Peptides for Sarcopenia: Research on Preserving Muscle Mass with Aging

Introduction#
Sarcopenia, the progressive loss of skeletal muscle mass and function with aging, is one of the most significant yet underappreciated conditions affecting older adults. Estimates suggest that 10 to 50 percent of adults over age 60 are affected, depending on diagnostic criteria and population studied. The consequences extend beyond weakness: sarcopenia is independently associated with increased fall risk, fractures, loss of independence, metabolic dysfunction, and mortality.
Despite its prevalence, sarcopenia has no FDA-approved pharmacological treatment. Exercise and nutritional interventions remain the standard of care, but adherence is often poor among the elderly and frail populations who need them most. This gap has driven significant research interest in peptide-based approaches that target the biological mechanisms underlying age-related muscle loss.
This guide examines the major peptide research strategies for sarcopenia, focusing on compounds with clinical trial data where available and clearly distinguishing between established evidence and preclinical findings. For general background on muscle-related peptides, see our guide on top peptides for muscle recovery and growth.
The Biology of Sarcopenia#
Understanding why muscle is lost with aging is essential for evaluating peptide interventions. Sarcopenia involves multiple converging mechanisms:
Hormonal Decline#
Growth hormone secretion decreases approximately 14 percent per decade after age 30, a phenomenon termed somatopause. The resulting decline in IGF-1 reduces anabolic signaling through the PI3K/Akt/mTOR pathway, shifting the balance toward muscle protein breakdown. Testosterone and estrogen levels also decline, further reducing anabolic drive.
Satellite Cell Dysfunction#
Muscle satellite cells, the resident stem cells responsible for muscle repair and regeneration, decline in both number and function with aging. This impairs the capacity to repair exercise-induced damage and regenerate muscle fibers after injury. The satellite cell pool in aged muscle can be 50 to 70 percent smaller than in young muscle, and the remaining cells show slower activation kinetics.
Increased Myostatin Signaling#
GDF-8 (myostatin), the primary negative regulator of muscle mass, shows increased expression and signaling activity in aged muscle. This shifts the balance toward muscle protein degradation and inhibits satellite cell proliferation. Myostatin signals through activin type II receptors (ActRIIA and ActRIIB), activating SMAD2/3 transcription factors that suppress muscle-specific gene expression.
Chronic Inflammation#
Aging is associated with a state of chronic low-grade inflammation (inflammaging) characterized by elevated levels of IL-6, TNF-alpha, and CRP. These inflammatory mediators directly promote muscle protein breakdown through activation of the ubiquitin-proteasome pathway and NF-kB signaling.
Mitochondrial Dysfunction#
Age-related decline in mitochondrial function reduces the energy available for muscle contraction and protein synthesis, contributing to both weakness and atrophy. Impaired mitochondrial quality control (mitophagy) leads to accumulation of dysfunctional mitochondria that generate excess reactive oxygen species, further damaging muscle proteins.
