CJC-1295 DAC vs CJC-1295 No DAC: GHRH Analog Comparison
CJC-1295 DAC vs No DAC compared: long-acting weekly dosing vs pulsatile GH release, pharmacokinetics, and research evidence.
Verdict at a Glance
CJC-1295 DAC and CJC-1295 without DAC share an identical core GHRH agonist sequence but produce fundamentally different pharmacokinetic profiles. The DAC version offers weekly dosing convenience and sustained GH/IGF-1 elevation, supported by Phase 1-2 clinical data. The non-DAC version (Mod GRF 1-29) produces physiological pulsatile GH release with rapid clearance and better safety reversibility, but requires multiple daily injections. The choice depends on whether sustained GH axis stimulation or physiological pulsatile signaling is the research priority.
| Best for | Pick | Why |
|---|---|---|
| Convenience and sustained GH/IGF-1 elevation | CJC-1295 DAC | Weekly dosing with demonstrated sustained IGF-1 elevation for 6-14 days per dose; Phase 1-2 clinical PK/PD data available |
| Physiological pulsatile GH release | CJC-1295 without DAC | 30-minute half-life produces discrete GH pulses that closely mimic natural GHRH signaling; rapid clearance preserves hormonal cycling |
| Combination with GHRP peptides | CJC-1295 without DAC | Synergistic GH release when co-administered with ipamorelin or GHRP-6 at matched timing; pulsatile release allows temporal coordination |
| Minimal injection burden | CJC-1295 DAC | Single weekly injection versus 2-3 daily injections; substantially lower compliance burden for sustained research protocols |
| Category | CJC-1295 DAC | CJC-1295 without DAC | Advantage |
|---|---|---|---|
| Mechanism of Action | GHRH-R agonist with Drug Affinity Complex enabling albumin binding; sustained receptor activation over 6-8 days; continuous GH axis stimulation modulated by somatostatin cycling | Same GHRH-R agonist core (29aa with 4 DPP-IV resistant substitutions); 30-minute half-life produces discrete GH pulses mimicking physiological GHRH signaling; rapid clearance after each dose | Comparable |
