Non-GLP-1 Approaches to Weight Loss: Amylin, Melanocortin, and Myostatin Pathways

Introduction#
The GLP-1 receptor agonist revolution has dominated the weight loss landscape, with semaglutide, tirzepatide, and newer multi-agonists achieving unprecedented weight loss in clinical trials. But GLP-1 agonists are not the only pathway to pharmacological weight management. Several other peptide-based mechanisms are advancing through clinical development, targeting fundamentally different biological systems.
This article reviews three non-GLP-1 pathways with active clinical programs: amylin analogs (cagrilintide, petrelintide, pramlintide), melanocortin receptor agonists (setmelanotide, bivamelagon), and anti-myostatin antibodies (bimagrumab). Each targets a distinct aspect of energy balance -- appetite, satiety, central weight regulation, or body composition -- and some are being developed as standalone therapies while others are positioned as GLP-1 adjuncts.
For GLP-1-specific weight loss data, see 5 Most Promising Peptides for Weight Loss and GLP-1 Drugs Ranked by Weight Loss.
The Amylin Pathway#
Amylin is a pancreatic hormone co-secreted with insulin after meals. It slows gastric emptying, suppresses glucagon secretion, and promotes satiety through the area postrema in the brainstem -- a mechanism complementary to but distinct from GLP-1 signaling. The amylin pathway has been validated by three generations of analogs with progressively better pharmacology.
Pramlintide: The First-Generation Proof of Concept#
Pramlintide (Symlin) was FDA-approved in 2005 as an adjunct to insulin therapy for type 1 and type 2 diabetes. It is a synthetic analog of human amylin with three proline substitutions that prevent the aggregation problems that made native amylin unsuitable as a drug.
Key data:
- Modest weight loss of 1-2 kg in diabetes trials (not its primary indication)
- Required three daily injections due to a short half-life
- Demonstrated that amylin receptor agonism reduces food intake and body weight in humans
- Limited by injection frequency and nausea
Pramlintide's clinical utility was constrained by its dosing burden, but it established the biological validity of amylin-based weight loss. Its development paved the way for long-acting analogs.
Cagrilintide: The Long-Acting Revolution#
Cagrilintide is Novo Nordisk's long-acting amylin analog, designed for once-weekly subcutaneous injection. It represents a generational advance over pramlintide's three-daily dosing.
Key data:
- Phase 2 monotherapy (706 participants, 26 weeks): Weight reductions of 6.0% (0.3 mg), 9.0% (1.2 mg), 9.7% (2.4 mg), and 10.8% (4.5 mg) versus 3.0% placebo
- As part of CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg): 20.4% weight loss at 68 weeks in the Phase 3 REDEFINE 1 trial (3,417 participants)
- The CagriSema combination NDA has been filed with the FDA
Cagrilintide's importance extends beyond its monotherapy weight loss. Its combination with semaglutide demonstrated that amylin and GLP-1 receptor agonism are truly complementary -- producing greater weight loss together than either alone. For a detailed comparison, see CagriSema vs Retatrutide.
Petrelintide: The Next-Generation Amylin Analog#
Petrelintide is Zealand Pharma's next-generation long-acting amylin analog, positioned as a potential foundational therapy for obesity with potential for lean muscle preservation.
Key data:
- Phase 2b ZUPREME-1 trial (obesity without T2D, 42 weeks) completed enrollment in March 2025; topline results expected H1 2026
- Phase 2b ZUPREME-2 trial (obesity with T2D, 28 weeks) enrollment completed in November 2025
- Roche entered a major collaboration and licensing agreement with Zealand Pharma in March 2025 to co-develop petrelintide and combination products, including a fixed-dose combination with CT-388 (Roche's GLP-1/GIP dual agonist)
Petrelintide's value proposition centers on tolerability and lean mass preservation. Early data suggests amylin analogs may deliver weight loss comparable to GLP-1 agonists but with a better patient experience -- potentially less nausea -- and improved body composition outcomes. The Roche/Zealand combination strategy (petrelintide + CT-388) mirrors Novo Nordisk's CagriSema approach of pairing amylin with incretin agonism.
