Retatrutide Phase 3 Results 2026: TRIUMPH Trial Weight Loss Data

Introduction#
Retatrutide (LY3437943) is the first triple receptor agonist -- targeting GIP, GLP-1, and glucagon receptors simultaneously -- to produce Phase 3 clinical trial results. Developed by Eli Lilly, it delivered the highest weight loss ever recorded in a Phase 3 obesity trial when TRIUMPH-4 results were reported in December 2025.
The TRIUMPH clinical trial program encompasses eight Phase 3 studies across obesity, type 2 diabetes, obstructive sleep apnea, knee osteoarthritis, chronic low back pain, MASLD/MASH, and cardiometabolic outcomes. This article reviews the available Phase 3 data from TRIUMPH-4, analyzes the safety profile including the new dysesthesia signal, and compares retatrutide with approved therapies like semaglutide and tirzepatide.
Important: Retatrutide is an investigational drug. It is NOT FDA-approved for any indication. All data discussed comes from clinical trials and regulatory filings. This article does not constitute medical advice or a recommendation to seek access to this compound.
TL;DR: Retatrutide Phase 3 Weight Loss by Dose#
The following summary reflects TRIUMPH-4 Phase 3 data at 48 and 68 weeks. The 48-week column captures the on-treatment trajectory partway through the trial; the 68-week column is the primary endpoint readout.
| Dose | Weight Loss % (48 weeks) | Weight Loss % (68 weeks) | Key Finding |
|---|---|---|---|
| Placebo | ~-1.5% | -2.1% | Minimal change; standard lifestyle counseling only |
| Retatrutide 9 mg | ~-22% | -26.4% (-64.2 lbs) | Strong efficacy with dysesthesia rate under 10% |
| Retatrutide 12 mg | ~-24% | -28.7% (-71.2 lbs) | Highest Phase 3 obesity weight loss ever recorded; ~40% of patients lost 30%+ |
Source: TRIUMPH-4 topline results (Eli Lilly, December 2025). The 48-week figures are interim-trajectory estimates and should be verified against Lilly's full published data release. See the full efficacy breakdown below.
Latest Updates (April 2026)#
- April 2026: Updated post-hoc analyses of TRIUMPH-4 have provided additional granularity on the nausea incidence pattern across dose-escalation and maintenance phases. See the April 2026 TRIUMPH-4 Nausea Incidence section below for details.
- March 2026: The TRIUMPH program design paper by Giblin et al. has been published in Diabetes, Obesity and Metabolism (PMID: 41090431), providing full details on the four-study registrational program evaluating retatrutide across obesity, OSA, and knee OA indications with over 5,800 participants enrolled.
- December 2025: TRIUMPH-4 topline results announced -- retatrutide 12 mg achieved 28.7% mean weight loss at 68 weeks in adults with obesity and knee osteoarthritis, the highest weight loss ever reported in a Phase 3 obesity trial.
- Upcoming in 2026: Seven additional TRIUMPH Phase 3 readouts are expected, including the 80-week TRIUMPH-1 trial (general obesity without diabetes), TRIUMPH-2 (obesity with type 2 diabetes), TRIUMPH-3 (obesity with cardiovascular disease), and trials in MASLD/MASH and chronic low back pain. Analysts project TRIUMPH-1 could show weight loss exceeding 30% due to the longer treatment duration.
- NDA filing: Eli Lilly is expected to submit a New Drug Application in late 2026 or early 2027 once the full Phase 3 data package is analyzed. If granted priority review, FDA approval could come as early as mid-2027.
The Triple Agonist Mechanism#
Why Three Receptors?#
Retatrutide's design builds on the incremental receptor-addition strategy that has defined the obesity drug pipeline:
- GLP-1 receptor agonism: Suppresses appetite via hypothalamic signaling, slows gastric emptying, improves insulin secretion (the foundation established by semaglutide)
- GIP receptor agonism: Enhances insulin sensitivity, may improve fat metabolism, and appears to modulate the GI tolerability of GLP-1 agonism (the addition made by tirzepatide)
- Glucagon receptor agonism: Increases energy expenditure through hepatic fat oxidation, promotes thermogenesis, and may contribute to liver fat reduction (the novel addition in retatrutide)
The hypothesis behind triple agonism is that activating all three receptor pathways simultaneously produces additive or synergistic weight loss effects that exceed what any one or two receptors can achieve. The TRIUMPH-4 data confirm this hypothesis with the largest weight loss ever observed in a Phase 3 obesity trial.