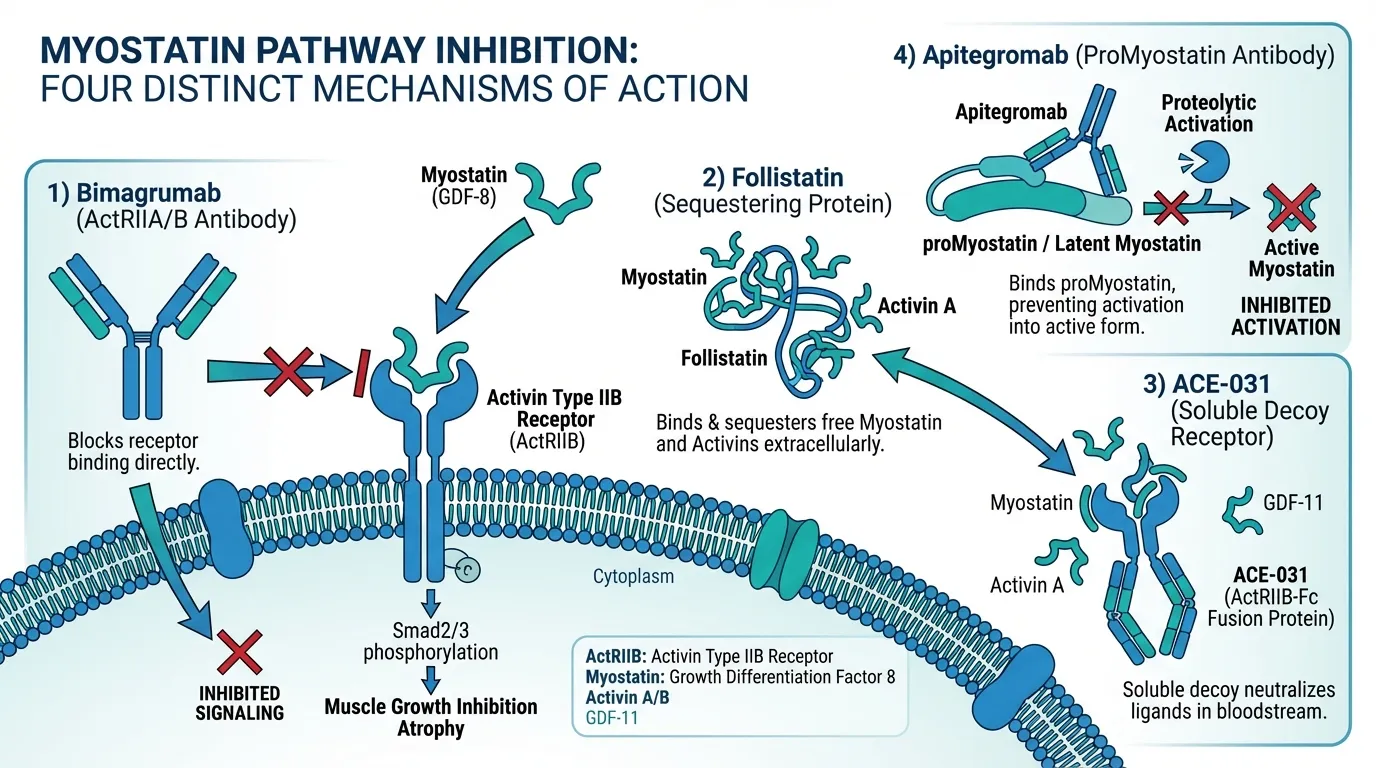
Myostatin Inhibition Approaches#
The myostatin pathway represents the most actively pursued pharmaceutical target for muscle wasting conditions, including sarcopenia. Multiple peptide and biologic strategies have been developed to inhibit this pathway at different points.
Bimagrumab: Receptor-Level Blockade#
Bimagrumab (BYM338) is a fully human monoclonal antibody developed by Novartis that blocks activin type II receptors (ActRIIA and ActRIIB). By targeting the receptor rather than individual ligands, bimagrumab provides broad inhibition of the myostatin/activin signaling cascade.
Sarcopenia Clinical Data#
Bimagrumab has been studied specifically in sarcopenia in a Phase 2 randomized controlled trial. In this study of older adults with low muscle mass and impaired mobility, bimagrumab treatment produced statistically significant increases in lean body mass compared to placebo. Participants received intravenous infusions of 30 mg/kg every four weeks.
The lean mass increases were dose-dependent and measurable by dual-energy X-ray absorptiometry (DXA). However, the improvements in lean mass did not consistently translate into corresponding improvements in functional measures such as gait speed or the Short Physical Performance Battery, raising questions about whether the accrued muscle mass is fully functional.
Obesity and Body Composition Data#
More compelling evidence comes from bimagrumab's Phase 2b trial in patients with obesity and type 2 diabetes. This 48-week study demonstrated a striking recomposition effect: approximately 20 percent reduction in fat mass with simultaneous 3.6 percent gain in lean mass, without caloric restriction or exercise requirements. While not a sarcopenia study, these body composition effects are directly relevant to the sarcopenic obesity phenotype that affects many older adults.
