GLP-1 Drug Cost Comparison 2026: Insurance, Cash, and Compounded Pricing

Introduction#
The cost of GLP-1 receptor agonist medications remains one of the biggest barriers to access for the millions of people who could benefit from these treatments. In 2026, the GLP-1 pricing landscape is more complex than ever, with brand-name drugs, compounded alternatives, and a rapidly changing insurance environment all influencing what patients actually pay.
This guide breaks down the current pricing for major GLP-1 medications, compares brand-name versus compounded options, and outlines practical strategies for reducing out-of-pocket costs. All prices reflect publicly available data as of early 2026 and may vary by pharmacy, region, and insurance plan.
Important: This article covers pricing information for educational purposes. It does not constitute financial or medical advice. Always verify current pricing with your pharmacy and insurance provider.
Brand-Name GLP-1 Pricing Overview#
Current List Prices#
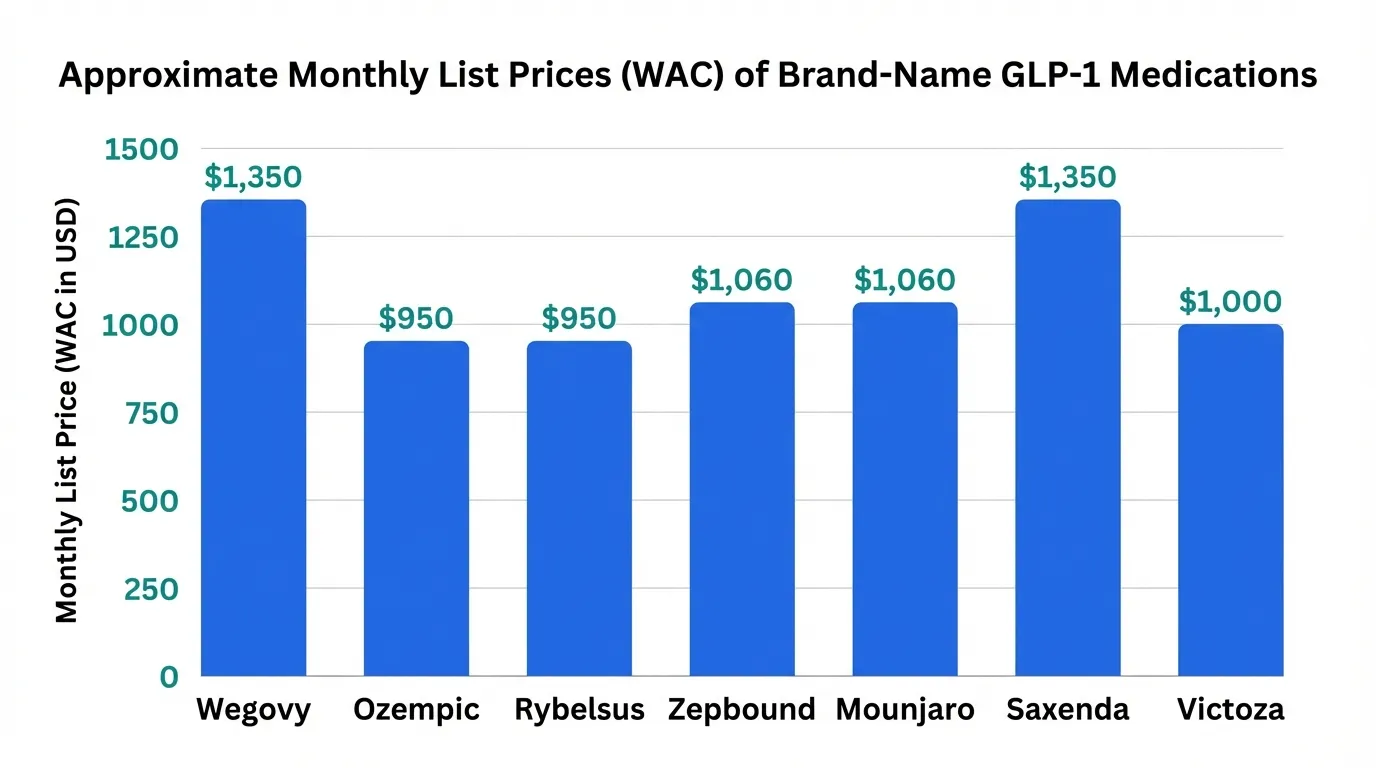
The wholesale acquisition cost (WAC) -- often called the "list price" -- for brand-name GLP-1 medications provides a baseline for understanding the pricing landscape, though few patients pay these amounts directly.
