Compounding Pharmacy Peptide Access: 2026 Regulatory Changes

Introduction#
The regulatory landscape for compounded peptides is undergoing significant changes in 2026. At the intersection of pharmaceutical regulation, patient access, drug pricing, and safety oversight, the rules governing peptide compounding affect millions of patients and billions of dollars in healthcare spending.
This article provides an overview of the current regulatory framework, recent FDA actions, and their practical impact on peptide access. The information is presented for educational purposes and reflects publicly available regulatory information as of early 2026.
Important: This article discusses regulatory and legal matters for informational purposes only. It does not constitute legal or medical advice. Patients should consult their healthcare providers and pharmacists about current medication availability.
Background: How Compounding Regulation Works#
The Legal Framework#
Pharmacy compounding in the United States is governed primarily by the Federal Food, Drug, and Cosmetic Act (FD&C Act), as amended by the Drug Quality and Security Act (DQSA) of 2013. Two sections define the two types of compounding pharmacies:
Section 503A (Traditional Compounding):
- Individual prescriptions for specific patients
- State-licensed pharmacies with pharmacist oversight
- Exempt from FDA premarket approval if certain conditions are met
- Cannot compound copies of commercially available drugs (with exceptions)
- Limited to state-level regulatory oversight
Section 503B (Outsourcing Facilities):
- Can compound without individual prescriptions
- Must register with the FDA and comply with current good manufacturing practices (cGMP)
- Subject to FDA inspection
- Can distribute across state lines
- Must report adverse events to the FDA
The Drug Shortage Exception#
A critical provision allows compounding of copies of commercially available drugs when those drugs are on the FDA's drug shortage list. This exception became central to the GLP-1 compounding debate when semaglutide and tirzepatide experienced supply shortages in 2023-2025, enabling compounding pharmacies to legally produce versions of these drugs at significantly lower prices.
The GLP-1 Compounding Controversy#
How It Started#
The GLP-1 compounding market grew rapidly in response to two converging forces:
- Supply shortages: Unprecedented demand for semaglutide (Wegovy/Ozempic) and tirzepatide (Mounjaro/Zepbound) led to persistent supply shortages, placing both drugs on the FDA shortage list
- Price disparity: Brand-name GLP-1 drugs cost $800-1,350 per month without insurance, while compounded versions were available for $150-500