Current Status#
Bimagrumab is not FDA-approved for any indication. Clinical development has shifted focus from sarcopenia to obesity and metabolic disease, where the combined fat loss and lean mass gain appears commercially more compelling. For a detailed comparison of bimagrumab with another myostatin pathway approach, see our bimagrumab vs follistatin comparison.
Follistatin: Natural Myostatin Antagonist#
Follistatin is an endogenous glycoprotein that acts as the body's natural brake on myostatin signaling. It directly binds and sequesters myostatin, activin A, activin B, and other TGF-beta superfamily ligands in the extracellular space, preventing them from activating their receptors.
Preclinical Evidence#
The case for follistatin's muscle-building effects is compelling at the preclinical level. Overexpression of follistatin in mice produces dramatic muscle hypertrophy, with muscle mass increases of two to three times normal. The follistatin-overexpressing "mighty mouse" model demonstrates that removing the myostatin brake can produce striking muscle growth.
Gene Therapy Trials#
Follistatin has entered human clinical trials through AAV-mediated gene therapy. Mendell and colleagues conducted trials of AAV1-FS344 gene therapy in patients with Becker muscular dystrophy and inclusion body myositis. In the inclusion body myositis cohort, intramuscular injection of AAV1-follistatin showed improvements in the 6-minute walk test at 6 months. These trials provide proof of concept that sustained follistatin expression can affect human muscle, but the gene therapy approach is targeted at severe neuromuscular diseases rather than age-related sarcopenia.
Relevance to Sarcopenia#
For sarcopenia specifically, follistatin faces practical challenges. The recombinant protein has a short half-life requiring frequent dosing, and no standardized pharmaceutical formulation exists. Gene therapy is not a practical approach for age-related muscle loss given the irreversibility and the risk-benefit calculus in a generally healthy but aging population. Follistatin remains primarily of interest as a biological proof of concept rather than a near-term sarcopenia therapeutic.
ACE-031: Soluble Receptor Decoy#
ACE-031 (ramatercept) was a soluble ActRIIB-Fc fusion protein developed by Acceleron Pharma. It functioned as a decoy receptor, circulating in the bloodstream and binding myostatin, activin, GDF-11, and other TGF-beta superfamily ligands before they could reach cell-surface receptors.
Clinical History#
ACE-031 entered a Phase 2 clinical trial in boys with Duchenne muscular dystrophy (DMD). Early results demonstrated measurable increases in lean body mass and reductions in fat mass, confirming the expected pharmacological activity. However, the trial was halted when several participants experienced minor epistaxis (nosebleeds) and telangiectasias (dilated small blood vessels), likely related to the broad TGF-beta superfamily inhibition affecting vascular biology through inhibition of activin receptor-like kinase 1 (ALK1) signaling.
Lessons for Sarcopenia#
The ACE-031 experience illustrates a critical challenge in myostatin pathway therapeutics: selectivity. By trapping multiple TGF-beta superfamily ligands, ACE-031 affected vascular biology alongside muscle biology. This has driven the field toward more selective approaches. Acceleron pivoted to ACE-083, a locally administered follistatin-based compound (also discontinued), and eventually to luspatercept (ACE-536), which selectively targets the erythroid pathway and gained FDA approval for anemia.
For more on how ACE-031 compares with a more selective approach, see our ACE-031 vs Apitegromab comparison.
Apitegromab: Selective Myostatin Targeting#
Apitegromab (SRK-015) represents the next generation of myostatin pathway therapeutics, developed by Scholar Rock with a focus on improved selectivity. Rather than blocking the receptor or trapping multiple ligands, apitegromab is a monoclonal antibody that specifically targets proMyostatin and latent myostatin, preventing the proteolytic activation of myostatin from its inactive precursor forms.
Mechanism Advantages#
This selective approach is significant because it targets only myostatin, leaving other TGF-beta superfamily signaling intact. This specificity should avoid the vascular side effects seen with ACE-031 and the broader reproductive and metabolic effects of pan-receptor blockade. By targeting the activation step rather than the mature ligand or receptor, apitegromab addresses myostatin signaling at a different point in the pathway.
