How Semaglutide Works for Weight Loss: Mechanism of Action Explained

Introduction#
Semaglutide has become one of the most prescribed medications in the world, generating significant public interest in how a weekly injection can produce substantial and sustained weight loss. Marketed as Wegovy (for weight management) and Ozempic (for type 2 diabetes), semaglutide consistently produces 15-17% body weight loss in clinical trials -- far exceeding what was previously achievable with anti-obesity medications.
Understanding how semaglutide works requires looking at multiple levels: the molecular interaction with the GLP-1 receptor, the downstream effects on appetite and metabolism, and the clinical evidence documenting these effects in large patient populations.
This article reviews the mechanism of action of semaglutide in detail, covering everything from receptor pharmacology to the key clinical trial results.
For information about when semaglutide's effects become noticeable, see our peptide timelines guide.
GLP-1: The Endogenous Hormone#
What GLP-1 Does Naturally#
Glucagon-like peptide-1 (GLP-1) is a hormone produced primarily by L-cells in the small intestine in response to food intake. It is part of the incretin system -- a set of gut hormones that regulate blood sugar and appetite after eating.
Natural GLP-1 has several effects:
| Effect | Mechanism | Location |
|---|---|---|
| Insulin secretion | Stimulates glucose-dependent insulin release | Pancreatic beta cells |
| Glucagon suppression | Reduces glucagon secretion (lowers blood sugar) | Pancreatic alpha cells |
| Appetite reduction | Signals satiety to the brain | Hypothalamus, brainstem |
| Gastric emptying | Slows the rate at which the stomach empties | Vagus nerve, stomach |
| Nausea (at high levels) | Central and peripheral nervous system stimulation | Brainstem area postrema |
The Problem with Natural GLP-1#
Natural GLP-1 has a half-life of approximately 2 minutes. It is rapidly degraded by the enzyme dipeptidyl peptidase-4 (DPP-4) and cleared by the kidneys. This extremely short half-life means that natural GLP-1 cannot be used as a drug -- it would need to be infused continuously.
This is why GLP-1 receptor agonists like semaglutide were developed: to mimic GLP-1's effects with a molecule that lasts much longer in the body.
How Semaglutide Was Engineered#
Semaglutide is a modified version of human GLP-1 with three key structural changes that extend its duration of action:
1. Amino Acid Substitution (Position 8)#
The alanine at position 8 of native GLP-1 is replaced with alpha-aminoisobutyric acid (Aib). This modification makes semaglutide resistant to degradation by DPP-4, the enzyme that destroys natural GLP-1 within minutes.
2. Fatty Acid Side Chain (C18)#
A C18 fatty diacid chain is attached to lysine at position 26 via a linker. This fatty acid binds to albumin in the blood. Since albumin has a half-life of approximately 19 days, semaglutide essentially hitchhikes on albumin, dramatically slowing its clearance from the body.
3. Amino Acid Substitution (Position 34)#
Lysine at position 34 is replaced with arginine to prevent the fatty acid chain from attaching at the wrong position during manufacturing.
The result of these modifications: semaglutide has a half-life of approximately 7 days (compared to 2 minutes for natural GLP-1), enabling once-weekly dosing.
For more on how chemical modifications affect peptide stability and pharmacokinetics, see our peptide stability guide.