| Medication | Brand Name | Indication | Monthly List Price (approx.) | Manufacturer |
|---|---|---|---|---|
| Semaglutide 2.4 mg | Wegovy | Weight management | $1,349 | Novo Nordisk |
| Semaglutide 1.0 mg | Ozempic | Type 2 diabetes | $968 | Novo Nordisk |
| Semaglutide oral 14 mg | Rybelsus | Type 2 diabetes | $936 | Novo Nordisk |
| Tirzepatide (weight) | Zepbound | Weight management | $1,059 | Eli Lilly |
| Tirzepatide (diabetes) | Mounjaro | Type 2 diabetes | $1,023 | Eli Lilly |
| Liraglutide 3.0 mg | Saxenda | Weight management | $1,385 | Novo Nordisk |
| Liraglutide 1.8 mg | Victoza | Type 2 diabetes | $1,032 | Novo Nordisk |
Key observation: Eli Lilly's tirzepatide (Zepbound) entered the market at a notably lower list price than Novo Nordisk's semaglutide (Wegovy), positioning itself as the more competitively priced option among newer-generation GLP-1 drugs. Lilly also launched a direct-to-consumer program offering Zepbound vials at reduced prices for patients without insurance coverage.
What Patients Actually Pay#
List prices rarely reflect actual out-of-pocket costs. The real price depends on several layers of negotiation:
- With commercial insurance and copay card: $0-25 per month (both Novo Nordisk and Eli Lilly offer manufacturer copay assistance programs)
- With commercial insurance, no copay card: $50-300 per month (varies by formulary tier and plan design)
- Medicare Part D (2026): Variable copay depending on plan; the Inflation Reduction Act's $2,000 annual out-of-pocket cap applies
- Cash price without insurance: $800-1,350 per month at retail pharmacies
- Cash price with GoodRx or similar: $750-1,200 per month
Compounded GLP-1 Pricing#
The Compounded Alternative#
Compounding pharmacies have offered semaglutide and tirzepatide at substantially lower prices than brand-name versions. These compounded products are made by 503A (patient-specific) or 503B (outsourcing facility) pharmacies under FDA oversight, though they are not FDA-approved products.
| Compounded Product | Typical Monthly Cost | Source Type |
|---|---|---|
| Compounded semaglutide (injection) | $150-400 | 503A/503B pharmacy |
| Compounded semaglutide (sublingual) | $100-300 | 503A pharmacy |
| Compounded tirzepatide (injection) | $200-500 | 503A/503B pharmacy |
Regulatory Uncertainty#
The compounded GLP-1 market faces significant regulatory uncertainty in 2026. The FDA's position on compounding these medications has evolved:
- Compounding of a drug is permitted under Section 503A of the FD&C Act when the brand-name drug is on the FDA's drug shortage list
- Semaglutide and tirzepatide have experienced supply constraints, which temporarily enabled compounding
- As supply stabilizes, the FDA has signaled potential restrictions on compounded versions
- Several legal challenges and congressional actions have complicated the regulatory picture
Patients relying on compounded GLP-1 medications should be aware that availability could change based on regulatory decisions. See our compounding pharmacy regulatory guide for detailed coverage of the 2026 landscape. For a focused breakdown of compounded semaglutide pricing, eligibility, and pharmacy selection, see our Compounded Semaglutide Cost Guide 2026.