Clinical Development#
Apitegromab is being developed primarily for spinal muscular atrophy (SMA), where the Phase 3 SAPPHIRE trial is evaluating its ability to improve motor function in patients already receiving SMN-correcting therapies (nusinersen or risdiplam). Phase 2 TOPAZ data showed encouraging improvements in motor function measures in SMA Type 2 and Type 3 patients.
While SMA is not sarcopenia, the principle of selective myostatin inhibition demonstrated by apitegromab could be applicable to age-related muscle loss. If the SAPPHIRE trial demonstrates a clean safety profile and meaningful muscle effects, it would validate the selective approach for potential broader applications in muscle wasting.
Growth Factor Approaches#
MGF: Exercise-Mimetic Repair Signal#
MGF (Mechano Growth Factor) is a 24-amino acid peptide corresponding to the unique C-terminal E-domain of the IGF-1Ec splice variant. Unlike circulating IGF-1, MGF is expressed locally in muscle tissue specifically in response to mechanical loading and damage, making it a direct signal for muscle repair.
Relevance to Aging Muscle#
MGF expression is particularly relevant to sarcopenia because aging muscle shows blunted MGF expression in response to exercise. Studies have demonstrated that older adults produce significantly less MGF mRNA after resistance exercise compared to younger individuals, despite similar mechanical loading. This impaired MGF response may partly explain why aged muscle is slower to repair and adapt to exercise.
Preclinical Data#
In animal studies, exogenous MGF administration has enhanced satellite cell activation and muscle regeneration. MGF activates the muscle stem cell pool without immediately driving differentiation, expanding the available repair cells. The PEGylated form (PEG-MGF) has an extended half-life compared to native MGF, which degrades rapidly in circulation.
Evidence Assessment for Sarcopenia#
MGF's biological role in exercise-induced repair is established, but the therapeutic potential of exogenous MGF peptide for sarcopenia remains speculative. The key distinction is between the well-documented endogenous MGF response to exercise and the less-characterized effects of exogenous MGF administration. No human clinical trials have specifically evaluated MGF peptide for sarcopenia or age-related muscle loss. The rationale is biologically sound, but the clinical evidence is preclinical only.
The GH/IGF-1 Axis and Aging#
While not specifically classified as anti-sarcopenia peptides, growth hormone secretagogues address the somatopause component of sarcopenia. The age-related decline in GH and IGF-1 is one of the best-characterized hormonal contributors to muscle loss.
Growth hormone replacement in elderly individuals has shown modest increases in lean body mass in meta-analyses, but these increases often do not translate to proportional improvements in strength or function. GH therapy also carries side effects including fluid retention, joint pain, carpal tunnel syndrome, and potential effects on glucose metabolism, which limit its risk-benefit profile in aging populations.
GH secretagogues such as ipamorelin and sermorelin offer a more physiological approach by stimulating endogenous GH release while preserving pulsatile secretion and negative feedback regulation. These agents have better safety profiles than exogenous GH, but their specific efficacy for sarcopenia has not been demonstrated in dedicated clinical trials. For more on the GH secretagogue approach to muscle recovery, see the science of peptide-enhanced muscle recovery.
Comparing Anti-Sarcopenia Strategies#
The following table summarizes the key approaches and their evidence status:
| Approach | Peptide/Biologic | Target | Evidence Level | Key Advantage | Key Limitation |
|---|---|---|---|---|---|
| Receptor blockade | Bimagrumab | ActRIIA/ActRIIB | Phase 2 (sarcopenia) | Proven lean mass gain in humans | Lean mass gain may not equal functional improvement |
| Ligand sequestration | Follistatin | Myostatin, activins | Phase 1 (gene therapy) | Potent preclinical muscle growth | Short half-life, no standard formulation |
| Decoy receptor | ACE-031 | Myostatin, activins, GDF-11 | Phase 2 (discontinued) | Demonstrated lean mass increase | Vascular side effects, discontinued |
| Selective inhibition | Apitegromab | ProMyostatin/latent myostatin | Phase 3 (SMA) | Myostatin-specific selectivity | Not yet studied in sarcopenia |
| Growth factor | MGF | Satellite cells | Preclinical | Muscle-specific repair signal | No human clinical data |
| Negative regulator | GDF-8 (myostatin) | ActRIIB/SMAD2/3 | Target validated | Most validated muscle growth target | Therapeutic = inhibiting this pathway |
Challenges in Sarcopenia Drug Development#
The Lean Mass vs. Function Gap#
One of the most persistent challenges in sarcopenia drug development has been the dissociation between increases in lean body mass and improvements in physical function. Bimagrumab's sarcopenia trial demonstrated this clearly: statistically significant lean mass gains did not consistently produce corresponding improvements in gait speed or physical performance. This suggests that simply adding muscle mass is not sufficient; the accrued muscle must be functional, properly innervated, and integrated into movement patterns.