Amylin Pathway Summary#
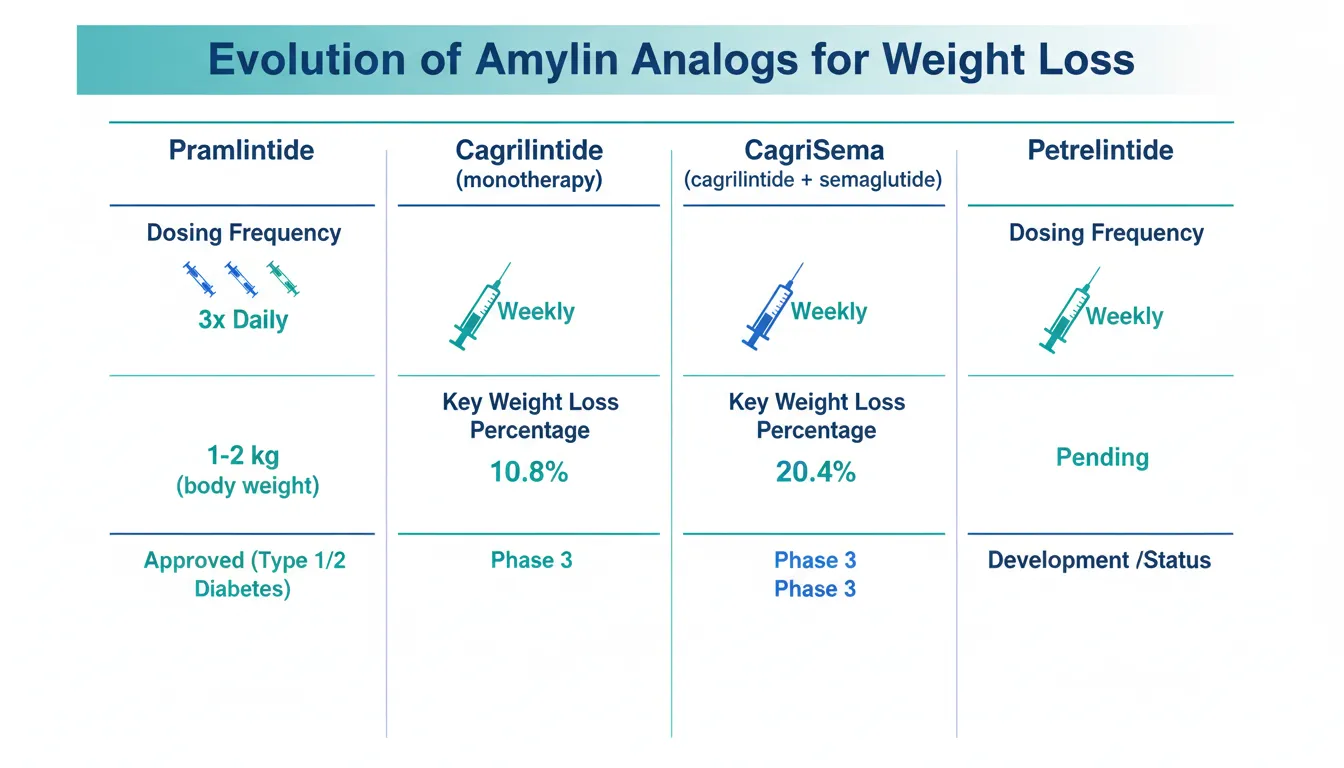
| Compound | Developer | Dosing | Phase | Key Weight Loss Data |
|---|---|---|---|---|
| Pramlintide | AstraZeneca | 3x daily SC | Approved (T1D/T2D) | 1-2 kg (diabetes adjunct) |
| Cagrilintide | Novo Nordisk | Weekly SC | Phase 3 (as CagriSema) | 10.8% mono; 20.4% combo |
| Petrelintide | Zealand / Roche | Weekly SC | Phase 2b | Results pending (H1 2026) |
The Melanocortin Pathway#
The melanocortin-4 receptor (MC4R) is a central regulator of appetite and energy balance in the hypothalamus. MC4R activation suppresses appetite and increases energy expenditure. Loss-of-function MC4R mutations are the most common monogenic cause of severe obesity, affecting approximately 2-6% of people with severe obesity.
Setmelanotide: Targeted Genetic Obesity Treatment#
Setmelanotide (Imcivree) was FDA-approved in 2020 as the first MC4R agonist for chronic weight management -- specifically for patients aged 6 and older with obesity due to POMC deficiency, PCSK1 deficiency, or leptin receptor (LEPR) deficiency.
Key data:
- In POMC deficiency: Mean weight loss of 25.6% at 1 year
- In LEPR deficiency: Mean weight loss of 12.5% at 1 year
- Targets three rare genetic obesity conditions that are upstream of MC4R signaling
- Daily subcutaneous injection
Setmelanotide's clinical success validated the melanocortin pathway for weight management but in a very narrow patient population (estimated 1,000-3,000 patients in the US with these specific genetic deficiencies). The question has been whether MC4R agonism can be extended to broader obesity populations.