Insurance Coverage Landscape#
Commercial Insurance#
Coverage for GLP-1 weight management drugs has expanded significantly since 2023:
- Tier placement: Most commercial plans now include at least one GLP-1 for weight management, typically on Tier 3 (preferred brand) or Tier 4 (non-preferred brand)
- Prior authorization: Nearly universal, typically requiring documented BMI of 30+ (or 27+ with comorbidity), evidence of failed lifestyle interventions, and sometimes a step-therapy requirement
- Step therapy: Some plans require trying liraglutide (Saxenda) before approving semaglutide or tirzepatide for weight management
- Quantity limits: Most plans align with FDA-approved dosing schedules
Medicare Coverage#
The landscape for Medicare coverage of anti-obesity medications shifted in 2026:
- The TREAT Act provisions expanded Medicare Part D coverage to include FDA-approved anti-obesity medications
- Coverage applies to drugs with FDA-approved weight management indications (Wegovy, Zepbound, Saxenda)
- Standard Part D cost-sharing applies, with the $2,000 annual out-of-pocket cap providing meaningful protection
- Medicare Advantage plans may offer additional coverage through supplemental benefits
Medicaid Coverage#
Medicaid coverage remains inconsistent across states:
- Some states cover GLP-1 medications for weight management under their Medicaid formularies
- Others cover only for the diabetes indication
- Coverage criteria, preferred agents, and prior authorization requirements vary significantly by state
- Managed Medicaid plans may have different formulary decisions than fee-for-service Medicaid
Cost-Saving Strategies#
Manufacturer Programs#
Both major GLP-1 manufacturers offer significant savings programs:
Novo Nordisk (Wegovy/Ozempic):
- Savings card for commercially insured patients (may reduce copay to $0-25)
- Patient assistance program (Novo Nordisk PAP) for uninsured patients meeting income criteria
- Savings offer for cash-paying patients
Eli Lilly (Zepbound/Mounjaro):
- Commercial copay savings card
- Lilly direct-to-consumer vial program for Zepbound at reduced cash prices
- Solutions Center for insurance navigation support
- Patient assistance for qualifying uninsured patients
Pharmacy Shopping#
Prices can vary substantially between pharmacies:
- Retail chain pharmacies: Typically charge the highest cash prices
- Independent pharmacies: May offer competitive pricing, especially for compounded products
- Mail-order pharmacies: Often provide 90-day supplies at lower per-month costs
- Specialty pharmacies: Required by some insurers; pricing varies
- Discount programs: GoodRx, RxSaver, and similar platforms can identify lower-cost pharmacy options
Dosing Considerations#
For patients managing costs, dosing strategy matters:
- Maintenance dose optimization: Some patients achieve adequate weight management on lower doses (e.g., semaglutide 1.7 mg instead of 2.4 mg), which reduces cost
- Diabetes vs. weight indication: The same active ingredient may be available at different prices depending on the indication and brand name
- Pen sharing (not recommended): While some patients consider sharing multi-dose pens, this practice carries infection risk and dosing inaccuracy and is not endorsed by manufacturers or medical guidelines
Pipeline Drugs and Future Pricing#
What Is Coming#
Several investigational GLP-1 class drugs could reshape pricing dynamics:
- Retatrutide: Eli Lilly's triple agonist in Phase 3 trials. Pricing has not been announced, but Lilly's track record with Zepbound suggests competitive positioning
- Survodutide: Boehringer Ingelheim's dual GLP-1/glucagon agonist. Expected to enter a market with established pricing benchmarks
- Orforglipron: Eli Lilly's oral GLP-1 agonist, which could disrupt pricing by eliminating injection costs and cold-chain requirements
- Generic competition: No generic semaglutide or tirzepatide is expected before patent expiration dates (estimated late 2020s to early 2030s for key patents)
Pricing Pressure Factors#
Several forces are pushing GLP-1 prices downward:
- Competition: More drugs in the class means more formulary negotiation leverage for insurers
- Political pressure: Congressional scrutiny of obesity drug pricing continues
- Scale: Manufacturing capacity expansion should reduce per-unit production costs
- International reference pricing: Growing awareness of lower prices in other countries adds pressure
- Oral formulations: If orforglipron is approved, its lower manufacturing cost could set new pricing expectations
Cost Comparison by Scenario#
Monthly Cost Estimates by Patient Situation#
| Scenario | Semaglutide (Wegovy) | Tirzepatide (Zepbound) | Liraglutide (Saxenda) | Compounded Semaglutide |
|---|---|---|---|---|
| Commercial insurance + copay card | $0-25 | $0-25 | $0-25 | N/A |
| Commercial insurance, no copay card | $100-300 | $75-250 | $100-300 | N/A |
| Medicare Part D | $100-400* | $100-400* | $100-350* | N/A |
| Cash pay (retail) | $1,200-1,350 | $1,000-1,060 | $1,100-1,385 | N/A |
| Cash pay (compounded) | N/A | N/A | N/A | $150-400 |
*Medicare costs subject to plan design, deductible status, and $2,000 annual OOP cap.