TRIUMPH Phase 3 Program Overview#
The TRIUMPH program, described in detail by Giblin et al. (2026) in Diabetes, Obesity and Metabolism, consists of eight Phase 3 trials enrolling over 5,800 participants across multiple indications:
| Trial | Population | Duration | Status (as of March 2026) |
|---|---|---|---|
| TRIUMPH-1 | Adults with obesity (weight management basket + OSA/OA nested) | 80 weeks | Ongoing; readout expected 2026 |
| TRIUMPH-2 | Adults with obesity (weight management basket + OSA/OA nested) | ~68-80 weeks | Ongoing; readout expected 2026 |
| TRIUMPH-3 | Adults with obesity and cardiovascular disease | ~68-80 weeks | Ongoing; readout expected 2026 |
| TRIUMPH-4 | Adults with obesity and knee osteoarthritis | 68 weeks | Results reported December 2025 |
| Additional trials | Type 2 diabetes, chronic low back pain, MASLD/MASH, cardiometabolic outcomes | Varies | Enrolling/ongoing; readouts expected 2026 |
All four primary TRIUMPH trials test retatrutide 9 mg and 12 mg doses versus placebo, with some trials also evaluating a 4 mg maintenance dose. All participants undergo dose escalation starting at 2 mg weekly, increasing every 4 weeks until reaching the target dose.
TRIUMPH-4 Results: Record-Setting Weight Loss#
Trial Design#
TRIUMPH-4 (NCT05931367) enrolled 445 adults with obesity (BMI 30+ or BMI 27+ with comorbidity) and knee osteoarthritis, without type 2 diabetes. Participants were randomized 1:1:1 to retatrutide 9 mg, retatrutide 12 mg, or placebo for 68 weeks. The trial had co-primary endpoints: percent change in body weight and change in WOMAC pain subscale score. The average baseline weight was 112.7 kg (248.5 lbs), and 84% of participants had a BMI of 35 or greater.
Weight Loss Results#
| Endpoint | Retatrutide 9 mg | Retatrutide 12 mg | Placebo |
|---|---|---|---|
| Mean body weight change | -26.4% (-29.1 kg / -64.2 lbs) | -28.7% (-32.3 kg / -71.2 lbs) | -2.1% (-2.1 kg / -4.6 lbs) |
| Patients achieving 25%+ loss | 47.7% | 58.6% | 1.3% |
| Patients achieving 30%+ loss | 30.5% | 39.4% | 0.8% |
| Patients achieving 35%+ loss | 18.2% | 23.7% | 0.0% |
These results represent the highest weight loss ever reported in a Phase 3 obesity trial. Nearly 4 in 10 patients on the 12 mg dose lost 30% or more of their body weight -- a threshold previously achievable only through bariatric surgery.
Knee Osteoarthritis Pain Outcomes#
A notable feature of TRIUMPH-4 was the co-primary endpoint of knee OA pain reduction, measured by WOMAC pain subscale:
| Endpoint | Retatrutide 9 mg | Retatrutide 12 mg | Placebo |
|---|---|---|---|
| WOMAC pain change | -4.5 points (-75.8%) | -4.4 points (-74.3%) | -2.4 points (-40.3%) |
| WOMAC physical function change | -4.1 points (-71.8%) | -4.2 points (-73.7%) | -- |
| Completely pain-free at 68 weeks | 14.1% | 12.0% | 4.2% |
The substantial pain reduction suggests that retatrutide's magnitude of weight loss translates into clinically meaningful improvements in obesity-related comorbidities -- a finding that strengthens the case for its therapeutic value beyond weight loss alone.
Cardiovascular and Metabolic Markers#
Retatrutide also demonstrated improvements in cardiometabolic risk factors at the 12 mg dose:
- Systolic blood pressure reduction of 14.0 mmHg
- Reductions in non-HDL cholesterol
- Reductions in triglycerides
- Reductions in high-sensitivity C-reactive protein (hs-CRP)
These findings are consistent with the metabolic benefits observed with other incretin-based therapies, though dedicated cardiovascular outcomes data from the TRIUMPH program are still pending.
