GLP-1 Side Effects Compared: Which Drug Is Best Tolerated?

Introduction#
Gastrointestinal side effects are the defining tolerability challenge of GLP-1 receptor agonists. Nausea, vomiting, diarrhea, and constipation affect a substantial proportion of patients, and they are the primary reason patients discontinue treatment. As the obesity drug pipeline expands from semaglutide and tirzepatide to triple agonists, oral formulations, and biased agonists, the side effect profiles are diverging in important ways.
This guide compares GI adverse event rates across seven drugs spanning approved therapies, next-generation multi-receptor agonists, and novel biased agonists specifically engineered for improved tolerability. Understanding these differences is essential for evaluating the risk-benefit profile of each agent.
Important: Semaglutide and tirzepatide are FDA-approved. All other agents discussed are investigational. Cross-trial comparisons have inherent limitations due to differences in populations, titration protocols, and study designs.
The GI Side Effect Landscape#
Why GLP-1 Drugs Cause GI Side Effects#
GLP-1 receptor activation produces gastrointestinal effects through two primary mechanisms:
-
Delayed gastric emptying: GLP-1 slows the rate at which food moves from the stomach to the small intestine. While this contributes to satiety and weight loss, it also produces nausea, bloating, and constipation.
-
Central nausea signaling: GLP-1 receptors in the area postrema (the brain's vomiting center) are activated by circulating drug, producing nausea independently of gastric effects.
These are on-target effects -- the same receptor activation that suppresses appetite and lowers blood glucose also causes GI symptoms. This means GI side effects are, to some degree, inherent to the mechanism. The challenge for drug developers is to decouple efficacy from tolerability.
The Beta-Arrestin Hypothesis#
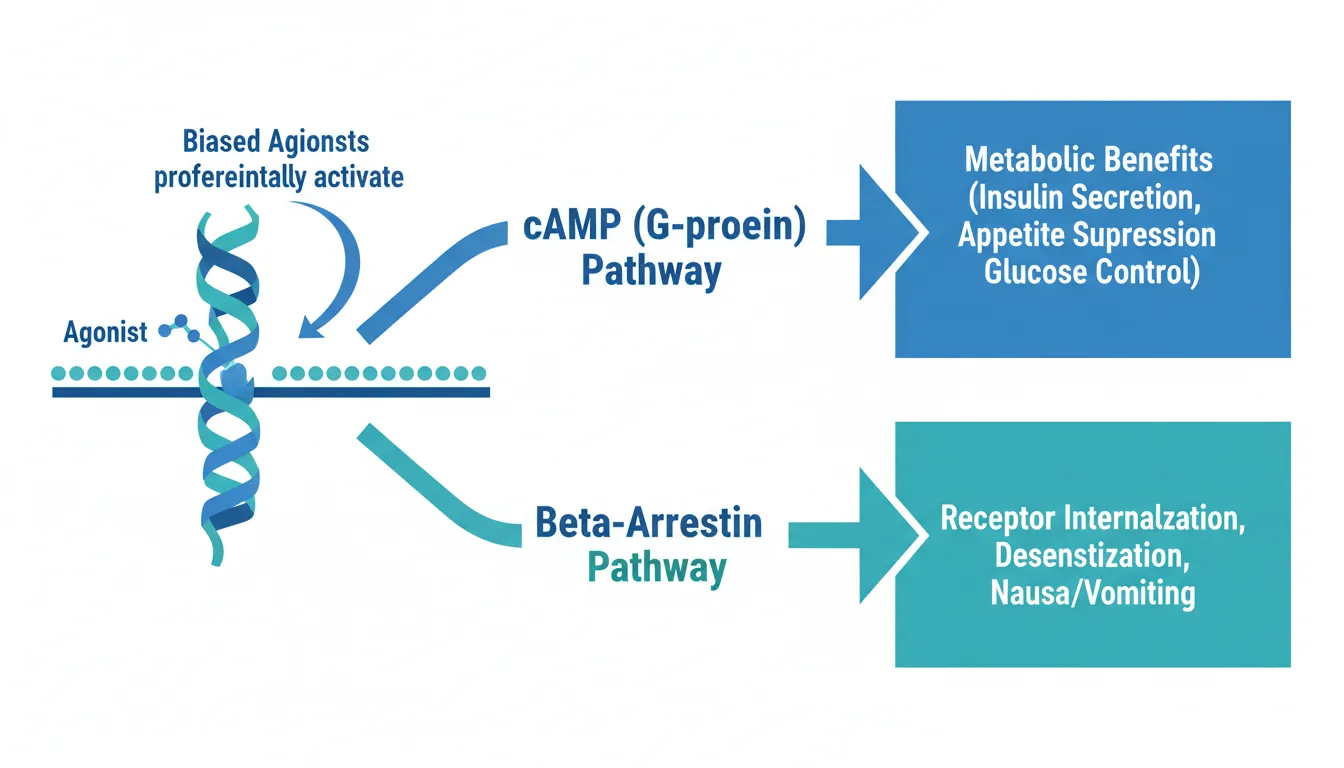
A key insight driving next-generation drug design is the role of beta-arrestin in GLP-1 receptor signaling. When a GLP-1 agonist binds its receptor, it can activate two downstream pathways:
- cAMP (G-protein) pathway: Mediates the metabolic benefits (insulin secretion, appetite suppression, glucose control)
- Beta-arrestin pathway: Triggers receptor internalization and desensitization, and may contribute to nausea and vomiting
Drugs that preferentially activate the cAMP pathway while minimizing beta-arrestin recruitment -- called "biased agonists" -- may maintain efficacy while reducing GI side effects. This hypothesis is being tested clinically by ecnoglutide and CT-388.
