Triple Agonists Explained: The Future of Weight Loss Treatment

Introduction#
The evolution of anti-obesity pharmacotherapy has followed a clear trajectory: from single to dual to triple receptor agonists, with each generation producing greater weight loss. The latest clinical data from retatrutide's Phase 3 TRIUMPH program confirmed what the field had hypothesized -- targeting three metabolic hormone receptors simultaneously produces the highest weight loss ever observed in clinical trials.
This review examines the science behind triple (and quadruple) receptor agonists, why adding glucagon receptor agonism to the GLP-1 backbone matters, and what the clinical data reveal about this emerging drug class.
Important: All triple and quadruple agonists discussed are investigational. None are FDA-approved.
The Evolution: From Single to Triple Agonism#
Generation 1: GLP-1 Monoagonists#
The first generation targeted only the GLP-1 receptor:
- Semaglutide (Wegovy): 14.9% weight loss at 68 weeks
- Mechanism: Appetite suppression, delayed gastric emptying, improved insulin sensitivity
Generation 2: Dual Agonists#
Adding a second receptor target improved efficacy:
- Tirzepatide (GLP-1 + GIP): 20.9% weight loss at 72 weeks
- Survodutide (GLP-1 + glucagon): 18.7% at 46 weeks
- CagriSema (GLP-1 + amylin): 22.7% at 68 weeks
Generation 3: Triple Agonists#
Adding a third receptor pushed weight loss further:
- Retatrutide (GLP-1 + GIP + glucagon): 28.7% at 68 weeks
Generation 4: Quadruple Agonists#
The latest frontier adds a fourth receptor:
- Bioglutide/NA-931 (GLP-1 + GIP + glucagon + IGF-1): 13.8% at 13 weeks (Phase 2)
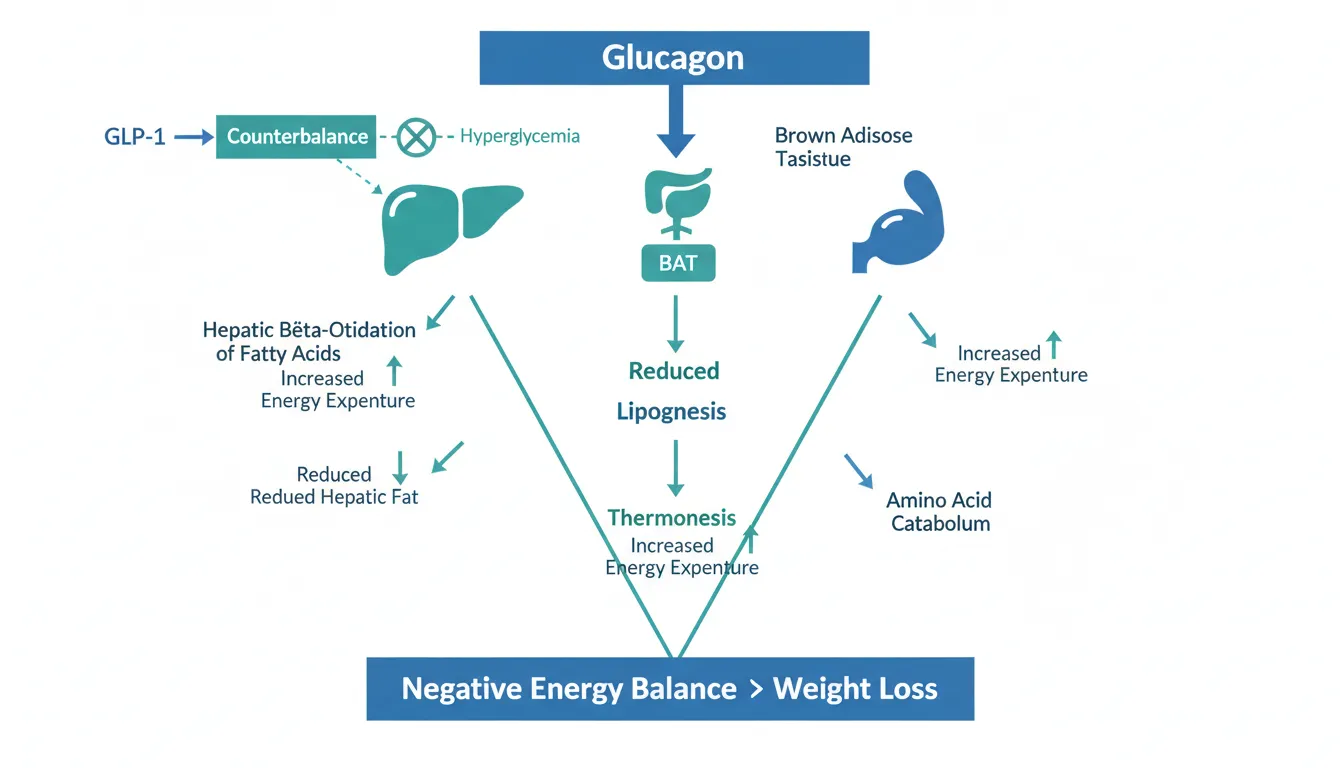
Why Glucagon Matters#
The addition of glucagon receptor agonism to the GLP-1 backbone is the key innovation distinguishing triple agonists from dual GLP-1/GIP agonists like tirzepatide. Glucagon contributes to weight loss through mechanisms distinct from GLP-1:
Energy Expenditure#
Glucagon increases resting energy expenditure by stimulating hepatic thermogenesis and brown adipose tissue activation. While GLP-1 primarily reduces energy intake (appetite suppression), glucagon increases energy output, attacking the energy balance equation from both sides simultaneously.