Safety Profile: What the Data Show#
Gastrointestinal Adverse Events#
As with all incretin-based therapies, GI side effects were the most common adverse events in TRIUMPH-4:
| Adverse Event | Retatrutide 9 mg | Retatrutide 12 mg | Placebo |
|---|---|---|---|
| Nausea | 38.1% | 43.2% | 10.7% |
| Diarrhea | 34.7% | 33.1% | 13.4% |
| Constipation | 21.8% | 25.0% | 8.7% |
| Vomiting | 20.4% | 20.9% | 0.0% |
| Decreased appetite | 19.0% | 18.2% | 9.4% |
These rates are higher than those reported for semaglutide and tirzepatide in their respective Phase 3 trials, which is expected given the additional receptor activity and greater weight loss magnitude.
April 2026 Update: TRIUMPH-4 Nausea Incidence#
Post-hoc analyses and conference presentations in early 2026 have provided additional granularity on the TRIUMPH-4 nausea signal that was only summarized at the top line in December 2025.
Across the TRIUMPH-4 trial, nausea incidence in the retatrutide arms was concentrated during the dose-escalation phase (weeks 0-20) and declined sharply through the maintenance phase. Peak weekly incidence at the 12 mg dose was reported in the dose-escalation window, with substantially lower rates during maintenance dosing. The latest analyses suggest that the majority of nausea events were mild-to-moderate, with severe events occurring in a smaller subset of patients.
Clinical implications of the updated nausea data:
- Dose escalation matters: The concentration of nausea events in the escalation phase supports a conservative titration approach (the standard 4-week dose steps), with consideration of a slower schedule for sensitive patients.
- Tolerability improves over time: The declining nausea incidence from escalation to maintenance is consistent with what has been seen with semaglutide and tirzepatide, suggesting retatrutide's GI profile follows the same adaptive pattern despite higher absolute rates.
- The 9 mg dose advantage: Combined with the much lower dysesthesia rate at 9 mg (8.8% vs 20.9%), the more manageable nausea profile strengthens the case that 9 mg may become the preferred clinical dose if retatrutide is approved.
These observations are subject to revision as the full TRIUMPH-4 manuscript and subsequent TRIUMPH readouts are published. Readers should consult the primary literature for definitive figures.
Dysesthesia: A Novel Safety Signal#
The most notable safety finding from TRIUMPH-4 was the emergence of dysesthesia -- abnormal or unpleasant touch sensations -- as a dose-dependent adverse event:
- 9 mg dose: 8.8% incidence
- 12 mg dose: 20.9% incidence
- Placebo: 0.7%
This signal was not observed in the earlier Phase 2 trial and has not been reported with GLP-1 or GLP-1/GIP agonists. Two leading hypotheses have been proposed: GLP-1 receptor activity on peripheral nerves, and effects on small blood vessels supplying sensory nerves, with the glucagon receptor component potentially contributing.
According to Eli Lilly, dysesthesia events were generally mild and did not appear to be a primary driver of treatment discontinuation. However, the 20.9% rate at the highest dose is clinically significant and will require further characterization in the remaining TRIUMPH readouts.
Discontinuation Rates#
Treatment discontinuation due to adverse events was dose-dependent:
| Group | Discontinuation Due to AEs |
|---|---|
| Retatrutide 9 mg | 12.2% |
| Retatrutide 12 mg | 18.2% |
| Placebo | 4.0% |
Notably, discontinuation rates were lower among participants with higher baseline BMI (35+): 8.8% at 9 mg and 12.1% at 12 mg in this subgroup. This suggests that higher-BMI patients may tolerate retatrutide better, possibly because the benefit-risk ratio is more favorable for those with more severe obesity.
The 18.2% discontinuation rate at 12 mg is substantially higher than semaglutide (7.0% in STEP 1) or tirzepatide (6.2% at 15 mg in SURMOUNT-1). Some discontinuations were reportedly due to patients perceiving "excessive weight loss" -- an unusual reason for dropout in obesity trials.