This combination created a massive market for compounded GLP-1 medications, with estimates suggesting hundreds of compounding pharmacies and telehealth companies began offering compounded semaglutide and tirzepatide.
FDA Response#
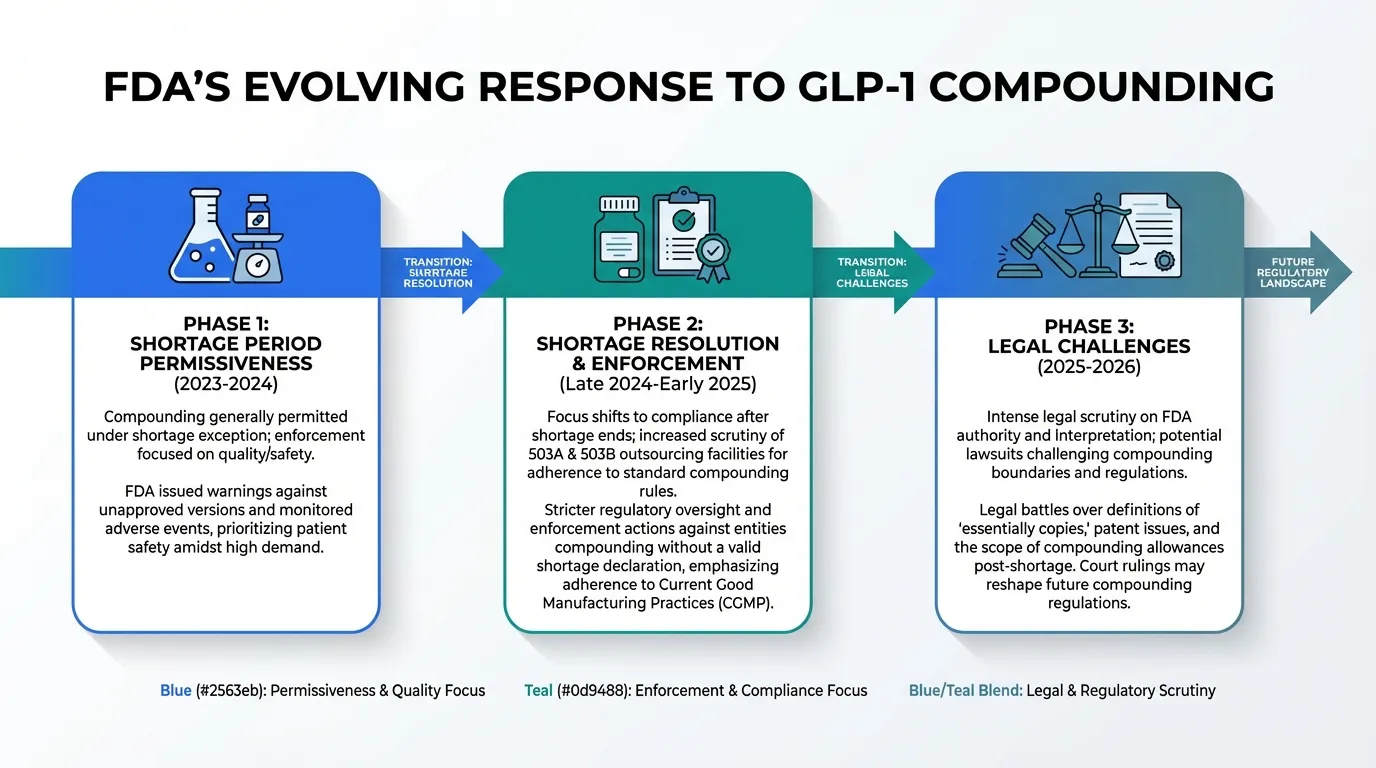
The FDA's approach to GLP-1 compounding has evolved through several stages:
Phase 1 -- Shortage period permissiveness: While drugs remained on the shortage list, compounding was generally permitted under the shortage exception. The FDA focused enforcement on quality and safety violations rather than the legality of compounding per se.
Phase 2 -- Shortage resolution and enforcement: As manufacturers increased supply and drugs came off the shortage list (or the FDA determined shortages were resolved), the legal basis for compounding weakened. The FDA issued communications to compounders regarding the changing shortage status.
Phase 3 -- Legal challenges: Compounding pharmacies, industry groups, and patient advocates filed legal challenges to FDA enforcement actions, arguing that compounding should continue based on ongoing access needs, salt form differences, or remaining supply constraints. These legal proceedings are ongoing.
The Salt Form Debate#
A technical but significant regulatory question centers on whether compounded versions constitute "copies" of the commercially available drug:
- Brand-name semaglutide uses semaglutide base
- Some compounders produce semaglutide sodium salt, arguing it is a different chemical form and therefore not a "copy"
- The FDA has contested this interpretation in some enforcement actions
- Court rulings on this question have varied by jurisdiction
This technical distinction has major practical implications for whether compounding can legally continue regardless of shortage status.
Beyond GLP-1: Research Peptide Compounding#
FDA Bulk Drug Substance Review#
The FDA's Pharmacy Compounding Advisory Committee (PCAC) evaluates bulk drug substances for their suitability for compounding. Substances are placed into categories:
- Category 1: Suitable for use in compounding under Section 503A or 503B
- Category 2: Raises safety or efficacy concerns that may make the substance unsuitable for compounding
- Category 3: Under evaluation; additional data needed
Peptides Affected#
Several research peptides have been subject to FDA scrutiny through this process:
BPC-157: Has been discussed in the context of FDA bulk drug substance nominations. BPC-157 is not an FDA-approved drug and has no completed human clinical trials, which raises questions about its suitability for compounding under the established framework. See our BPC-157 FDA status article for detailed coverage.