Hepatic Fat Metabolism#
Glucagon promotes hepatic beta-oxidation of fatty acids and reduces hepatic lipogenesis. This is why glucagon-containing agonists (survodutide, retatrutide) show particular promise for MASH/MASLD, where liver fat accumulation is the core pathology.
Amino Acid Metabolism#
Glucagon stimulates amino acid catabolism and ureagenesis. This may have implications for lean mass dynamics, though the clinical impact is complex and dose-dependent.
Glycogenolysis#
Glucagon promotes glycogen breakdown, which could theoretically raise blood glucose. However, in the context of dual or triple agonists, the concurrent GLP-1 agonism (which promotes insulin secretion and suppresses glucagon) counterbalances this effect, maintaining glycemic control.
Retatrutide: The Triple Agonist Leader#
Mechanism#
Retatrutide is a single peptide molecule that activates three receptors:
- GLP-1 receptor: Appetite suppression, insulin secretion, delayed gastric emptying
- GIP receptor: Insulin potentiation, possible adipose tissue effects
- Glucagon receptor: Increased energy expenditure, hepatic fat oxidation
The peptide uses a C20 fatty diacid to enable albumin binding and a ~5-day half-life for weekly dosing.
Phase 3 TRIUMPH-4 Results#
The TRIUMPH-4 trial enrolled participants with obesity and knee osteoarthritis:
| Dose | Weight Loss | vs Placebo |
|---|---|---|
| Retatrutide 9 mg | 26.4% | 24.3 pp |
| Retatrutide 12 mg | 28.7% | 26.6 pp |
| Placebo | 2.1% | -- |
Key secondary outcomes at 12 mg:
- Average weight loss of 71.2 lbs (32.3 kg)
- Systolic blood pressure reduced by 14.0 mmHg
- Significant improvements in non-HDL cholesterol, hs-CRP, and triglycerides
- WOMAC knee pain reduced by 75.8% (4.5 points)
- More than 1 in 8 patients were completely free of knee pain
Why 28.7% Is Remarkable#
To put retatrutide's result in context:
| Drug | Mechanism | Weight Loss | Duration |
|---|---|---|---|
| Retatrutide 12 mg | GLP-1/GIP/GCG | 28.7% | 68 wk |
| CagriSema | GLP-1 + Amylin | 22.7% | 68 wk |
| Tirzepatide 15 mg | GLP-1/GIP | 20.9% | 72 wk |
| SC Semaglutide 2.4 mg | GLP-1 | 14.9% | 68 wk |
The incremental benefit of adding glucagon agonism (retatrutide vs tirzepatide) appears to be approximately 7-8 percentage points of additional weight loss, comparable to the benefit of adding GIP agonism to GLP-1 alone (tirzepatide vs semaglutide, ~6 percentage points).
Phase 3 Program#
Seven additional Phase 3 TRIUMPH readouts are expected in 2026, including studies evaluating maintenance dosing strategies. The full program will generate data across obesity, T2D, obstructive sleep apnea, and osteoarthritis.
The Glucagon Partners: Survodutide and Pemvidutide#
While retatrutide combines glucagon with GLP-1 and GIP, two other drugs pair glucagon specifically with GLP-1, helping isolate glucagon's contribution:
Survodutide (Boehringer Ingelheim)#
Mechanism: Dual GLP-1/glucagon agonist Phase 2: 18.7% weight loss at 46 weeks Phase 3: SYNCHRONIZE program, results expected 2026 Breakthrough therapy designation: For MASH
Survodutide's 18.7% result demonstrates that GLP-1 + glucagon alone produces weight loss exceeding GLP-1 monoagonism (~15%) but below retatrutide's triple agonism (~29%). The glucagon component contributes approximately 3-4 percentage points of additional weight loss beyond GLP-1 alone.
