Subcutaneous vs Intramuscular Peptide Injection: What Research Shows

Introduction#
The route of administration -- how a peptide enters the body -- significantly affects its absorption rate, bioavailability, onset of action, and overall pharmacokinetic profile. For injectable peptides, the two most common routes are subcutaneous (SubQ) and intramuscular (IM) injection.
Most research peptides and FDA-approved peptide drugs are administered subcutaneously. However, some peptides are given intramuscularly, and understanding the differences between these routes helps explain why specific routes are preferred for specific compounds.
This article compares subcutaneous and intramuscular injection in terms of absorption, technique, injection sites, and peptide-specific considerations.
Subcutaneous Injection (SubQ)#
What It Is#
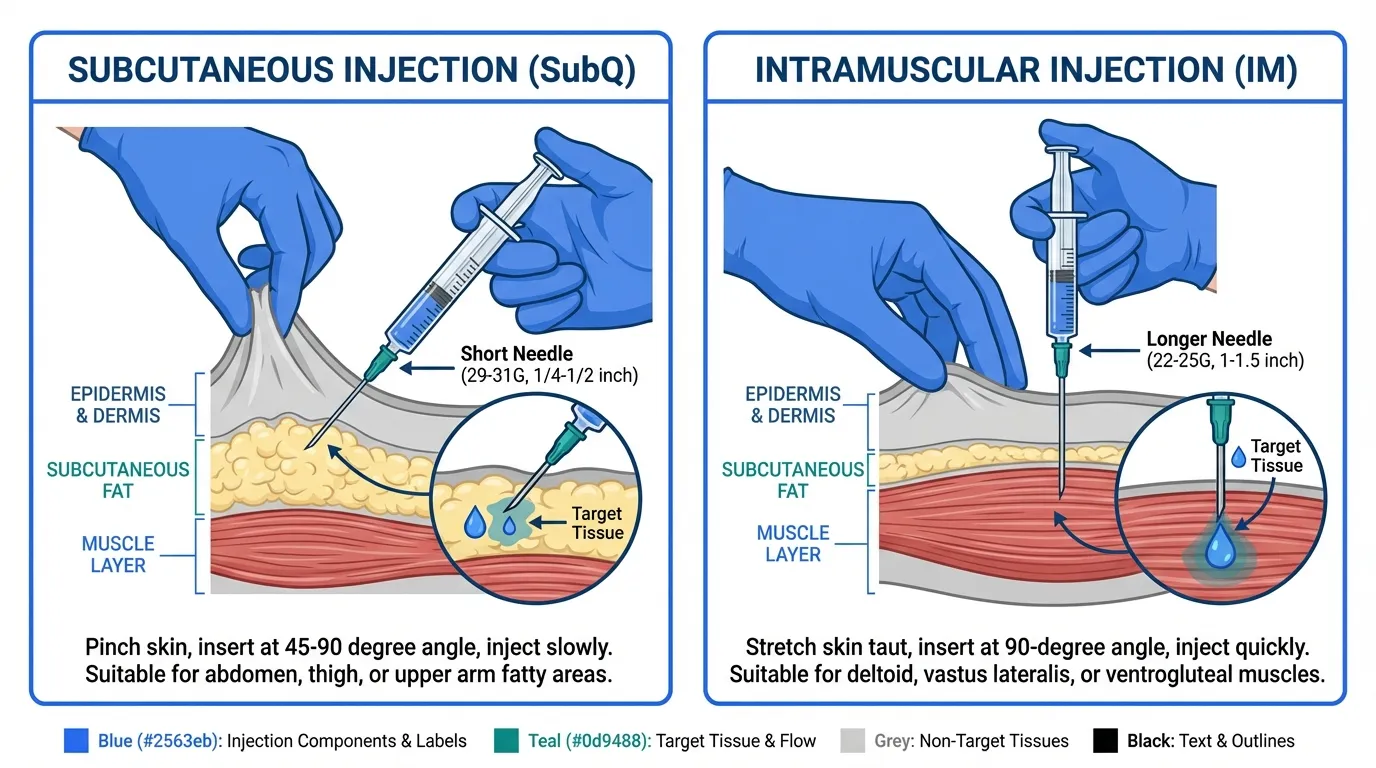
A subcutaneous injection delivers the peptide into the layer of fat and connective tissue (the hypodermis) that lies just beneath the skin and above the muscle. The needle penetrates only 4-8 mm into the tissue.
How Absorption Works#
When a peptide is injected subcutaneously, it enters a tissue with relatively low blood flow compared to muscle. The peptide is absorbed gradually as it diffuses from the injection site into nearby capillaries and lymphatic vessels.