Drug-by-Drug Side Effect Profiles#
Semaglutide (Wegovy/Ozempic)#
Semaglutide is the most extensively studied GLP-1 agonist, with GI data from the STEP program (obesity) and SUSTAIN program (T2D).
STEP 1 (semaglutide 2.4 mg, 68 weeks):
| Adverse Event | Semaglutide 2.4 mg | Placebo |
|---|---|---|
| Any GI event | 74.2% | 47.9% |
| Nausea | 44.2% | 17.4% |
| Diarrhea | 30.0% | 15.7% |
| Vomiting | 24.8% | 6.4% |
| Constipation | 24.2% | 11.1% |
Discontinuation due to GI AEs: 4.3% (vs 0.7% placebo)
Key characteristics:
- GI events are most common during dose escalation and generally diminish over time
- Severe GI events occur in approximately 4% of patients
- The 16-week dose escalation schedule (0.25 mg to 2.4 mg) was designed to minimize GI impact
Tirzepatide (Zepbound/Mounjaro)#
Tirzepatide adds GIP receptor agonism to GLP-1 activity. The SURMOUNT trials provide comprehensive GI data across three dose levels.
SURMOUNT-1 (tirzepatide, 72 weeks):
| Adverse Event | 5 mg | 10 mg | 15 mg | Placebo |
|---|---|---|---|---|
| Nausea | 24.6% | 33.3% | 31.0% | 9.5% |
| Diarrhea | 18.7% | 21.2% | 23.0% | 7.3% |
| Vomiting | 8.3% | 10.7% | 12.2% | 1.7% |
| Constipation | 17.1% | 17.1% | 11.7% | 4.8% |
Discontinuation due to AEs: 4.3% (5 mg), 7.1% (10 mg), 6.2% (15 mg) vs 2.6% placebo
Key characteristics:
- GI events occur primarily during dose escalation
- The GIP component does not appear to add substantial GI burden beyond GLP-1 effects
- Pooled SURMOUNT-1 to -4 analysis showed treatment discontinuation due to GI AEs ranged from 1.0% to 10.5%
Retatrutide#
Retatrutide adds glucagon receptor agonism to GLP-1 and GIP, creating a triple agonist. The TRIUMPH-4 Phase 3 trial revealed both expected and unexpected side effects.
TRIUMPH-4 (retatrutide, 68 weeks):
| Adverse Event | Retatrutide (pooled) | Placebo |
|---|---|---|
| Nausea | 43% | -- |
| Diarrhea | 33% | -- |
| Vomiting | 21% | -- |
| Dysesthesia | 8.8% (9 mg) / 20.9% (12 mg) | 0.7% |
Discontinuation due to AEs: 12.2% (9 mg), 18.2% (12 mg) vs 4.0% placebo
Key characteristics:
- Highest GI adverse event rates among the drugs compared here
- Dysesthesia is a novel safety signal -- abnormal touch sensations affecting up to 21% at the 12 mg dose, not seen in Phase 2. This was not observed with GLP-1 or GLP-1/GIP agonists and may be related to the glucagon component
- Higher discontinuation rates than semaglutide or tirzepatide, though some discontinuations were due to "perceived excessive weight loss" in patients with lower BMI
- The higher GI burden correlates with retatrutide's higher weight loss (28.7%)
Orforglipron#
Orforglipron is an oral non-peptide GLP-1 agonist. The ATTAIN-1 Phase 3 trial provides the first large-scale GI data for an oral small-molecule GLP-1 drug.