Retatrutide vs Tirzepatide vs Semaglutide#
While no head-to-head trials have been conducted, cross-trial comparisons provide context for how retatrutide performs relative to approved therapies. These comparisons have inherent limitations (different populations, protocols, and baseline characteristics) and should be interpreted with caution.
Efficacy Comparison#
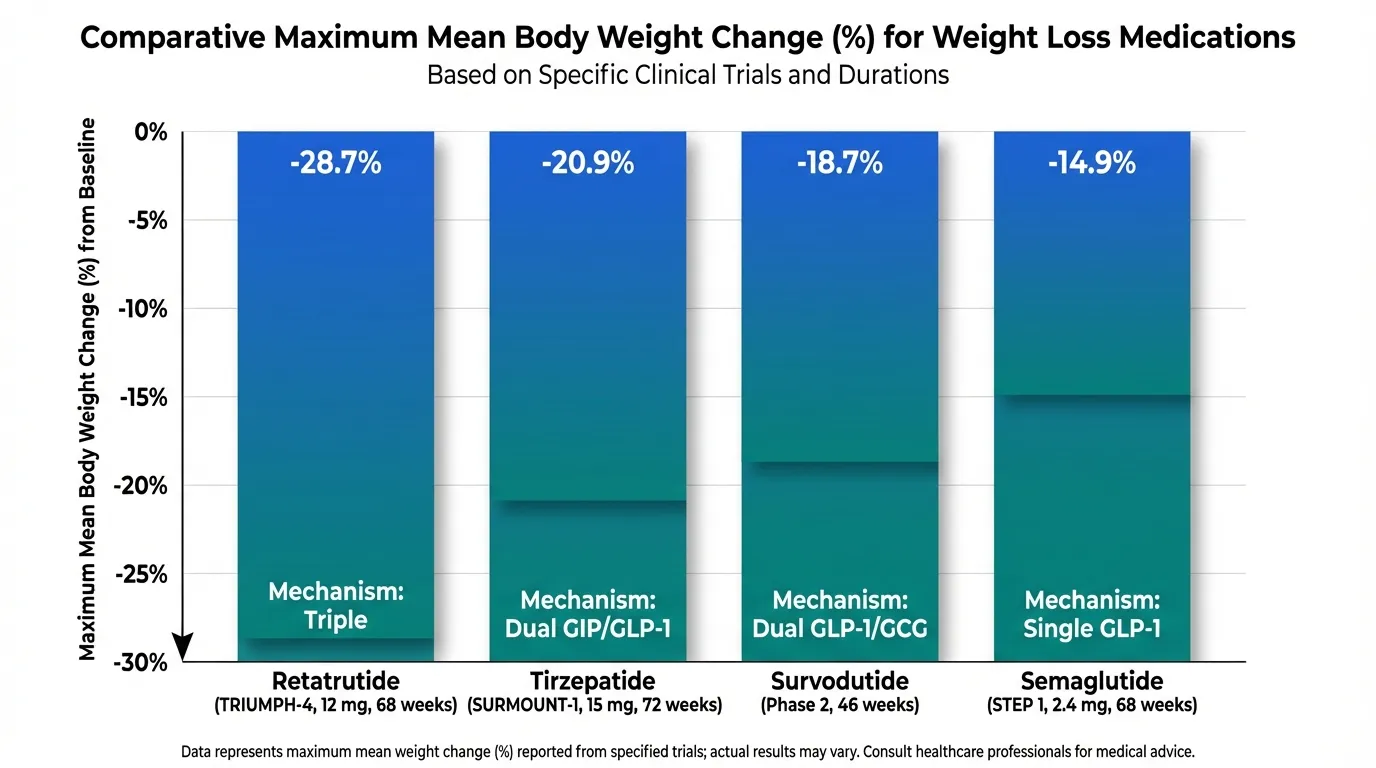
| Drug | Trial | Duration | Max Dose Weight Loss | Mechanism |
|---|---|---|---|---|
| Retatrutide | TRIUMPH-4 | 68 weeks | -28.7% | Triple (GIP/GLP-1/GCG) |
| Tirzepatide | SURMOUNT-1 | 72 weeks | -20.9% | Dual (GIP/GLP-1) |
| Semaglutide | STEP 1 | 68 weeks | -14.9% | Single (GLP-1) |
| Survodutide | Phase 2 | 46 weeks | -18.7% | Dual (GLP-1/GCG) |
A network meta-analysis published in 2025 comparing these agents confirmed that retatrutide demonstrated the greatest absolute weight reduction among the three, with a mean percentage weight loss significantly higher than both tirzepatide and semaglutide.