This results in:
- Slower absorption compared to intramuscular injection
- More sustained blood levels with a flatter pharmacokinetic curve
- Longer time to peak concentration (Tmax is typically delayed)
- Predictable, consistent absorption when proper technique is used
Injection Technique#
- Clean the injection site with an alcohol swab
- Pinch a fold of skin to lift the subcutaneous tissue away from the muscle
- Insert the needle at a 45-90 degree angle (90 degrees for longer needles in areas with adequate fat; 45 degrees for thinner areas)
- Inject slowly and steadily
- Release the skin pinch after removing the needle
- Do not massage the site (this can alter absorption rates)
Common Injection Sites#
| Site | Location | Notes |
|---|---|---|
| Abdomen | 2+ inches from the navel, avoiding the belt line | Most common site; large surface area for rotation |
| Outer thigh | Front/outer upper thigh | Easy for self-injection; good fat layer |
| Upper arm | Back of the upper arm | May require assistance for self-injection |
| Lower back / flank | Above the hip, lateral to the spine | Alternative site for rotation |
Site rotation is important to prevent lipodystrophy (changes in fat tissue at frequently used injection sites). Rotate between different areas and leave at least 1 inch between consecutive injection locations within the same area.
Advantages of SubQ Injection#
- Ease of self-administration: Simple technique with short needles
- Less painful: Smaller gauge needles (29-31G) and shallow depth
- Lower risk of hitting blood vessels or nerves: The subcutaneous layer has fewer large vessels
- Consistent absorption: Predictable pharmacokinetics for most peptides
- Suitable for most peptide volumes: Standard volumes of 0.1-1.0 mL
Limitations of SubQ Injection#
- Volume limitation: Generally limited to 1-2 mL per injection site
- Slower onset: Not ideal when rapid absorption is needed
- Injection site reactions: Some peptides may cause local redness, swelling, or itching
- Variable absorption in different body compositions: Very lean individuals may have limited subcutaneous tissue in some areas
Intramuscular Injection (IM)#
What It Is#
An intramuscular injection delivers the peptide directly into muscle tissue, which has a rich blood supply. The needle must penetrate through the skin, subcutaneous fat, and fascia to reach the muscle.
How Absorption Works#
Muscle tissue has a much higher blood flow than subcutaneous tissue, particularly during and after physical activity. This means:
- Faster absorption compared to subcutaneous injection
- Higher peak concentrations (Cmax) with a sharper pharmacokinetic curve
- Shorter time to peak (Tmax is earlier)
- Variable absorption depending on the specific muscle used and activity level
Injection Technique#
- Clean the injection site with an alcohol swab
- Stretch the skin taut over the muscle (or use the Z-track technique to prevent leakage)
- Insert the needle at a 90 degree angle with a quick, dart-like motion
- Use a longer needle (1-1.5 inches / 25-38 mm) to reach the muscle
- Aspirate briefly to check for blood (indicating a blood vessel)
- Inject slowly and steadily
- Remove the needle and apply light pressure
Common Injection Sites#
| Site | Muscle | Notes |
|---|---|---|
| Deltoid | Upper arm (deltoid muscle) | Small muscle; limited to smaller volumes (1-2 mL) |
| Vastus lateralis | Outer thigh | Large muscle; suitable for larger volumes |
| Ventrogluteal | Hip (gluteus medius) | Preferred for larger volumes; fewer nerves and vessels |
| Dorsogluteal | Upper outer buttock | Traditional site but higher risk of sciatic nerve injury |
Advantages of IM Injection#
- Faster absorption: Useful when rapid onset is desired
- Larger volumes: Can accommodate 2-5 mL per injection site depending on the muscle
- Depot effect: Some formulations create a depot in the muscle for extended release
- Suitable for oil-based preparations: Viscous solutions inject more easily into muscle
Limitations of IM Injection#
- More painful: Larger needles and deeper penetration
- Harder to self-administer: Some sites (gluteal) are difficult to reach alone
- Higher risk: Greater chance of hitting blood vessels, nerves, or causing hematomas
- Requires longer needles: 1-1.5 inch needles depending on body composition
- Variable absorption with exercise: Physical activity increases muscle blood flow, potentially altering absorption
Head-to-Head Comparison#
| Factor | Subcutaneous | Intramuscular |
|---|---|---|
| Needle gauge | 27-31G (thin) | 22-25G (thicker) |
| Needle length | 6-12 mm (1/4 - 1/2 inch) | 25-38 mm (1 - 1.5 inch) |
| Injection angle | 45-90 degrees | 90 degrees |
| Absorption rate | Slower, more gradual | Faster, sharper peak |
| Time to peak | Longer | Shorter |
| Pain level | Lower | Higher |
| Self-injection ease | Easy | Moderate (site-dependent) |
| Max volume per site | 1-2 mL | 2-5 mL |
| Site reaction risk | Moderate (local) | Lower (local) but higher (systemic) |
Which Route for Which Peptides?#
Peptides Typically Given Subcutaneously#
The vast majority of research peptides and FDA-approved peptide drugs use the subcutaneous route:
- GLP-1 receptor agonists: Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are exclusively subcutaneous
- Growth hormone secretagogues: Ipamorelin, sermorelin, GHRP-2, and CJC-1295 are typically administered SubQ
- Healing peptides: BPC-157 and TB-500 are commonly injected SubQ, often near the site of injury
- Growth hormone: Pharmaceutical HGH is administered subcutaneously
- Immune peptides: Thymosin Alpha-1 is administered subcutaneously in its approved international formulations
Peptides Sometimes Given Intramuscularly#
Some peptides use the IM route in specific contexts:
- GnRH agonists: Triptorelin depot formulations (Trelstar) are given as intramuscular injections for sustained release
- HCG: HCG can be administered either SubQ or IM depending on the formulation and clinical indication
- Gonadorelin: Gonadorelin may be given IM for diagnostic purposes
- B12 and other larger-volume injections: Often given IM due to volume requirements
The BPC-157 Localized Injection Approach#
BPC-157 is notable for a practice that is common in the research community: injecting subcutaneously as close to the site of injury as possible. The rationale is that localized injection delivers the highest concentration of peptide to the target tissue. While this approach is biologically plausible, it has not been systematically compared to distant-site injection in controlled studies.