ATTAIN-1 (orforglipron, 72 weeks):
| Adverse Event | 6 mg | 12 mg | 36 mg | Placebo |
|---|---|---|---|---|
| Nausea | 28.9% | 35.9% | 33.7% | 10.4% |
| Vomiting | 5% | 7% | 14% | 1% |
| Diarrhea | Reported | Reported | Reported | -- |
Discontinuation due to AEs: 5.3-10.3% (orforglipron) vs 2.7% placebo
Key characteristics:
- GI profile is broadly similar to injectable GLP-1 agonists despite oral route
- Nausea rates are comparable to tirzepatide
- The oral formulation does not appear to worsen GI tolerability relative to SC injection
- Safety profile described as "consistent with injectable GLP-1 medicines"
Ecnoglutide#
Ecnoglutide is a cAMP-biased GLP-1 receptor agonist developed by Sciwind Biosciences. It was specifically designed to preferentially activate the G-protein/cAMP pathway while minimizing beta-arrestin recruitment.
SLIMMER Phase 3 (ecnoglutide, 40 weeks):
| Feature | Ecnoglutide | Placebo |
|---|---|---|
| Any TEAE | 93% | 84% |
| GI events | Most common, mild-moderate | -- |
| Treatment discontinuation due to AEs | ~2% (10 of ~498) | -- |
| Weight loss (2.4 mg) | 13.2% | +0.1% |
Key characteristics:
- Lowest discontinuation rate among the drugs compared here (~2%)
- GI events described as "mild-to-moderate" with no detailed breakdown of individual symptom rates publicly available
- The biased agonism profile may contribute to reduced severity of GI effects
- Discontinuation rates of 6-11% across dose groups (including all causes, not just AEs)
- Demonstrates that cAMP bias may translate to a clinically meaningful tolerability advantage
CT-388#
CT-388 is a signal-biased dual GLP-1/GIP receptor agonist developed by Roche/Genentech. It was designed with minimal beta-arrestin recruitment at both receptors, aiming to reduce receptor desensitization and improve tolerability.
Phase 1b (CT-388, 24 weeks):
| Adverse Event | CT-388 (titration) | CT-388 (maintenance) |
|---|---|---|
| Nausea | 83.3% | 54% |
| Vomiting | 75.0% | 33% |
| Diarrhea | 54.2% | 50% |
| Constipation | 58.3% | -- |
Phase 2 (CT-388 up to 24 mg, 48 weeks):
- GI AEs described as "mild-to-moderate" and "generally consistent with incretin class"
- Discontinuation due to AEs: 5.9% (vs 1.3% placebo)
- Weight loss: 22.5% placebo-adjusted at 48 weeks
Key characteristics:
- Phase 1b showed very high absolute GI rates during titration, but these declined substantially during maintenance
- Phase 2 data showed a much more favorable tolerability profile with a low discontinuation rate of 5.9%
- The signal-biased design appears to provide sustained receptor activation without desensitization
- Despite high initial GI rates, very few patients discontinued, suggesting events were transient and manageable
- Phase 3 (ENITH program) planned for 2026
Bioglutide (NA-931)#
Bioglutide is the first oral quadruple receptor agonist (GLP-1, GIP, glucagon, and IGF-1), developed by Biomed Industries.
Phase 2 (NA-931, 13 weeks):
| Adverse Event | NA-931 | Placebo |
|---|---|---|
| Nausea/vomiting | 7.3% | Similar |
| Diarrhea | 6.3% | Similar |
| Overall TEAEs | Mild/insignificant | -- |
Key characteristics:
- Lowest GI adverse event rates of any drug in this comparison by a wide margin
- 83% of all GI events classified as "insignificant"
- No clinically meaningful difference in GI events between NA-931 and placebo
- No muscle loss observed
- However, the study was only 13 weeks with 125 participants -- tolerability at higher doses and longer durations is unknown
Side-by-Side Comparison#
| Drug | Nausea | Vomiting | Diarrhea | AE Discontinuation | Weight Loss |
|---|---|---|---|---|---|
| Semaglutide 2.4 mg | 44% | 25% | 30% | 4.3% | 14.9% (68 wk) |
| Tirzepatide 15 mg | 31% | 12% | 23% | 6.2% | 20.9% (72 wk) |
| Retatrutide 12 mg | 43% | 21% | 33% | 18.2% | 28.7% (68 wk) |
| Orforglipron 36 mg | 34% | 14% | NR | 5.3-10.3% | 11.2% (72 wk) |
| Ecnoglutide 2.4 mg | Mild-mod | Mild-mod | Mild-mod | ~2% | 13.2% (40 wk) |
| CT-388 24 mg | Mild-mod (Ph2) | Mild-mod (Ph2) | Mild-mod (Ph2) | 5.9% | 22.5% (48 wk) |
| Bioglutide 150 mg | 7.3% | 7.3% | 6.3% | NR | 13.8% (13 wk) |
NR = not reported; Ph2 = Phase 2 data with aggregate descriptions rather than specific rates
Cross-trial comparison caveat: These rates come from different trials with different populations, titration schedules, treatment durations, and AE reporting conventions. They should be used for general comparison, not precise ranking.