This gap has led to debate about whether DXA-measured lean mass is the right endpoint for sarcopenia trials. Total lean mass includes water content and non-contractile components, which may not reflect true functional muscle capacity. Newer imaging approaches (MRI, CT) that can distinguish muscle quality (fat infiltration, fiber density) may prove more informative.
Regulatory Pathway Uncertainty#
Until recently, sarcopenia lacked a formal disease classification, which complicated regulatory pathways for drug approval. The inclusion of sarcopenia in the ICD-10 classification (code M62.84) was an important step, but the FDA has not yet established clear guidance on acceptable endpoints for sarcopenia drug trials. This regulatory ambiguity has discouraged some pharmaceutical companies from pursuing sarcopenia indications.
Combination Approach Potential#
Given the multifactorial nature of sarcopenia, single-target approaches may be insufficient. A combination strategy pairing a myostatin pathway inhibitor (to remove the brake on muscle growth) with exercise or a GH secretagogue (to provide anabolic drive) could potentially overcome the lean mass-to-function gap. However, no such combination trials have been conducted in sarcopenia.
The Role of Exercise#
No discussion of sarcopenia interventions is complete without emphasizing that resistance exercise remains the most effective intervention for maintaining muscle mass and function with aging. Exercise simultaneously activates multiple anabolic pathways: it stimulates GH secretion, increases local MGF expression, reduces myostatin levels, activates satellite cells, and improves neuromuscular coordination.
The peptide strategies discussed here are best understood as potential complements to exercise, not replacements. Even bimagrumab's sarcopenia trial was designed with a background of standard-of-care recommendations including physical activity. For individuals who cannot exercise due to severe frailty, injury, or illness, pharmacological approaches become more important, but this represents a specific clinical scenario rather than a general recommendation.
Future Directions#
More Selective Myostatin Inhibitors#
The field is moving toward increasingly selective approaches. Apitegromab's targeting of the myostatin activation step, rather than the receptor or mature ligand, represents this trend. Future molecules may achieve even greater selectivity, potentially targeting muscle-specific myostatin activation while leaving systemic signaling intact.
Combination Therapies#
Combining myostatin inhibition with anabolic stimulation (GH secretagogues, exercise programs, or nutritional interventions) represents a logical next step. The rationale is straightforward: removing the brake (myostatin inhibition) while pressing the accelerator (anabolic signaling) should produce greater effects than either alone.
Biomarkers and Patient Selection#
Identifying which sarcopenic patients are most likely to respond to specific interventions could improve clinical trial success. Myostatin levels, satellite cell function, inflammatory markers, and hormone profiles could potentially guide treatment selection.
Senolytics and Muscle Aging#
Emerging research on senescent cells in aged muscle suggests that clearing these cells could improve the muscle stem cell niche and restore regenerative capacity. While not peptide-based, this approach addresses a root cause of sarcopenia that complements the pathway-specific strategies discussed above.
Conclusion#
Peptide research for sarcopenia has produced several biologically compelling strategies, with myostatin pathway inhibition being the most clinically advanced. Bimagrumab has the strongest human evidence, with Phase 2 sarcopenia data and Phase 2b obesity data demonstrating clear effects on lean mass and body composition. Apitegromab represents the most promising current development program for selective myostatin inhibition, though its clinical focus is SMA rather than sarcopenia.