Other Administration Routes#
While subcutaneous and intramuscular are the most common injectable routes, some peptides use alternative administration methods:
| Route | Examples | Notes |
|---|---|---|
| Oral | Semaglutide (Rybelsus) | Requires absorption enhancer (SNAC); rare for peptides due to GI degradation |
| Intranasal | Semax, Selank, Oxytocin | Bypasses GI tract; may allow CNS delivery |
| Topical | GHK-Cu creams and serums | Limited to local/cosmetic applications |
| Intravenous | Some clinical research settings | Rapid onset; requires medical setting |
| Sublingual | Some research peptides | Limited bioavailability data for most peptides |
Practical Tips for Injectable Peptides#
Reducing Injection Pain#
- Use the smallest gauge needle practical for the volume (29-31G for SubQ)
- Allow alcohol to dry completely before inserting the needle
- Inject at room temperature -- cold solutions can cause more discomfort
- Insert the needle quickly with a smooth, confident motion
- Inject the solution slowly
- Apply gentle pressure (not massage) after removal
- Rotate injection sites consistently
When to Seek Guidance#
Consult a healthcare professional if you experience:
- Persistent redness, swelling, or warmth at injection sites (possible infection)
- Hard lumps that do not resolve within a few days
- Significant bruising or hematoma formation
- Any signs of allergic reaction (hives, difficulty breathing, facial swelling)
For detailed information on peptide preparation and reconstitution before injection, see our reconstitution guide. For dose calculations, use our dosing calculator.
Key Takeaways#
-
Subcutaneous injection is the standard route for most peptides. It offers easier self-administration, less pain, lower risk, and predictable absorption.
-
Intramuscular injection provides faster absorption but is more painful and carries higher risk. It is used for specific formulations that require it, such as depot preparations.
-
The choice of route affects pharmacokinetics. SubQ provides slower, more sustained absorption while IM produces faster peaks. This can impact both efficacy and side effects.
-
Injection site rotation is important for both routes to prevent tissue damage from repeated injections in the same location.
-
Most FDA-approved peptide drugs specify their route. Always follow the prescribed administration route -- do not switch between SubQ and IM without clinical guidance.
-
Proper technique matters. Correct needle selection, injection angle, and aseptic practices reduce pain, minimize complications, and ensure reliable peptide delivery.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:

{kind=link}
Frequently Asked Questions About Subcutaneous vs Intramuscular Peptide Injection: What Research Shows
What does this article cover?
Subcutaneous vs intramuscular peptide injection compared. Covers absorption, technique, site selection, and preferred routes by peptide. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers BPC-157, Semaglutide, Ipamorelin. Key context: BPC-157 (Commonly administered via subcutaneous injection near the site of injury, illustrating localized ...); Semaglutide (FDA-approved GLP-1 agonist administered exclusively via subcutaneous injection, demonstrating sta...); Ipamorelin (Growth hormone secretagogue typically administered subcutaneously, representing standard peptide ...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Subcutaneous vs Intramuscular Peptide Injection: What Research Shows." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Commonly administered via subcutaneous injection near the site of injury, illustrating localized .... FDA-approved GLP-1 agonist administered exclusively via subcutaneous injection, demonstrating sta.... Growth hormone secretagogue typically administered subcutaneously, representing standard peptide .... These takeaways are based on the research data available at the time of publication.
What is BPC-157 and why is it significant?
BPC-157 is a peptide discussed in this article because: Commonly administered via subcutaneous injection near the site of injury, illustrating localized injection strategy. For a complete profile of BPC-157, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.
Understanding Peptide Side Effects: A Comprehensive Safety Guide
A thorough, evidence-based guide to peptide side effects by category — covering GLP-1 agonists, GH secretagogues, tissue repair peptides, and melanocortins — with serious risk flags, drug interactions, monitoring recommendations, and guidance on when to stop.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.
You Might Also Like
Related content you may find interesting