Biased Agonism: Does It Work?#
The Evidence So Far#
Two drugs in this comparison -- ecnoglutide and CT-388 -- were specifically engineered with biased agonism to improve tolerability:
Ecnoglutide (cAMP-biased at GLP-1R):
- Discontinuation due to AEs: approximately 2%, among the lowest reported for any GLP-1 agonist
- Weight loss of 13.2% at 40 weeks is competitive with semaglutide-class efficacy
- The tolerability-to-efficacy ratio appears favorable
CT-388 (signal-biased at both GLP-1R and GIPR):
- Despite very high Phase 1b GI rates during titration (83% nausea), Phase 2 showed only 5.9% AE discontinuation
- Weight loss of 22.5% at 48 weeks is among the highest in the field
- The tolerability-to-efficacy ratio is notable: comparable weight loss to tirzepatide with a lower discontinuation rate
What the Data Suggest#
The biased agonism hypothesis appears to be supported by early clinical data, though with important caveats:
- Biased agonists do not eliminate GI side effects -- they may reduce their severity and duration
- The key metric is discontinuation, not incidence -- a drug with high nausea rates but low discontinuation may indicate transient, manageable symptoms
- Longer and larger trials are needed -- both ecnoglutide and CT-388 have limited Phase 3 data available
Patterns and Insights#
More Receptors, More Side Effects#
A general pattern emerges: adding receptor targets increases both efficacy and GI side effect burden.
| Targets | Example | Weight Loss | Nausea Rate |
|---|---|---|---|
| GLP-1 alone | Semaglutide | ~15% | 44% |
| GLP-1 + GIP | Tirzepatide | ~21% | 31% |
| GLP-1 + GIP + GCG | Retatrutide | ~29% | 43% |
The exception is tirzepatide, where adding GIP agonism actually lowered nausea rates compared to GLP-1 alone (31% vs 44%). This may reflect GIP's distinct receptor pharmacology or tirzepatide's specific molecular design. In contrast, adding glucagon agonism (retatrutide) pushed nausea back to semaglutide-like levels while adding the novel dysesthesia signal.
Oral vs Injectable Tolerability#
Orforglipron's GI profile (34% nausea at 36 mg) is broadly comparable to injectable GLP-1 agonists. This dispels the hypothesis that oral GLP-1 drugs might have worse GI tolerability due to direct gut exposure. The oral route of administration does not appear to be a significant independent driver of GI adverse events.
Bioglutide's dramatically low GI rates (7.3%) are noteworthy but must be interpreted cautiously given the short duration and small sample size.
The Discontinuation Hierarchy#
Discontinuation rates due to adverse events provide a practical measure of tolerability that matters most to patients:
- Best tolerated: Ecnoglutide (~2%), Bioglutide (NR but minimal)
- Well tolerated: Semaglutide (4.3%), CT-388 (5.9%), Tirzepatide (4.3-7.1%)
- Moderate: Orforglipron (5.3-10.3%)
- Higher burden: Retatrutide (12.2-18.2%)
Titration Matters#
GI side effects are strongly concentrated during dose escalation. All drugs show improvement during maintenance dosing:
- CT-388 nausea dropped from 83% (titration) to 54% (maintenance)
- Semaglutide and tirzepatide GI events are described as "transient" and occurring "primarily during dose escalation"
- Slower titration schedules generally reduce GI severity
This is clinically relevant: patients who tolerate the first 4-8 weeks of dose escalation will likely experience manageable side effects long-term.
Novel Safety Signals#
Dysesthesia (Retatrutide)#
The emergence of dysesthesia (abnormal touch sensation) in 8.8-20.9% of retatrutide-treated patients is the most notable novel signal in this comparison. This was not observed in Phase 2 and has not been reported with GLP-1 or GLP-1/GIP agonists. The glucagon receptor component is the most likely contributor. While these events did not appear to drive discontinuation, the 20.9% rate at the highest dose warrants close monitoring in the broader TRIUMPH program.