Key Takeaways#
-
List prices do not reflect reality for most patients. Manufacturer programs, insurance negotiations, and pharmacy selection create a wide range of actual costs, from $0 to over $1,300 per month for the same medication.
-
Insurance coverage is expanding but uneven. Commercial plans increasingly cover GLP-1 weight management drugs, Medicare Part D coverage expanded in 2026, but Medicaid remains inconsistent by state.
-
Compounded GLP-1 medications offer the lowest cash prices but face regulatory uncertainty. Patients using compounded products should stay informed about FDA regulatory actions and have contingency plans.
-
Tirzepatide (Zepbound) is priced below semaglutide (Wegovy) at list price, and Eli Lilly has been more aggressive with direct-to-consumer savings programs.
-
The pipeline offers hope for lower prices. Increased competition from retatrutide, survodutide, oral formulations, and eventual generic entry should create downward pricing pressure over the coming years.
-
Talk to your healthcare provider and insurance company. The optimal drug from a cost perspective depends entirely on individual insurance coverage, available copay programs, and clinical factors.
This article is for informational purposes only and does not constitute medical or financial advice. Drug prices change frequently. Always verify current pricing with your pharmacy and insurance provider. For medical information about GLP-1 medications, see our peptide profiles and consult a healthcare professional.
Related Articles#

{kind=link}
Frequently Asked Questions About GLP-1 Drug Cost Comparison 2026: Insurance, Cash, and Compounded Pricing
How much does Wegovy cost without insurance in 2026?
The list price for Wegovy (semaglutide 2.4 mg) is approximately $1,350 per month without insurance. However, actual out-of-pocket costs vary significantly depending on pharmacy, manufacturer savings programs, and whether compounded alternatives are available. Some patients pay as little as $0-25 per month with commercial insurance and manufacturer copay cards.
Is compounded semaglutide cheaper than brand-name Wegovy?
Compounded semaglutide has historically been significantly cheaper, typically ranging from $150-400 per month compared to over $1,300 for brand-name Wegovy. However, the FDA has been tightening regulations on compounded versions of GLP-1 drugs, and availability may be affected by ongoing regulatory changes in 2026.
Does insurance cover GLP-1 medications for weight loss?
Coverage varies widely by insurer and plan. Many commercial insurance plans now cover Wegovy and Zepbound for weight management, though prior authorization is typically required. Medicare Part D began covering anti-obesity medications in 2026 following the TREAT Act provisions. Medicaid coverage varies by state. Patients should verify coverage with their specific plan.
Which GLP-1 drug is the most affordable option?
Liraglutide (Saxenda) is generally the least expensive brand-name GLP-1 for weight loss due to its longer market presence. Compounded semaglutide, where available, has been the most affordable GLP-1 option overall. Manufacturer savings programs and insurance negotiation can significantly reduce costs for any GLP-1 medication.
Will GLP-1 drug prices decrease in 2026?
Several factors are creating downward pricing pressure on GLP-1 drugs in 2026, including increased competition from new entrants like retatrutide, expanded insurance coverage mandates, manufacturer savings programs, and ongoing discussion of drug pricing reform. However, list prices for brand-name drugs have remained high, and actual price reductions depend heavily on insurance and pharmacy benefit manager negotiations.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.

Retatrutide Canada Guide
Retatrutide in Canada: Everything You Need to Know — part of the Next-Gen Weight Loss content cluster.
Liraglutide Side Effects: 2026 Mid-Year Update
A mid-2026 review of liraglutide (Saxenda, Victoza) side effects covering GI tolerability, cardiovascular safety from LEADER, long-term post-marketing signals, and how the profile compares to semaglutide, tirzepatide, and retatrutide.
You Might Also Like
Related content you may find interesting