Mechanisms of Weight Loss#
Semaglutide produces weight loss through several interconnected mechanisms:
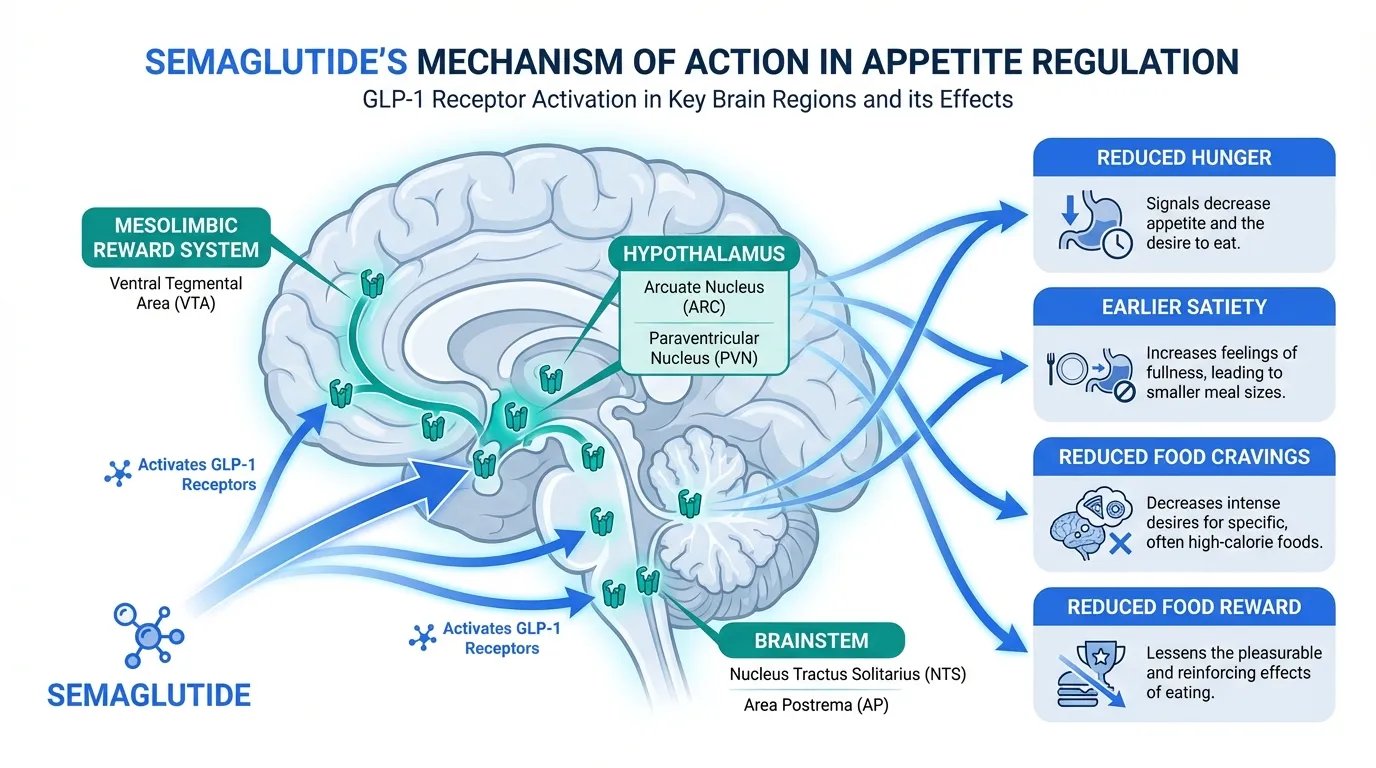
1. Central Appetite Suppression#
The most significant mechanism driving semaglutide's weight loss effect is central appetite suppression -- reducing hunger and food cravings through direct effects on the brain.
GLP-1 receptors are expressed in several brain regions involved in appetite regulation:
- Hypothalamus: The arcuate nucleus and paraventricular nucleus, which regulate hunger and satiety signaling
- Brainstem: The nucleus tractus solitarius (NTS) and area postrema, which process satiety signals from the gut
- Mesolimbic reward system: Regions involved in the hedonic (pleasure-driven) aspects of eating
Semaglutide activates these receptors, producing:
- Reduced hunger: Patients report feeling less hungry between meals
- Earlier satiety: Feeling full sooner during meals, leading to smaller portion sizes
- Reduced food cravings: Decreased desire for high-calorie, palatable foods
- Reduced food reward: Food becomes less rewarding, reducing the drive to eat beyond physiological need
Research using functional MRI has shown that semaglutide reduces brain activation in reward centers when patients are shown images of highly palatable foods, providing objective evidence for the food reward reduction effect.
2. Delayed Gastric Emptying#
Semaglutide slows the rate at which the stomach empties its contents into the small intestine. This means food stays in the stomach longer after a meal, contributing to a prolonged feeling of fullness.
This effect is most pronounced in the early weeks of treatment and may partially attenuate with continued use. It is also the mechanism behind the most common side effect -- nausea -- which tends to improve over time as the body adapts.
