary Mechanism: Soluble activin receptor type IIB (ActRIIB) decoy that traps myostatin and related ligands FDA Status: Clinical development discontinued
ACE-031 was a recombinant fusion protein designed to act as a "myostatin trap" — a soluble version of the activin receptor IIB (ActRIIB) that binds myostatin (and other TGF-beta ligands) in the bloodstream before they can reach their cellular receptors.
Research Findings#
ACE-031 represents the most significant clinical development effort in myostatin inhibition:
- Duchenne muscular dystrophy (DMD) — a Phase 2 trial in boys with DMD demonstrated increases in lean body mass and bone mineral density, suggesting biological activity of the myostatin-trapping mechanism
- Safety concerns — the trial was halted due to minor nosebleeds, gum bleeding, and small dilated blood vessels (telangiectasias) observed in some participants. These vascular side effects were attributed to ACE-031's inhibition of BMP9 and BMP10 — TGF-beta family members involved in vascular homeostasis — not to myostatin inhibition itself
- Lesson learned — ACE-031 demonstrated that non-selective TGF-beta family inhibition produces unacceptable vascular side effects, driving the field toward more selective approaches
Important Considerations#
ACE-031's clinical program was discontinued and it is not in active development. However, its legacy is significant: it proved that myostatin trapping can increase muscle mass in humans but also showed that the TGF-beta superfamily is too interconnected for broad-spectrum inhibition to be safe. The successor approach — more selective myostatin or activin inhibitors — is being pursued by multiple companies.
3. GDF-8 (Myostatin) — The Target#
Evidence Level: Well-characterized biology; multiple therapeutic approaches targeting GDF-8 Primary Mechanism: Negative regulator of muscle growth through ActRIIB/Smad2/3 signaling FDA Status: Endogenous protein; targeted by investigational therapies
GDF-8 (myostatin) is not a therapeutic compound but rather the biological target that the other peptides in this guide aim to inhibit. Understanding myostatin biology is essential context for evaluating myostatin inhibitor strategies.
Current Therapeutic Approaches Targeting Myostatin#
Multiple approaches to myostatin inhibition have been or are being developed:
- Anti-myostatin antibodies — monoclonal antibodies that directly bind and neutralize circulating myostatin (e.g., domagrozumab, stamulumab). Several have shown modest increases in lean mass but disappointing functional outcomes in clinical trials
- Activin receptor traps — like ACE-031, these capture myostatin before receptor binding (newer versions with improved selectivity are in development)
- Gene therapy — follistatin gene therapy and direct myostatin gene editing approaches
- Antisense oligonucleotides — targeting myostatin mRNA to reduce production
The Efficacy Gap#
A critical finding across myostatin inhibitor trials has been the disconnect between increases in muscle mass and improvements in muscle function. Multiple compounds have demonstrated measurable increases in lean body mass while failing to produce proportional improvements in strength, mobility, or functional outcomes. This suggests that myostatin inhibition-induced muscle may differ qualitatively from exercise-induced muscle.
4. IGF-1 LR3#
Evidence Level: Well-characterized pharmacology; limited clinical data for muscle-specific applications Primary Mechanism: Long-acting IGF-1 analog; promotes muscle protein synthesis through IGF-1 receptor activation FDA Status: Not approved for muscle indications; mecasermin (recombinant IGF-1) approved for IGF-1 deficiency
IGF-1 LR3 is a modified form of insulin-like growth factor 1 (IGF-1) with an extended half-life due to reduced binding to IGF-binding proteins (IGFBPs). It approaches muscle growth through a complementary pathway to myostatin inhibition — rather than removing the brake on muscle growth, IGF-1 LR3 steps on the accelerator.