Safety Comparison#
| Safety Metric | Retatrutide 12 mg | Tirzepatide 15 mg | Semaglutide 2.4 mg |
|---|---|---|---|
| Nausea rate | 43.2% | ~31% | ~44% |
| Discontinuation (AEs) | 18.2% | ~6.2% | ~7.0% |
| Dysesthesia | 20.9% | Not reported | Not reported |
| Weight loss magnitude | -28.7% | -20.9% | -14.9% |
The pattern is clear: retatrutide delivers the greatest weight loss but at the cost of a higher side effect burden. The dysesthesia signal is unique to retatrutide and adds a safety consideration that does not apply to tirzepatide or semaglutide. Whether the additional ~8 percentage points of weight loss over tirzepatide justifies the increased adverse event profile is a question that will ultimately be weighed by regulators, clinicians, and patients on an individual basis.
The 9 mg Dose as a Practical Consideration#
An important clinical question is whether the 9 mg dose offers a better benefit-risk balance than 12 mg:
- Weight loss: 26.4% vs 28.7% (only 2.3 percentage points difference)
- Nausea: 38.1% vs 43.2%
- Dysesthesia: 8.8% vs 20.9% (substantial difference)
- Discontinuation: 12.2% vs 18.2%
The 9 mg dose achieves weight loss that still exceeds any other drug in Phase 3 trials while having less than half the dysesthesia rate of 12 mg. This dose may emerge as the practical "sweet spot" for many patients if retatrutide is approved.
Comprehensive Comparison: Retatrutide vs Tirzepatide vs Semaglutide#
The following table compares retatrutide with the two leading approved weight loss medications across key clinical dimensions. These are cross-trial comparisons and should be interpreted with caution, as the trials enrolled different patient populations with different baseline characteristics.
| Parameter | Retatrutide | Tirzepatide (Zepbound) | Semaglutide (Wegovy) |
|---|---|---|---|
| Mechanism | Triple agonist (GIP/GLP-1/glucagon) | Dual agonist (GIP/GLP-1) | Single agonist (GLP-1) |
| Pivotal Trial | TRIUMPH-4 (Phase 3) | SURMOUNT-1 (Phase 3) | STEP 1 (Phase 3) |
| Max Dose | 12 mg weekly | 15 mg weekly | 2.4 mg weekly |
| Trial Duration | 68 weeks | 72 weeks | 68 weeks |
| Max Weight Loss | -28.7% | -20.9% | -14.9% |
| Patients Losing 20%+ | ~58% (12 mg) | ~36% (15 mg) | ~15% (2.4 mg) |
| Nausea Rate | 43.2% | ~31% | ~44% |
| Discontinuation (AEs) | 18.2% | ~6.2% | ~7.0% |
| Dysesthesia | 20.9% (12 mg) | Not reported | Not reported |
| Dosing Frequency | Once weekly | Once weekly | Once weekly |
| Route | Subcutaneous injection | Subcutaneous injection | Subcutaneous injection |
| Approval Status | Investigational (Phase 3) | FDA-approved (2023) | FDA-approved (2021) |
| CV Outcomes Data | Pending (TRIUMPH-3) | Pending (SURMOUNT-MMO) | Positive (SELECT trial) |
Key Comparison Takeaways#
-
Weight loss magnitude: Retatrutide produces approximately 8 percentage points more weight loss than tirzepatide and 14 percentage points more than semaglutide at maximum doses, a clinically meaningful difference that could benefit patients with severe obesity.
-
Safety trade-off: The additional weight loss comes with higher discontinuation rates (18.2% vs ~6%) and the novel dysesthesia signal. Patients and clinicians will need to weigh the benefit-risk balance individually.
-
Glucagon advantage: Retatrutide's unique glucagon receptor component may provide specific advantages for liver fat reduction (relevant for MASLD/MASH) and energy expenditure that cannot be achieved with GLP-1 or dual agonists alone.