Bivamelagon: Oral MC4R Agonism for Broader Populations#
Bivamelagon is Rhythm Pharmaceuticals' oral MC4R agonist being developed for acquired hypothalamic obesity (AHO) -- a condition typically caused by brain tumors or their treatment that damages the hypothalamus.
Key Phase 2 data (SIGNAL trial):
- 600 mg cohort (n=8): -9.3% BMI reduction from baseline (p=0.0004)
- 400 mg cohort (n=7): -7.7% BMI reduction (p=0.0002)
- 200 mg cohort (n=6): -2.7% BMI reduction (p=0.018)
- Placebo cohort (n=7): +2.2% BMI increase
- Safety consistent with MC4R mechanism; most common adverse events were mild diarrhea and nausea
Bivamelagon's significance lies in two aspects: it is oral (most obesity peptides are injectable), and it targets AHO -- a condition notoriously resistant to conventional weight management, including GLP-1 agonists. Rhythm plans to seek regulatory input on Phase 3 trial design.
Melanocortin Pathway Summary#
| Compound | Developer | Route | Phase | Target Population |
|---|---|---|---|---|
| Setmelanotide | Rhythm | Daily SC | Approved | POMC, PCSK1, LEPR deficiency |
| Bivamelagon | Rhythm | Daily oral | Phase 2 | Acquired hypothalamic obesity |
The Myostatin/Body Composition Pathway#
While amylin and melanocortin approaches reduce total body weight, the myostatin pathway addresses a different but increasingly recognized problem: the quality of weight loss. GLP-1 agonists produce substantial weight loss, but 25-40% typically comes from lean mass (muscle), which has negative implications for metabolic health, physical function, and long-term weight maintenance.
Bimagrumab: Fat Loss with Muscle Preservation#
Bimagrumab is an anti-activin type II receptor (ActRII) antibody that simultaneously reduces fat mass and increases lean mass -- a dual effect not seen with any other single agent in the obesity space.
Key data:
- BELIEVE trial (Phase 2b, 507 participants): Bimagrumab + semaglutide achieved 22.1% weight loss with 92.8% of weight loss from fat. Semaglutide alone achieved 15.7% weight loss with 71.8% from fat
- Monotherapy: Bimagrumab alone produced 10.8% weight loss while increasing lean mass by 2.5%
- Earlier Phase 2 (T2D + obesity): Significant reductions in fat mass with simultaneous lean mass increases versus placebo over 48 weeks
Bimagrumab is being positioned as a GLP-1 adjunct rather than a standalone obesity treatment. For detailed comparison with other myostatin inhibitors, see [Next-Generation Myostatin Inhibitors: Bimagrumab, Trevogrumab, and Apitegromab](/blog/myostatin-inhibitor-peptides-compared).
How These Pathways Compare to GLP-1#
| Pathway | Mechanism | Weight Loss Range | Unique Advantage | Limitation |
|---|---|---|---|---|
| GLP-1 agonism | Appetite suppression, insulin, gastric emptying | 15-25% (Phase 3) | Proven, approved, CV benefit | GI side effects, lean mass loss |
| Amylin agonism | Satiety, gastric emptying, glucagon suppression | 10-11% mono; 20% combo | Complementary to GLP-1; may preserve lean mass | No standalone approval for obesity |
| MC4R agonism | Central appetite suppression, energy expenditure | 9-26% (genetic obesity) | Targets genetic/hypothalamic obesity | Narrow approved populations |
| Anti-myostatin | Blocks muscle growth inhibition | 10-22% (with GLP-1) | Preserves/increases lean mass | IV infusion; no standalone approval |
The Combination Future#
The most clinically advanced development in non-GLP-1 weight management is the combination strategy -- pairing non-GLP-1 mechanisms with GLP-1 agonists to achieve superior outcomes:
- CagriSema (cagrilintide + semaglutide): Amylin + GLP-1. Phase 3 complete, NDA filed. 20.4% weight loss.
- Petrelintide + CT-388 (amylin + GLP-1/GIP): Roche/Zealand combination in planning. Aims to pair amylin with a dual incretin agonist.
- Bimagrumab + semaglutide (anti-myostatin + GLP-1): Phase 2b complete. 22.1% weight loss with 93% from fat.
- Trevogrumab + semaglutide (anti-myostatin + GLP-1): Regeneron Phase 2. Targeting muscle preservation during GLP-1 weight loss.
The overarching trend is clear: the next generation of obesity treatments will likely combine multiple mechanisms to maximize weight loss while improving its quality (more fat, less muscle).