Research Findings#
IGF-1 LR3's muscle growth mechanisms are well-characterized:
- Protein synthesis — IGF-1 activates the PI3K/Akt/mTOR pathway, the primary intracellular signaling cascade for muscle protein synthesis
- Satellite cell activation — IGF-1 stimulates the proliferation and differentiation of muscle satellite cells, supporting muscle repair and hypertrophy
- Anti-catabolic effects — IGF-1 signaling inhibits muscle protein breakdown through suppression of the ubiquitin-proteasome pathway and autophagy
- Extended half-life — the LR3 modification (amino acid substitution at position 3 plus a 13-amino-acid N-terminal extension) reduces IGFBP binding, increasing free IGF-1 levels and extending the effective half-life from hours to approximately 20-30 hours
Important Considerations#
IGF-1 LR3 carries significant safety concerns. Chronic IGF-1 elevation is epidemiologically associated with increased cancer risk — IGF-1 is a potent growth factor that promotes cell proliferation in many tissue types, not just muscle. Hypoglycemia is a common side effect due to IGF-1's insulin-like metabolic activity. IGF-1 LR3 is not approved for muscle enhancement, and its use carries meaningful health risks. For its broader context in muscle recovery, see Top Peptides for Muscle Recovery and Growth.
5. MGF (Mechano-Growth Factor)#
Evidence Level: Preclinical; primarily in vitro and animal data Primary Mechanism: Splice variant of IGF-1 produced locally in muscle after mechanical loading; promotes satellite cell activation FDA Status: Not approved; not FDA-evaluated
MGF (mechano-growth factor) is a splice variant of the IGF-1 gene that is produced locally within skeletal muscle tissue in response to mechanical loading (exercise) or damage. Unlike systemic IGF-1, MGF acts primarily through autocrine/paracrine signaling within the muscle tissue where it is produced.
Research Findings#
MGF's role in muscle biology centers on local repair signaling:
- Exercise-induced expression — MGF is upregulated in muscle tissue following resistance exercise, particularly after eccentric (muscle-lengthening) contractions
- Satellite cell activation — MGF activates muscle satellite cells, promoting their proliferation and initiating the repair process that leads to muscle adaptation
- Age-related decline — MGF expression in response to exercise declines with age, potentially contributing to the reduced adaptive capacity of aging muscle (sarcopenia)
- Local vs. systemic action — unlike circulating IGF-1, MGF acts primarily within the muscle where it is produced, suggesting a more targeted growth signal
Important Considerations#
Synthetic MGF as an injectable peptide faces significant challenges. The peptide is rapidly degraded in circulation (half-life of minutes), and delivering it to specific muscle tissue after systemic injection is problematic. PEGylated MGF (MGF with polyethylene glycol modification) has been developed to extend half-life, but the pharmacology of injected MGF differs fundamentally from the endogenous locally-produced form. No clinical trials have been conducted for MGF in muscle applications.
How These Compounds Compare#
| Feature | Follistatin | ACE-031 | GDF-8 (Myostatin) | IGF-1 LR3 | MGF |
|---|---|---|---|---|---|
| Approach | Natural inhibitor | Receptor decoy | Target protein | Anabolic signaling | Local growth factor |
| Pathway | Myostatin + activin inhibition | TGF-beta trapping | Smad2/3 (brake on growth) | PI3K/Akt/mTOR (growth signal) | Satellite cell activation |
| Evidence Level | Gene therapy trials | Phase 2 (discontinued) | Well-characterized | Clinical (for IGF-1 deficiency) | Preclinical only |
| FDA Status | Investigational | Discontinued | Endogenous target | Not approved (for muscle) | Not evaluated |
| Key Challenge | Off-target TGF-beta effects | Vascular safety | Mass vs. function gap | Cancer risk; hypoglycemia | Rapid degradation |
| Selectivity | Low (multiple TGF-beta) | Low (multiple TGF-beta) | N/A | Low (systemic growth) | High (local muscle) |
The Fundamental Challenge: Mass vs. Function#
The most important lesson from myostatin inhibitor development is the mass-function disconnect. Multiple compounds have successfully increased muscle mass in clinical trials while failing to proportionally improve muscle function. Several hypotheses explain this gap:
- Muscle quality — myostatin inhibition may produce muscle with different fiber type composition, contractile properties, or neuromuscular integration compared to exercise-induced hypertrophy
- Neural adaptation — strength is partly neurological (motor unit recruitment, firing rate). Pharmacological muscle growth may not produce the neural adaptations that accompany training-induced strength gains
- Dosing and duration — clinical trials may not have optimized dose or treatment duration to achieve functional improvements
This mass-function gap has led to disappointing clinical outcomes for multiple myostatin-targeted programs and remains the central challenge in the field.