Thymosin Alpha-1: Has a more complex regulatory history. While it is approved as a drug in some countries (though not the US), its status for compounding purposes has been subject to regulatory review.
Other peptides: Various other research peptides used in compounding have been or are being evaluated, including some growth hormone secretagogues and healing peptides.
Impact on Patient Access#
FDA regulatory actions on non-GLP-1 peptides have had cascading effects:
- Some compounding pharmacies have discontinued peptide products voluntarily to avoid regulatory risk
- Prices for remaining compounded peptides have increased as supply decreases
- Patients who were using compounded peptides for therapeutic purposes have faced disruption
- The research peptide marketplace has shifted as some products move from compounding pharmacies to research chemical suppliers operating under different regulatory frameworks
The 503B Outsourcing Facility Landscape#
Increased Scrutiny#
503B outsourcing facilities, which can produce larger batches of compounded medications, have faced increased FDA attention:
- Inspection frequency: The FDA has increased inspection frequency for 503B facilities producing GLP-1 compounds
- cGMP enforcement: Several facilities have received warning letters or Form 483 observations for manufacturing practice deficiencies
- Sterility concerns: Injectable peptide compounding requires stringent sterile manufacturing conditions that not all facilities consistently maintain
- Potency verification: Ensuring compounded peptides contain the labeled amount of active ingredient has been an enforcement focus
Quality Considerations#
The compounding quality debate has two sides:
Concerns:
- Variable potency between and within batches
- Sterility assurance challenges, particularly for injectable formulations
- Limited stability testing compared to brand-name manufacturers
- No FDA premarket review of safety and efficacy
- Reports of adverse events from compounded products
Counterarguments:
- Well-run 503B facilities follow cGMP standards comparable to traditional manufacturers
- Third-party testing can verify potency and sterility
- Access to affordable medications is a public health imperative
- Brand-name manufacturers have also had quality issues and recalls
Congressional and Legal Developments#
Legislative Actions#
Several legislative efforts have addressed peptide compounding access:
- Compounding access proposals: Bills introduced to protect patient access to compounded medications when brand-name drugs are unaffordable
- Drug pricing reform: Broader drug pricing legislation that could reduce the price differential driving compounding demand
- FDA oversight modifications: Proposals to clarify FDA authority over compounding in specific circumstances
Legal Challenges#
The legal landscape includes:
- Industry lawsuits against FDA: Compounding pharmacy trade groups have challenged specific FDA enforcement actions and interpretations of the shortage exception
- State-level actions: Some states have enacted or proposed legislation to protect in-state compounding pharmacies
- Constitutional questions: Some legal challenges raise questions about FDA authority and interstate commerce regulation of pharmacy practice
What Patients Should Know#
Practical Guidance#
For patients currently using or considering compounded peptides:
- Verify pharmacy credentials: Confirm that your compounding pharmacy is properly licensed and, if a 503B, registered with the FDA
- Ask about testing: Request certificates of analysis (COA) showing potency, sterility, and endotoxin testing results
- Stay informed: Regulatory changes can affect availability with little notice; maintain awareness of your medication's compounding status
- Have contingency plans: If using compounded GLP-1 medications, discuss brand-name alternatives and insurance options with your prescriber in case compounding is restricted
- Report adverse events: Report any adverse events from compounded products to your pharmacy, prescriber, and the FDA MedWatch program
For Healthcare Providers#
Prescribers navigating the compounding landscape should consider:
- Prescribing authority: Ensure prescriptions for compounded peptides comply with federal and state regulations
- Patient counseling: Discuss the regulatory uncertainty with patients who rely on compounded medications
- Quality verification: Develop relationships with reputable compounding pharmacies that provide documentation of quality testing
- Insurance alternatives: Stay current on insurance coverage options and manufacturer assistance programs that may provide brand-name drugs at comparable costs to compounded versions
Looking Ahead#
Trends to Watch in 2026#
Several developments will shape the compounding landscape over the coming months:
- Court decisions: Pending legal cases could clarify the scope of FDA authority over peptide compounding
- Shortage list updates: Changes to the FDA drug shortage list directly affect compounding legality for specific products
- Congressional action: Legislation on both compounding access and drug pricing could shift the landscape
- New drug approvals: Approval of additional GLP-1 class drugs could increase competition and reduce brand-name pricing, potentially reducing compounding demand
- FDA guidance documents: New FDA guidance on compounding of specific product categories could provide clearer regulatory boundaries
Key Takeaways#
-
Peptide compounding regulation is in flux. The rules governing what can be compounded, by whom, and under what circumstances are actively being contested in courts, Congress, and by the FDA.