Important Considerations#
Evidence Hierarchy#
These non-GLP-1 approaches vary significantly in evidence maturity:
- FDA-approved: Pramlintide (diabetes), setmelanotide (genetic obesity) -- proven in narrow indications
- Phase 3 / NDA filed: Cagrilintide (as CagriSema) -- strong evidence in large trials
- Phase 2b: Petrelintide, bivamelagon, bimagrumab -- promising but pending Phase 3 confirmation
- Phase 2: Trevogrumab combinations -- early data
Not All Weight Loss Is Equal#
A recurring theme across these pathways is that total weight loss is not the only metric that matters. Body composition -- the ratio of fat to lean mass lost -- is increasingly recognized as critical for long-term health outcomes. The amylin pathway may offer better tolerability, the melanocortin pathway may reach patients unresponsive to GLP-1s, and the myostatin pathway directly addresses lean mass preservation.
Conclusion#
GLP-1 receptor agonists have set a high bar for obesity treatment, but they are not the complete answer. Amylin analogs provide complementary appetite suppression through distinct neural pathways and may offer better tolerability. Melanocortin agonists reach patients with genetic and hypothalamic obesity who respond poorly to GLP-1s. Anti-myostatin antibodies address the quality of weight loss by preserving and even building muscle during fat reduction.
The most likely clinical future involves combinations: amylin + incretin agonism (CagriSema, petrelintide + CT-388) for maximum appetite suppression, and anti-myostatin + GLP-1 (bimagrumab + semaglutide) for optimized body composition. These non-GLP-1 pathways are not competitors to GLP-1 therapy -- they are its complement.
For related reading, see 5 Most Promising Peptides for Weight Loss, GLP-1 Drugs Ranked by Weight Loss, GLP-1 and Amylin Combination Therapy, and Next-Generation Myostatin Inhibitors.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Cagrilintide Overview and Research Guide
- Cagrilintide Dosing Protocols
- Cagrilintide Side Effects and Safety
- Petrelintide Overview and Research Guide
- Petrelintide Dosing Protocols
- Petrelintide Side Effects and Safety
- Pramlintide Overview and Research Guide
- Pramlintide Dosing Protocols
- Pramlintide Side Effects and Safety
- Setmelanotide Overview and Research Guide
- Setmelanotide Dosing Protocols
- Setmelanotide Side Effects and Safety
- Bivamelagon Overview and Research Guide
- Bivamelagon Dosing Protocols
- Bivamelagon Side Effects and Safety
- Bimagrumab Overview and Research Guide
- Bimagrumab Dosing Protocols
- Bimagrumab Side Effects and Safety

{kind=link}
Frequently Asked Questions About Non-GLP-1 Approaches to Weight Loss: Amylin, Melanocortin, and Myostatin Pathways
What does this article cover?
A research review of non-GLP-1 peptide approaches to weight loss — amylin analogs (cagrilintide, petrelintide, pramlintide), melanocortin agonists (setmelanotide, bivamelagon), and anti-myostatin antibodies (bimagrumab). This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Cagrilintide, Petrelintide, Pramlintide, Setmelanotide, Bivamelagon, Bimagrumab. Key context: Cagrilintide (Long-acting amylin analog that produces clinically significant weight loss as monotherapy and for...); Petrelintide (Next-generation long-acting amylin analog developed by Zealand Pharma with Roche partnership, in ...); Pramlintide (FDA-approved amylin analog for diabetes that demonstrated the weight loss potential of amylin rec...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Long-acting amylin analog that produces clinically significant weight loss as monotherapy and for.... Next-generation long-acting amylin analog developed by Zealand Pharma with Roche partnership, in .... FDA-approved amylin analog for diabetes that demonstrated the weight loss potential of amylin rec.... These takeaways are based on the research data available at the time of publication.
What is Cagrilintide and why is it significant?
Cagrilintide is a peptide discussed in this article because: Long-acting amylin analog that produces clinically significant weight loss as monotherapy and forms half of the CagriSema combination. For a complete profile of Cagrilintide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

GLP-1 Plus Amylin: Why Combination Therapy Is the Next Frontier
A research review of GLP-1 and amylin combination therapy for obesity, covering CagriSema, amycretin, petrelintide, pramlintide, and the science behind dual appetite hormone targeting.

Preserving Muscle Mass on GLP-1 Medications: Research and Strategies
A research review of lean mass loss during GLP-1 treatment, with DEXA data from STEP and SURMOUNT trials, and emerging strategies including bimagrumab, resistance training, and high-protein diets.

Finnrick Analytics Review: Transparency Concerns and Conflicts of Interest (2026)
Is Finnrick Analytics trustworthy? We examine COI gaps, vendor pay-for-play, 15% lab discrepancies, and their astroturfing job listing. Full analysis.
You Might Also Like
Related content you may find interesting