Pemvidutide (Altimmune)#
Mechanism: Dual GLP-1/glucagon agonist Phase 2 MOMENTUM: 15.6% weight loss at 48 weeks Key differentiator: Class-leading lean mass preservation
Pemvidutide's most notable feature is body composition: only 21.9% of weight lost was lean mass, compared to the typical 25-40% with GLP-1 agonists alone. This suggests that glucagon's thermogenic effects may preferentially target fat mass while preserving muscle, a critical advantage for long-term metabolic health.
Bioglutide (NA-931): The Quadruple Agonist#
A New Paradigm#
Bioglutide (NA-931) represents the next leap in multi-receptor agonism. Developed by Biomed Industries, it is the first oral small molecule that simultaneously activates four metabolic hormone receptors:
- GLP-1 receptor: Appetite suppression, glycemic control
- GIP receptor: Insulin potentiation
- Glucagon receptor: Energy expenditure, liver fat reduction
- IGF-1 receptor: Growth signaling, anabolic effects
Why IGF-1?#
The addition of IGF-1 receptor agonism is the most novel aspect of bioglutide. IGF-1 signaling promotes:
- Muscle protein synthesis and preservation of lean mass
- Bone mineral density maintenance
- Cellular repair and regeneration
In theory, activating IGF-1 alongside the weight-loss-inducing GLP-1, GIP, and glucagon pathways could preserve or even increase lean mass during weight loss, addressing one of the most significant limitations of current anti-obesity therapies.
Phase 2 Results#
A 13-week multiple ascending dose study enrolled 125 participants:
| Dose | Weight Loss | vs Placebo |
|---|---|---|
| NA-931 150 mg (oral) | 13.8% | 11.9% |
| Placebo | ~2% | -- |
Additional findings:
- Up to 72% of treated subjects achieved 12% or greater weight loss at 13 weeks
- No muscle loss was observed
- TEAEs were insignificant or mild
- Drug absorption was unaffected by food (no fasting required)
- Oral daily dosing
Caveats#
While the Phase 2 data are impressive, several caveats apply:
- Small sample size (125 participants)
- Short duration (13 weeks)
- Limited peer-reviewed publication
- The company (Biomed Industries) is a smaller biotech without the resources of Lilly or Novo Nordisk
- Phase 3 has been announced but details are limited
Comparing Multi-Receptor Approaches#
| Feature | Retatrutide | Survodutide | Pemvidutide | Bioglutide |
|---|---|---|---|---|
| Receptors | GLP-1/GIP/GCG | GLP-1/GCG | GLP-1/GCG | GLP-1/GIP/GCG/IGF-1 |
| Route | SC weekly | SC weekly | SC weekly | Oral daily |
| Weight loss | 28.7% (68wk) | 18.7% (46wk) | 15.6% (48wk) | 13.8% (13wk) |
| Phase | Phase 3 | Phase 3 | Phase 2 | Phase 2 |
| Lean mass | Not reported | Not reported | 78.1% fat | No muscle loss |
| MASH data | Expected | BTD granted | Phase 2b positive | Not reported |
| Company | Eli Lilly | Boehringer | Altimmune | Biomed Industries |
The Glucagon Safety Question#
Adding glucagon agonism raises specific safety considerations:
Hyperglycemia Risk#
Glucagon's primary physiological role is to raise blood glucose. In the context of triple agonists, GLP-1-mediated insulin secretion counterbalances this effect. In TRIUMPH-4, retatrutide did not produce clinically significant hyperglycemia. However, the balance between glucagon's hyperglycemic potential and GLP-1's glucose-lowering effect may be critical in patients with type 2 diabetes.
Heart Rate#
GLP-1 agonists typically increase heart rate by 2-4 bpm. Glucagon can also increase heart rate. Whether triple agonists produce additive heart rate effects requires monitoring in Phase 3 studies.
GI Tolerability#
Triple agonism produces higher GI side effect rates than dual agonism. In retatrutide Phase 2 data, nausea (38-43%), diarrhea (33-35%), and vomiting (20-21%) were all higher than with tirzepatide or semaglutide. Whether this is a dose-dependent effect that can be mitigated with optimized titration is being evaluated in the TRIUMPH program.