-
GLP-1 compounding is the highest-profile battleground. The combination of high drug prices, massive demand, and supply constraints has created a complex regulatory situation with significant financial stakes.
-
Non-GLP-1 research peptides face separate challenges. The FDA's bulk drug substance review process is evaluating the compounding suitability of various peptides, with some facing restrictions.
-
Quality is a legitimate concern. Not all compounding pharmacies maintain equivalent quality standards, and patients should verify pharmacy credentials and request testing documentation.
-
Patient access hangs in the balance. The outcome of regulatory and legal proceedings will determine whether millions of patients continue to have access to affordable compounded peptide medications.
This article is for informational purposes only and does not constitute legal or medical advice. Regulatory information reflects publicly available data as of early 2026 and is subject to change. Consult a healthcare provider and pharmacist for current medication availability and legal compliance.
Related Articles#

{kind=link}
Frequently Asked Questions About Compounding Pharmacy Peptide Access: 2026 Regulatory Changes
Can compounding pharmacies still make semaglutide in 2026?
The situation is complex and evolving. Under the FD&C Act, pharmacies can compound drugs that are on the FDA drug shortage list. Semaglutide's shortage status has fluctuated, and FDA enforcement actions have targeted some compounders. Legal challenges and congressional actions have added further complexity. Patients should verify current availability with their compounding pharmacy and prescriber, as the situation may change at any time.
What is the difference between a 503A and 503B pharmacy?
503A pharmacies are traditional compounding pharmacies that prepare medications based on individual prescriptions for specific patients. 503B pharmacies are outsourcing facilities that can compound larger batches without individual prescriptions, operating under more stringent FDA oversight including current good manufacturing practice (cGMP) requirements and regular FDA inspections. Both can compound peptides under different regulatory frameworks.
Which peptides has the FDA restricted from compounding?
The FDA maintains a list of bulk drug substances evaluated for compounding eligibility. Some peptides have been placed in Category 2, meaning the FDA has raised concerns about their suitability for compounding. Specific peptides affected include some research peptides like BPC-157. The regulatory status of each peptide can change based on FDA review processes, and the list is periodically updated.
How do FDA compounding regulations affect peptide pricing?
FDA regulatory actions directly impact pricing by affecting supply. When compounding is restricted for a peptide, patients must use brand-name versions at significantly higher prices. For example, compounded semaglutide has historically cost $150-400 per month compared to over $1,300 for brand-name Wegovy. Regulatory uncertainty itself also affects pricing as compounders may raise prices to account for compliance costs and legal risks.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

FDA Peptide Regulation in 2026: What Is Banned and What Is Legal
FDA peptide regulation in 2026: which peptides are banned from compounding, which remain legal, and what the changes mean for researchers.

Peptide Interactions with Medications: What Your Doctor Needs to Know
Critical reference guide on peptide-drug interactions for healthcare professionals and patients. Covers GLP-1 delayed gastric emptying effects on oral medications, GH peptide interactions with diabetes and thyroid medications, immune peptide conflicts with immunosuppressants, and key information gaps.

What Peptides Are FDA Approved? The Complete List (2026)
Complete list of FDA-approved peptide drugs with brand names, indications, and approval dates. Updated March 2026 with the RFK Jr. Category 1 reclassification of 14 peptides for compounding pharmacy access.
You Might Also Like
Related content you may find interesting