Conclusion#
Myostatin inhibition represents one of the most scientifically compelling approaches to muscle growth, validated by dramatic natural experiments in animals and humans with myostatin deficiency. However, translating this biology into safe, effective therapeutics has proven far more challenging than initially anticipated.
The field has learned critical lessons: broad TGF-beta inhibition produces unacceptable vascular side effects (ACE-031), increased muscle mass does not automatically translate to improved function (multiple programs), and the safety concerns of systemic growth factor manipulation (IGF-1 LR3) are significant. Newer approaches — including more selective myostatin antibodies, gene therapy, and combination strategies — continue to advance.
For researchers interested in muscle growth peptides more broadly, see Top Peptides for Muscle Recovery and Growth. For dose calculations, visit the Dosing Calculator and HED Calculator. For safety guidance, see the Safety page.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Follistatin Overview and Research Guide
- Follistatin Dosing Protocols
- Follistatin Side Effects and Safety
- ACE-031 Overview and Research Guide
- ACE-031 Dosing Protocols
- ACE-031 Side Effects and Safety
- GDF-8 Overview and Research Guide
- GDF-8 Dosing Protocols
- GDF-8 Side Effects and Safety
- IGF-1 LR3 Overview and Research Guide
- IGF-1 LR3 Dosing Protocols
- IGF-1 LR3 Side Effects and Safety
- MGF Overview and Research Guide
- MGF Dosing Protocols
- MGF Side Effects and Safety

{kind=link}
Frequently Asked Questions About Myostatin Inhibitors and Muscle Growth Peptides: The Research Frontier
What does this article cover?
Myostatin inhibitors and muscle growth peptides — follistatin, ACE-031, GDF-8, IGF-1 LR3, and MGF — mechanisms and clinical evidence. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Follistatin, ACE-031, GDF-8, IGF-1 LR3, MGF. Key context: Follistatin (Endogenous glycoprotein that inhibits myostatin and activins, studied via gene therapy for muscle...); ACE-031 (Soluble activin receptor decoy that blocks myostatin signaling, tested in Duchenne muscular dystr...); GDF-8 (Myostatin itself (GDF-8) — the target of inhibitor strategies and the negative regulator of muscl...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Endogenous glycoprotein that inhibits myostatin and activins, studied via gene therapy for muscle.... Soluble activin receptor decoy that blocks myostatin signaling, tested in Duchenne muscular dystr.... Myostatin itself (GDF-8) — the target of inhibitor strategies and the negative regulator of muscl.... These takeaways are based on the research data available at the time of publication.
What is Follistatin and why is it significant?
Follistatin is a peptide discussed in this article because: Endogenous glycoprotein that inhibits myostatin and activins, studied via gene therapy for muscle-wasting diseases. For a complete profile of Follistatin, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptides for Muscle Growth and Preservation: Research Guide
Comprehensive guide to peptides for muscle growth and preservation — myostatin inhibitors (follistatin, bimagrumab, trevogrumab, apitegromab), IGF-1 pathway (IGF-1 LR3, MGF), and growth hormone secretagogues (ibutamoren, HGH) with clinical evidence and body recomp strategies.

Peptides for Sarcopenia: Research on Preserving Muscle Mass with Aging
Research review of peptides targeting sarcopenia and age-related muscle loss, including myostatin inhibitors, growth factors, and GH secretagogues with clinical trial data.

Top 10 Peptides for Muscle Recovery and Growth: Evidence-Based Research Guide
The 10 most studied peptides for muscle recovery and growth, including BPC-157, TB-500, IGF-1 LR3, ipamorelin, and follistatin, with mechanisms, evidence levels, and key research data.
You Might Also Like
Related content you may find interesting