-
Availability gap: Semaglutide and tirzepatide are available now by prescription. Retatrutide will not be available until at least mid-to-late 2027 at the earliest, assuming successful Phase 3 completion and FDA approval.
What's Coming in 2026: Remaining TRIUMPH Readouts#
Seven additional TRIUMPH trial results are expected throughout 2026, which will substantially expand the evidence base for retatrutide:
TRIUMPH-1 (80-Week Obesity Trial)#
TRIUMPH-1 is particularly anticipated because its longer 80-week treatment duration (vs 68 weeks in TRIUMPH-4) may demonstrate even greater weight loss. Analysts have projected that retatrutide could exceed 30% mean weight loss in this trial. TRIUMPH-1 also includes nested protocols for obstructive sleep apnea and knee osteoarthritis, providing data on multiple obesity-related comorbidities from a single trial.
Type 2 Diabetes Trials#
Retatrutide Phase 3 trials in type 2 diabetes will determine whether the triple agonist mechanism provides superior glycemic control compared to existing therapies. The Phase 2 data showed HbA1c reductions of up to 2.0% from baseline, and the Phase 3 trials will confirm whether this translates to clinically meaningful advantages over tirzepatide in diabetes management.
MASLD/MASH Trial#
Given the glucagon receptor component's role in hepatic fat oxidation, a dedicated Phase 3 trial is evaluating retatrutide's effects on metabolic dysfunction-associated steatohepatitis (MASH). This trial will use histological endpoints (liver biopsy) to assess resolution of steatohepatitis and fibrosis regression -- a higher bar than liver fat reduction alone.
Cardiometabolic Outcomes and Additional Indications#
Additional trials are evaluating retatrutide in cardiovascular disease, chronic low back pain, and obstructive sleep apnea as standalone indications. The cardiometabolic outcomes data will be particularly important given that semaglutide has demonstrated cardiovascular benefit in the SELECT trial.
Regulatory Timeline and Path to Approval#
Based on publicly available information and the current state of the TRIUMPH program:
- Phase 3 data compilation: Seven remaining TRIUMPH trial readouts expected throughout 2026, with primary completion dates between early and mid-2026
- NDA submission: Anticipated in late 2026 or early 2027 once the complete Phase 3 data package is analyzed, though Eli Lilly has not announced an official filing timeline
- FDA review: Standard review timeline is 10-12 months from NDA submission, though priority review could shorten this to 6-8 months
- Potential approval: Earliest plausible approval is the first or second quarter of 2027 under an optimistic scenario; late 2027 or 2028 is more conservative
These timelines are estimates and may change based on trial results, the dysesthesia signal's characterization in additional trials, manufacturing readiness, and regulatory decisions. Track the latest status in our Clinical Trial Tracker.
Phase 2 Data for Reference#
The Phase 2 trial (Jastreboff et al., published in NEJM in 2023; PMID: 37366315) provided the initial efficacy signal that motivated the TRIUMPH program:
- 48-week treatment in 338 adults with obesity
- Highest dose group (12 mg) achieved -24.2% mean body weight change
- Dose-response relationship was clear across 1 mg, 4 mg, 8 mg, and 12 mg groups
- GI adverse events were common but generally manageable
- Dysesthesia was not reported as a significant signal in Phase 2
The Phase 3 TRIUMPH-4 results exceeded Phase 2 in weight loss magnitude (28.7% vs 24.2%) at a longer duration (68 vs 48 weeks), with the weight loss trajectory not fully plateaued at study end.
Outstanding Questions#
Several important questions remain for the retatrutide program:
-
Dysesthesia characterization: Will the remaining TRIUMPH trials confirm the dose-dependent pattern? Is dysesthesia transient during dose escalation or persistent during maintenance? What is the underlying mechanism?
-
TRIUMPH-1 weight loss magnitude: Will the 80-week trial confirm projections exceeding 30% mean weight loss? Will the weight loss curve plateau or continue beyond 68 weeks?
-
Optimal dose selection: The 9 mg dose achieves 26.4% weight loss with substantially less dysesthesia (8.8% vs 20.9%). Will regulators and clinicians favor this dose over 12 mg?
-
Weight regain after discontinuation: Will the pattern of weight regain seen with semaglutide and tirzepatide also apply to retatrutide? Will the glucagon receptor component affect weight maintenance differently?