3. Metabolic Effects#
Beyond appetite and gastric emptying, semaglutide has metabolic effects that may contribute to weight management:
- Improved insulin sensitivity: Reduced body weight and direct GLP-1 receptor effects improve how the body responds to insulin
- Reduced hepatic glucose output: Less glucose production by the liver
- Potential effects on energy expenditure: Some data suggest GLP-1 agonists may have modest effects on resting metabolic rate, though this remains debated
4. What Semaglutide Does NOT Do#
Understanding what semaglutide does not do is equally important:
- It does not burn fat directly. The weight loss comes from reduced caloric intake, not from direct fat metabolism
- It does not increase metabolic rate significantly. Unlike some stimulant-based weight loss drugs, semaglutide works primarily through appetite suppression
- It does not selectively target visceral fat. Weight loss occurs from both visceral and subcutaneous fat, roughly proportional to starting levels
- It does not build muscle. Some lean mass loss occurs alongside fat loss, as is typical with caloric deficit
Key Clinical Trial Results#
The STEP Trial Program#
The STEP (Semaglutide Treatment Effect in People with obesity) program is the largest clinical trial program for a weight management drug. Key results from the pivotal trials:
| Trial | Population | Dose | Duration | Mean Weight Loss |
|---|---|---|---|---|
| STEP 1 | Obesity without diabetes | 2.4 mg weekly | 68 weeks | -14.9% (vs -2.4% placebo) |
| STEP 2 | Obesity with type 2 diabetes | 2.4 mg weekly | 68 weeks | -9.6% (vs -3.4% placebo) |
| STEP 3 | Obesity + intensive behavioral therapy | 2.4 mg weekly | 68 weeks | -16.0% (vs -5.7% placebo) |
| STEP 4 | Withdrawal study | 2.4 mg weekly | 68 weeks | Weight regain after discontinuation |
| STEP 5 | Extended treatment | 2.4 mg weekly | 104 weeks | -15.2% (maintained at 2 years) |
What the Numbers Mean#
- Approximately one-third of patients on semaglutide 2.4 mg lost 20% or more of their body weight
- Weight loss was progressive through approximately week 60, then plateaued
- Patients with type 2 diabetes lost less weight on average (consistent with known resistance to GLP-1-mediated weight loss in diabetes)
- STEP 4 showed that most weight is regained within a year of stopping semaglutide, indicating that continued treatment is necessary to maintain weight loss
Cardiovascular Outcomes#
The SELECT trial demonstrated that semaglutide 2.4 mg reduced major adverse cardiovascular events (MACE) by 20% in patients with established cardiovascular disease and obesity but without diabetes. This was a landmark finding because it showed cardiovascular benefit from weight loss independent of blood sugar control.
Side Effect Profile#
The most common side effects of semaglutide are gastrointestinal:
| Side Effect | Frequency | Timing | Management |
|---|---|---|---|
| Nausea | 40-45% | Most common during dose escalation | Usually improves over weeks |
| Diarrhea | 25-30% | Variable | Dietary modification |
| Vomiting | 20-25% | Most common during dose escalation | Usually improves over weeks |
| Constipation | 20-25% | Can be persistent | Fiber, hydration, stool softeners |
| Abdominal pain | 15-20% | Variable | Usually mild |
These GI side effects are mechanism-related -- they result from the same GLP-1 receptor activation that produces the therapeutic effects. The dose titration schedule (starting at 0.25 mg and increasing monthly) is designed to minimize these effects by allowing the body to adapt gradually.
For a comprehensive review of peptide side effects, see our peptide therapy side effects guide. To compare side effects across different peptides, use our side effects comparison tool.
Semaglutide vs. Next-Generation Peptides#
Semaglutide targets only the GLP-1 receptor. Newer peptides target multiple receptors simultaneously:
| Peptide | Targets | Max Weight Loss (Trials) | Status |
|---|---|---|---|
| Semaglutide | GLP-1 only | ~17% | FDA approved |
| Tirzepatide | GLP-1 + GIP | ~20.9% | FDA approved |
| Survodutide | GLP-1 + Glucagon | ~19% (Phase 2) | Phase 3 |
| Retatrutide | GLP-1 + GIP + Glucagon | ~28.7% (Phase 3 TRIUMPH-4) | Phase 3 |
The trend toward multi-target agonists reflects the understanding that obesity involves multiple hormonal pathways. Tirzepatide adds GIP receptor agonism, which appears to enhance weight loss and may improve tolerability. Retatrutide adds glucagon receptor agonism, which increases energy expenditure -- addressing a mechanism that semaglutide alone does not.