Dose-Dependent Risk#
Across all drugs, GI events and discontinuation rates increase with dose. For retatrutide, the 12 mg dose produced 28.7% weight loss but 18.2% discontinuation, while the 9 mg dose achieved 26.4% weight loss with 12.2% discontinuation. The marginal 2.3 percentage points of additional weight loss came at the cost of 6 percentage points higher discontinuation.
Managing GI Side Effects#
Regardless of the specific drug, several strategies can mitigate GI adverse events:
- Slow titration: Following or extending the recommended dose escalation schedule
- Dietary modification: Smaller meals, avoiding high-fat foods, eating slowly
- Timing: Taking the injection (or pill) at a consistent time, often in the evening
- Hydration: Maintaining adequate fluid intake to offset effects of reduced food intake
- Anti-emetics: Short-term use during dose escalation if needed
What to Watch#
- Ecnoglutide and CT-388 Phase 3 data -- Will the tolerability advantage of biased agonism hold in larger, longer trials?
- Retatrutide dysesthesia -- Will additional TRIUMPH readouts clarify the mechanism and reversibility?
- Head-to-head trials -- Direct comparisons (e.g., SURPASS-2 comparing tirzepatide to semaglutide) are needed for other drug pairs
- Real-world tolerability -- Trial populations may not reflect typical patients, who often have comorbidities and concomitant medications
Conclusion#
The GI side effect profile of GLP-1 drugs is not uniform. While nausea, vomiting, and diarrhea are class effects, their severity and clinical impact vary substantially across drugs. Semaglutide and tirzepatide have well-characterized, generally manageable GI profiles. Retatrutide's higher efficacy comes with correspondingly higher GI burden and a novel dysesthesia signal. Oral orforglipron matches injectable tolerability despite its different route.
The most intriguing development is the emergence of biased agonists. Ecnoglutide's approximately 2% AE discontinuation rate and CT-388's 5.9% rate despite 22.5% weight loss suggest that biased agonism may meaningfully improve the tolerability-efficacy equation. If Phase 3 data confirm these early signals, biased agonists could become the preferred approach for patients who struggle with GI side effects on current therapies.
This article is for educational and informational purposes only. It does not constitute medical advice.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Orforglipron Overview and Research Guide
- Orforglipron Dosing Protocols
- Orforglipron Side Effects and Safety
- Ecnoglutide Overview and Research Guide
- Ecnoglutide Dosing Protocols
- Ecnoglutide Side Effects and Safety
- CT-388 Overview and Research Guide
- CT-388 Dosing Protocols
- CT-388 Side Effects and Safety
- Bioglutide Overview and Research Guide
- Bioglutide Dosing Protocols
- Bioglutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About GLP-1 Side Effects Compared: Which Drug Is Best Tolerated?
What does this article cover?
A comprehensive comparison of GI side effects across GLP-1 drugs, from semaglutide and tirzepatide to next-generation biased agonists like ecnoglutide and CT-388 that may improve tolerability. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, Retatrutide, Orforglipron, Ecnoglutide, CT-388, Bioglutide. Key context: Semaglutide (FDA-approved GLP-1 benchmark with well-characterized GI side effect profile from STEP trials); Tirzepatide (Dual GLP-1/GIP agonist with GI rates from SURMOUNT trials showing dose-dependent tolerability); Retatrutide (Triple agonist with highest GI rates (43% nausea) plus novel dysesthesia signal in TRIUMPH-4). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "GLP-1 Side Effects Compared: Which Drug Is Best Tolerated?." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: FDA-approved GLP-1 benchmark with well-characterized GI side effect profile from STEP trials. Dual GLP-1/GIP agonist with GI rates from SURMOUNT trials showing dose-dependent tolerability. Triple agonist with highest GI rates (43% nausea) plus novel dysesthesia signal in TRIUMPH-4. These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: FDA-approved GLP-1 benchmark with well-characterized GI side effect profile from STEP trials. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Complete Guide to GLP-1 Receptor Agonists: Every Drug Explained
A comprehensive guide to every GLP-1 receptor agonist drug, from FDA-approved semaglutide and tirzepatide to pipeline therapies like retatrutide, amycretin, MariTide, and oral orforglipron.

GLP-1 Drugs Ranked by Weight Loss: 2026 Data Comparison
Every GLP-1 and incretin drug ranked by clinical weight loss data as of 2026, from retatrutide at 28.7% to oral orforglipron at 11.2%, with comparison tables and trial details.

How to Switch Between GLP-1 Medications: A Practical Guide
Practical guide for transitioning between GLP-1 medications including semaglutide, tirzepatide, and orforglipron, covering dose equivalences, timing, side effect management, and ATTAIN-MAINTAIN oral maintenance data.
You Might Also Like
Related content you may find interesting