Hepatic Effects#
Glucagon stimulates amino acid metabolism and ketogenesis, which could theoretically stress the liver. However, the net effect appears beneficial: survodutide has breakthrough therapy designation for MASH precisely because glucagon agonism reduces hepatic steatosis.
What the Data Tell Us#
The Receptor Hierarchy#
The clinical data suggest an approximate hierarchy of weight loss contribution:
- GLP-1 agonism alone: ~15% weight loss (semaglutide)
- Adding GIP agonism: +5-6 pp (tirzepatide ~21%)
- Adding glucagon agonism: +3-4 pp (survodutide ~19%) or +7-8 pp when combined with GIP (retatrutide ~29%)
- Adding IGF-1 agonism: Under investigation (bioglutide early data)
The combination of all three incretin-related pathways (GLP-1 + GIP + glucagon) appears to produce a synergistic rather than merely additive effect on weight loss.
The Body Composition Question#
Triple agonists may preserve lean mass better than GLP-1 monoagonists. Pemvidutide's 78.1% fat mass ratio is significantly better than the typical 60-75% observed with GLP-1 alone. Retatrutide's glucagon component and bioglutide's IGF-1 component may also contribute to lean mass preservation, though definitive body composition data are pending.
What to Watch in 2026#
- Retatrutide TRIUMPH readouts -- Seven more Phase 3 results expected, which will define the drug's clinical profile across multiple indications
- Survodutide SYNCHRONIZE results -- Phase 3 data will establish whether GLP-1/glucagon dual agonism achieves >20% weight loss at longer treatment durations
- Bioglutide Phase 3 initiation -- Advancement of the first quadruple agonist into late-stage development
- Body composition data -- Lean mass preservation may become as important as total weight loss in differentiating next-generation agents
Conclusion#
Triple agonists represent the current frontier of anti-obesity pharmacotherapy. Retatrutide's 28.7% weight loss in Phase 3 confirms that targeting GLP-1, GIP, and glucagon receptors simultaneously produces weight loss approaching bariatric surgery levels. The emergence of quadruple agonists like bioglutide, which add IGF-1 signaling to address lean mass preservation, suggests the field is far from reaching its ceiling.
The key question going forward is not whether multi-receptor agonists are more effective -- they clearly are -- but how to optimize the risk-benefit ratio: maximizing weight loss and metabolic improvement while maintaining tolerability and safety.
This article is for educational and informational purposes only. It does not constitute medical advice.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Survodutide Overview and Research Guide
- Survodutide Dosing Protocols
- Survodutide Side Effects and Safety
- Pemvidutide Overview and Research Guide
- Pemvidutide Dosing Protocols
- Pemvidutide Side Effects and Safety
- Bioglutide Overview and Research Guide
- Bioglutide Dosing Protocols
- Bioglutide Side Effects and Safety
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About Triple Agonists Explained: The Future of Weight Loss Treatment
What does this article cover?
A research review of triple and quadruple receptor agonists for obesity, from retatrutide's record-breaking 28.7% weight loss to bioglutide's quad-agonist approach, and why adding glucagon matters. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Retatrutide, Survodutide, Pemvidutide, Bioglutide, Semaglutide. Key context: Retatrutide (First-in-class triple GIP/GLP-1/glucagon agonist with 28.7% weight loss in Phase 3); Survodutide (Dual GLP-1/glucagon agonist demonstrating glucagon's contribution to weight loss); Pemvidutide (Dual GLP-1/glucagon agonist with class-leading lean mass preservation). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: First-in-class triple GIP/GLP-1/glucagon agonist with 28.7% weight loss in Phase 3. Dual GLP-1/glucagon agonist demonstrating glucagon's contribution to weight loss. Dual GLP-1/glucagon agonist with class-leading lean mass preservation. These takeaways are based on the research data available at the time of publication.
What is Retatrutide and why is it significant?
Retatrutide is a peptide discussed in this article because: First-in-class triple GIP/GLP-1/glucagon agonist with 28.7% weight loss in Phase 3. For a complete profile of Retatrutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

GLP-1 Drugs for MASH and Liver Disease: Beyond Weight Loss
Research review of GLP-1 and multi-receptor agonists for MASH (metabolic dysfunction-associated steatohepatitis), including survodutide, pemvidutide, mazdutide, semaglutide, and tirzepatide liver-specific clinical data.

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.
Peptides in Clinical Trials 2026: The Most Promising Pipeline
A research-focused overview of the most promising peptides in clinical trials as of 2026, including Retatrutide Phase 3 TRIUMPH data, Survodutide, Mazdutide, Ecnoglutide, and other emerging compounds reshaping metabolic medicine.
You Might Also Like
Related content you may find interesting