The persistent challenge remains translating lean mass gains into functional improvements that meaningfully affect quality of life for older adults. The lessons from ACE-031's discontinuation and follistatin's delivery challenges underscore that efficacy alone is insufficient -- safety, selectivity, and practicality all matter for a condition affecting a large, generally healthy aging population.
Despite significant investment and strong preclinical validation, sarcopenia remains without an FDA-approved pharmacological treatment. The peptide approaches reviewed here represent the most advanced candidates, but all face the common challenge of proving that pharmacologically increased muscle mass translates to meaningful clinical benefit in older adults. For researchers and clinicians, the field continues to evolve rapidly, and the combination of more selective molecules, better endpoints, and combination strategies may ultimately close the gap between biological promise and clinical reality.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- ACE-031 Overview and Research Guide
- ACE-031 Dosing Protocols
- ACE-031 Side Effects and Safety
- Apitegromab Overview and Research Guide
- Apitegromab Dosing Protocols
- Apitegromab Side Effects and Safety
- Bimagrumab Overview and Research Guide
- Bimagrumab Dosing Protocols
- Bimagrumab Side Effects and Safety
- Follistatin Overview and Research Guide
- Follistatin Dosing Protocols
- Follistatin Side Effects and Safety
- GDF-8 Overview and Research Guide
- GDF-8 Dosing Protocols
- GDF-8 Side Effects and Safety
- MGF Overview and Research Guide
- MGF Dosing Protocols
- MGF Side Effects and Safety

{kind=link}
Frequently Asked Questions About Peptides for Sarcopenia: Research on Preserving Muscle Mass with Aging
What does this article cover?
Research review of peptides targeting sarcopenia and age-related muscle loss, including myostatin inhibitors, growth factors, and GH secretagogues with clinical trial data. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers ACE-031, Apitegromab, Bimagrumab, Follistatin, GDF-8, MGF. Key context: ACE-031 (Soluble ActRIIB-Fc decoy receptor that traps myostatin and other TGF-beta ligands, studied in Duc...); Apitegromab (Anti-proMyostatin antibody with selective mechanism, currently in Phase 3 SAPPHIRE trial for spin...); Bimagrumab (Monoclonal antibody blocking activin type II receptors, with Phase 2 data in sarcopenia and obesi...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Peptides for Sarcopenia: Research on Preserving Muscle Mass with Aging." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Soluble ActRIIB-Fc decoy receptor that traps myostatin and other TGF-beta ligands, studied in Duc.... Anti-proMyostatin antibody with selective mechanism, currently in Phase 3 SAPPHIRE trial for spin.... Monoclonal antibody blocking activin type II receptors, with Phase 2 data in sarcopenia and obesi.... These takeaways are based on the research data available at the time of publication.
What is ACE-031 and why is it significant?
ACE-031 is a peptide discussed in this article because: Soluble ActRIIB-Fc decoy receptor that traps myostatin and other TGF-beta ligands, studied in Duchenne muscular dystrophy before discontinuation. For a complete profile of ACE-031, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptides for Muscle Growth and Preservation: Research Guide
Comprehensive guide to peptides for muscle growth and preservation — myostatin inhibitors (follistatin, bimagrumab, trevogrumab, apitegromab), IGF-1 pathway (IGF-1 LR3, MGF), and growth hormone secretagogues (ibutamoren, HGH) with clinical evidence and body recomp strategies.

Next-Generation Myostatin Inhibitors: Bimagrumab, Trevogrumab, and Apitegromab Compared
A research review comparing bimagrumab, trevogrumab, and apitegromab — three anti-myostatin antibodies in clinical development for muscle preservation, obesity, and spinal muscular atrophy.

Myostatin Inhibitors and Muscle Growth Peptides: The Research Frontier
Myostatin inhibitors and muscle growth peptides — follistatin, ACE-031, GDF-8, IGF-1 LR3, and MGF — mechanisms and clinical evidence.
You Might Also Like
Related content you may find interesting