| Research Evidence | Phase 1-2 clinical trial data from ConjuChem; published PK/PD studies in JCEM demonstrating sustained IGF-1 elevation; development discontinued before Phase 3 | Evidence derives from broader GHRH analog literature and CJC-1295 structure-activity studies; no independent clinical development separate from DAC program; preclinical status | CJC-1295 DAC |
| Side Effect Profile | Long half-life means adverse effects persist for days; theoretical risks of sustained GH/IGF-1 elevation include insulin resistance, fluid retention, joint pain; cannot rapidly reverse effects | Short half-life allows rapid clearance if adverse effects occur; transient GH elevation limits duration of any side effects; more physiological on/off pattern | CJC-1295 without DAC |
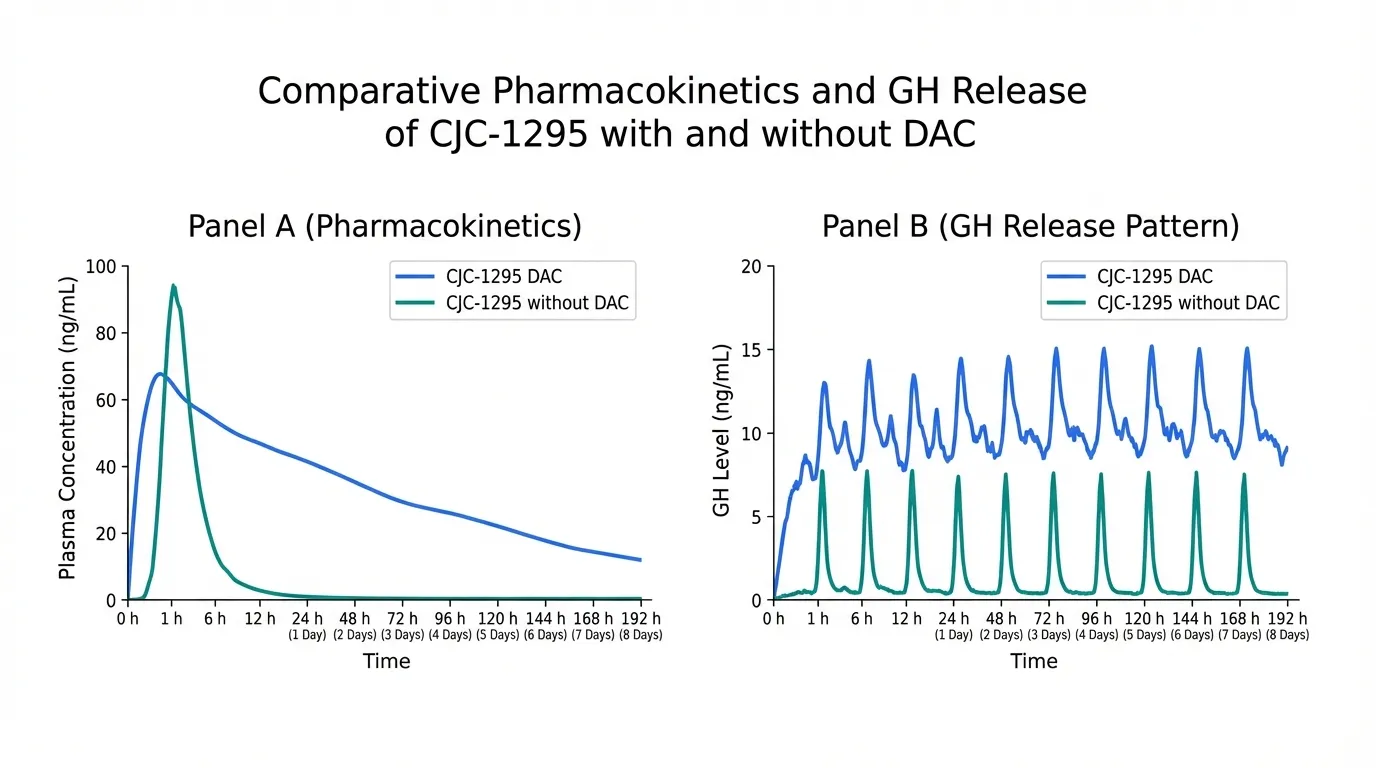
| GH Release Pattern | Sustained elevation of GH and IGF-1 for 6-14 days after single dose; amplifies all GH pulses including sleep-associated peaks; 2-10 fold GH increase, 1.5-3 fold IGF-1 increase | Discrete 1-2 hour GH pulses per injection; closely mimics endogenous pulsatile GH secretion; GH returns to baseline between doses; synergistic with GHRP co-administration | Comparable |
| Dosing Convenience | Once-weekly subcutaneous injection; simple dosing schedule; no timing requirements relative to meals or sleep | Requires 2-3 daily injections; timing matters (somatostatin troughs preferred); typically dosed pre-sleep and morning; significant injection burden | CJC-1295 DAC |

Introduction#
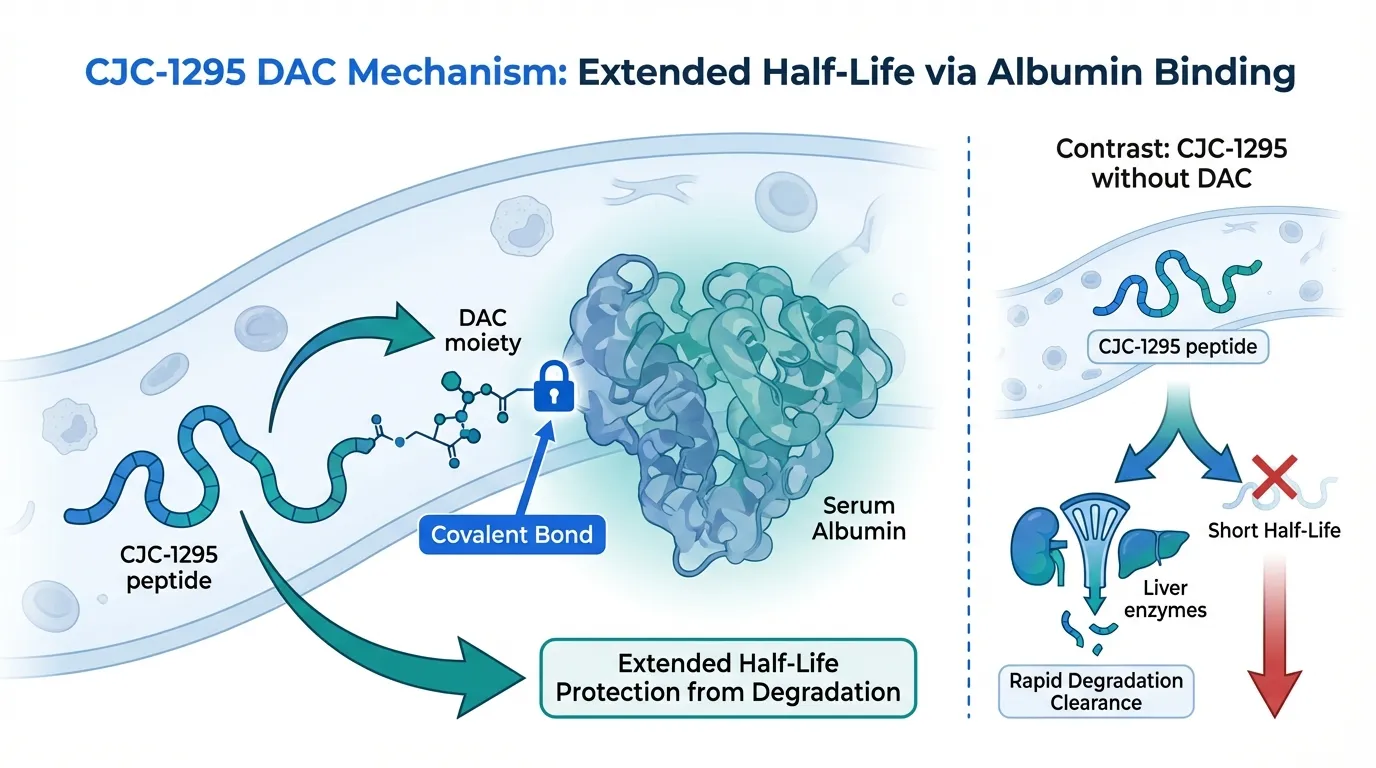
CJC-1295 DAC and CJC-1295 without DAC (Mod GRF 1-29) are two forms of the same GHRH receptor agonist that differ by a single molecular modification with dramatic pharmacokinetic consequences. The DAC (Drug Affinity Complex) moiety enables albumin binding, extending the half-life from approximately 30 minutes to 6-8 days. This single change transforms the compound from a pulsatile GH stimulator into a sustained-release GH axis activator, fundamentally altering its research applications and physiological effects.