For detailed comparisons, see our peptide comparison articles.
The Weight Regain Problem#
One of the most important clinical findings about semaglutide is from STEP 4: patients who discontinued semaglutide regained approximately two-thirds of their lost weight within one year. This finding has significant implications:
- Obesity is a chronic disease that requires ongoing treatment, similar to hypertension or diabetes
- Semaglutide does not "reset" the body's weight set point -- the biological drivers of weight regain persist
- Stopping treatment removes the appetite suppression that enabled reduced caloric intake
- Combination with lifestyle changes (diet, exercise, behavioral therapy) may attenuate but does not eliminate weight regain
This has led to the clinical consensus that semaglutide, like other chronic disease medications, should be continued long-term for sustained benefit.
Key Takeaways#
-
Semaglutide works primarily through central appetite suppression. It activates GLP-1 receptors in brain regions controlling hunger, satiety, and food reward, leading to reduced caloric intake.
-
Chemical modifications give it a 7-day half-life. A fatty acid side chain binds albumin, and amino acid substitutions resist enzymatic degradation, enabling once-weekly dosing.
-
Clinical trials demonstrate 15-17% average body weight loss at the 2.4 mg dose, with approximately one-third of patients losing 20% or more.
-
GI side effects are the most common. Nausea, diarrhea, and vomiting are mechanism-related and typically improve during dose titration.
-
Weight is regained after discontinuation. STEP 4 showed that most weight returns within a year of stopping treatment, supporting long-term use.
-
Next-generation multi-agonists like tirzepatide and retatrutide target additional receptors beyond GLP-1 and may produce greater weight loss.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety
- GLP-1 Overview and Research Guide
- GLP-1 Dosing Protocols
- GLP-1 Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety

{kind=link}
Frequently Asked Questions About How Semaglutide Works for Weight Loss: Mechanism of Action Explained
What does this article cover?
How semaglutide causes weight loss — GLP-1 receptor signaling, appetite regulation, gastric emptying, and STEP clinical trial results. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Semaglutide, Tirzepatide, GLP-1, Retatrutide. Key context: Semaglutide (The primary subject of this article, an FDA-approved GLP-1 receptor agonist that produces signifi...); Tirzepatide (Dual GIP/GLP-1 agonist compared to semaglutide, representing the next generation of incretin-base...); GLP-1 (The endogenous hormone that semaglutide mimics, providing context for understanding the peptide's...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: The primary subject of this article, an FDA-approved GLP-1 receptor agonist that produces signifi.... Dual GIP/GLP-1 agonist compared to semaglutide, representing the next generation of incretin-base.... The endogenous hormone that semaglutide mimics, providing context for understanding the peptide's.... These takeaways are based on the research data available at the time of publication.
What is Semaglutide and why is it significant?
Semaglutide is a peptide discussed in this article because: The primary subject of this article, an FDA-approved GLP-1 receptor agonist that produces significant weight loss through multiple mechanisms. For a complete profile of Semaglutide, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

The History of Peptide Research: From Insulin to Modern Therapeutics
History of peptide research from insulin's 1921 discovery to modern GLP-1 agonists. Key milestones in synthesis and therapeutics.

The Evolution of GLP-1 Receptor Agonists: From Single-Target to Multi-Receptor Metabolic Therapeutics
A research review tracing the evolution of GLP-1 receptor agonists from semaglutide through tirzepatide, retatrutide, and survodutide, examining how multi-receptor approaches have progressively expanded efficacy in obesity and metabolic disease.

Retatrutide Canada Guide
Retatrutide in Canada: Everything You Need to Know — part of the Next-Gen Weight Loss content cluster.
You Might Also Like
Related content you may find interesting