-
Cardiovascular outcomes: Semaglutide demonstrated cardiovascular benefits in the SELECT trial. Whether retatrutide provides similar, different, or additional cardiovascular effects is unknown pending dedicated trial data.
-
Head-to-head comparisons: No direct comparison with tirzepatide or semaglutide has been conducted. Cross-trial comparisons are suggestive but not definitive.
-
MASH/liver fat endpoints: Will the histological endpoints in the MASH trial support a separate regulatory indication for liver disease?
Key Takeaways#
-
Retatrutide's TRIUMPH-4 results show 28.7% weight loss at 68 weeks with the 12 mg dose -- the highest ever reported in an obesity Phase 3 trial, equivalent to an average of 71.2 lbs lost.
-
Nearly 40% of patients on 12 mg lost 30%+ of body weight, approaching bariatric surgery-level results without surgical intervention.
-
Knee osteoarthritis pain was reduced by ~75%, with 12-14% of retatrutide-treated patients becoming completely pain-free, demonstrating benefits beyond weight loss alone.
-
The safety profile includes a novel dysesthesia signal affecting 20.9% of patients at 12 mg, which was not seen in Phase 2 and requires further characterization.
-
The 9 mg dose may offer the best benefit-risk balance, achieving 26.4% weight loss with dramatically lower dysesthesia rates (8.8%) and lower discontinuation rates (12.2%).
-
Seven more TRIUMPH readouts are expected in 2026, including the 80-week TRIUMPH-1 trial that may show weight loss exceeding 30%.
-
FDA approval could come as early as Q1-Q2 2027 if remaining trials are successful and regulatory review proceeds on standard timelines.
This article is for educational and informational purposes only. Retatrutide is an investigational drug not approved for any use. This article does not constitute medical advice or encouragement to seek access to investigational compounds.
Frequently Asked Questions About Retatrutide Phase 3 Results#
What are the latest retatrutide Phase 3 results?#
The TRIUMPH-4 Phase 3 trial, reported in December 2025, showed retatrutide achieved 28.7% mean body weight loss (71.2 lbs) at 68 weeks with the 12 mg dose and 26.4% (64.2 lbs) with the 9 mg dose, compared to 2.1% with placebo. These are the highest weight loss percentages ever reported in any Phase 3 obesity trial. The trial also demonstrated significant reductions in knee osteoarthritis pain. Seven additional TRIUMPH trial readouts are expected throughout 2026, including the 80-week TRIUMPH-1 study.
How much weight loss does retatrutide cause?#
In the TRIUMPH-4 Phase 3 trial, participants on retatrutide 12 mg lost an average of 28.7% of their body weight (71.2 lbs) over 68 weeks. At the 9 mg dose, weight loss averaged 26.4% (64.2 lbs). Nearly 40% of patients on the 12 mg dose lost 30% or more of their body weight. The longer 80-week TRIUMPH-1 trial may show even greater weight loss, with some analysts projecting results above 30%.
When will retatrutide be FDA approved?#
No official FDA approval date has been announced. Eli Lilly has seven remaining Phase 3 TRIUMPH trial readouts expected throughout 2026. If trials are successful, an NDA submission is anticipated in late 2026 or early 2027, with potential FDA approval in the first or second quarter of 2027 under standard review timelines. These are estimates and subject to change based on trial results and regulatory decisions.
How does retatrutide compare to tirzepatide and semaglutide?#
Retatrutide produces substantially greater weight loss than both tirzepatide (28.7% vs 20.9%) and semaglutide (28.7% vs 14.9%) in their respective Phase 3 trials. However, retatrutide has higher rates of GI side effects and discontinuation, plus the novel dysesthesia signal. No head-to-head trial has been conducted, so cross-trial comparisons should be interpreted cautiously.
What is the dysesthesia side effect from retatrutide?#
Dysesthesia is an abnormal or unpleasant touch sensation that emerged as a novel safety signal in TRIUMPH-4. It occurred in 8.8% of patients on the 9 mg dose and 20.9% on the 12 mg dose, compared to just 0.7% with placebo. This side effect was not seen in Phase 2 and has not been reported with other incretin-based therapies. Eli Lilly reports that events were generally mild and did not appear to be a primary driver of treatment discontinuation.
Related Articles#

{kind=link}
Frequently Asked Questions About Retatrutide Phase 3 Results 2026: TRIUMPH Trial Weight Loss Data
How much weight loss with retatrutide?
In the TRIUMPH-4 Phase 3 trial, participants on retatrutide 12 mg lost an average of 28.7% of their body weight (71.2 lbs) over 68 weeks. At the 9 mg dose, weight loss averaged 26.4% (64.2 lbs). Nearly 40% of patients on the 12 mg dose lost 30% or more of their body weight. The longer 80-week TRIUMPH-1 trial may show even greater weight loss, with some analysts projecting results above 30%. These are the highest weight loss percentages ever reported in any Phase 3 obesity trial.
Is retatrutide FDA-approved?
No. As of April 2026, retatrutide is an investigational drug and is NOT FDA-approved for any indication. It remains in Phase 3 clinical trials under Eli Lilly's TRIUMPH program. No official FDA approval timeline has been announced. Retatrutide cannot legally be prescribed for weight loss or any other use in the United States outside of clinical trial settings.
When will retatrutide be available?
Retatrutide is not expected to be available by prescription before 2027 at the earliest. Eli Lilly has seven remaining Phase 3 TRIUMPH trial readouts expected throughout 2026. If these trials succeed, an NDA submission is anticipated in late 2026 or early 2027, with potential FDA approval in Q1-Q2 2027 under standard review timelines, or later under more conservative scenarios. Commercial launch would follow approval.
Retatrutide vs tirzepatide — which is better?
For raw weight loss, retatrutide produces substantially more than tirzepatide — 28.7% at 68 weeks (TRIUMPH-4) vs 20.9% at 72 weeks (SURMOUNT-1). However, tirzepatide is FDA-approved and available now, while retatrutide is investigational. Retatrutide also has higher rates of nausea (43% vs ~31%), higher treatment discontinuation (18.2% vs ~6.2%), and a novel dysesthesia signal (20.9% at 12 mg) not seen with tirzepatide. No head-to-head trial has been conducted. For most patients today, tirzepatide is the practical choice; retatrutide is more compelling for severe obesity if tolerated and once approved.
Retatrutide side effects?
The most common retatrutide side effects in TRIUMPH-4 were nausea (43.2% at 12 mg), diarrhea (33.1%), constipation (25.0%), vomiting (20.9%), and decreased appetite (18.2%). A novel dysesthesia signal — abnormal or unpleasant touch sensations — occurred in 20.9% of patients on the 12 mg dose and 8.8% on the 9 mg dose, versus 0.7% with placebo. Treatment discontinuation due to adverse events was 18.2% at 12 mg. GI events were generally most intense during dose escalation. All data are from clinical trials; retatrutide is not FDA-approved.
What is the dysesthesia side effect from retatrutide?
Dysesthesia is an abnormal or unpleasant touch sensation that emerged as a novel safety signal in the TRIUMPH-4 Phase 3 trial. It occurred in 8.8% of patients on the 9 mg dose and 20.9% on the 12 mg dose, compared to just 0.7% with placebo. This side effect was not seen in Phase 2 trials and has not been reported with other GLP-1 or dual agonist drugs. Eli Lilly reports that events were generally mild and did not appear to be a primary driver of treatment discontinuation.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Peptides in Clinical Trials 2026: The Most Promising Pipeline
A research-focused overview of the most promising peptides in clinical trials as of 2026, including Retatrutide Phase 3 TRIUMPH data, Survodutide, Mazdutide, Ecnoglutide, and other emerging compounds reshaping metabolic medicine.
Weight Loss Peptides: Mechanisms, Evidence, and How They Compare
A mechanism-focused guide to weight loss peptides — how GLP-1, GIP, and glucagon pathways drive fat loss, how single, dual, and triple agonists compare, and what the clinical evidence actually shows.

GLP-1 Drug Cost Comparison 2026: Insurance, Cash, and Compounded Pricing
A comprehensive comparison of GLP-1 medication costs in 2026, covering brand name, generic, and compounded pricing for semaglutide, tirzepatide, and liraglutide, plus insurance coverage strategies and cost-saving options.
You Might Also Like
Related content you may find interesting