Quick Comparison#
| Feature | CJC-1295 DAC | CJC-1295 without DAC |
|---|---|---|
| Structure | 30 amino acids + DAC, 3.6 kDa | 29 amino acids, 3.4 kDa |
| Half-Life | 6-8 days | ~30 minutes |
| GH Pattern | Sustained elevation | Discrete pulsatile release |
| Dosing | Once weekly | 2-3 times daily |
| IGF-1 Effect | 1.5-3x elevation, sustained 6-14 days | Transient elevation, returns to baseline |
| Clinical Data | Phase 1-2 trials (ConjuChem) | Preclinical / GHRH analog literature |
| Research Status | Discontinued before Phase 3 | Preclinical |
| WADA Status | Prohibited | Prohibited |
Mechanism of Action Comparison#
CJC-1295 DAC#
CJC-1295 DAC is a 30-amino acid synthetic analog of GHRH that incorporates the Drug Affinity Complex, a maleimido derivative of lysine that forms a covalent bond with serum albumin after subcutaneous injection. This albumin conjugation protects the peptide from DPP-IV degradation and reduces renal clearance, extending the half-life from minutes to 6-8 days.
The peptide activates the GHRH receptor (GHRH-R) on anterior pituitary somatotrophs, triggering Gs-cAMP-PKA signaling that stimulates both GH gene transcription and release of stored GH granules. Because receptor engagement persists for days, CJC-1295 DAC amplifies all natural GH pulses throughout the dosing interval. Somatostatin still modulates GH release, so some pulsatility is preserved, but the overall GH and IGF-1 levels are continuously elevated above baseline.
Clinical PK/PD data demonstrate dose-dependent GH increases (2-10 fold) and IGF-1 elevation (1.5-3 fold) persisting for up to 6-14 days after a single subcutaneous dose.
CJC-1295 without DAC (Mod GRF 1-29)#
CJC-1295 without DAC, commonly called Mod GRF 1-29, consists of the first 29 amino acids of human GHRH with four strategic substitutions (D-Ala2, Gln8, Ala15, Leu27) that confer resistance to DPP-IV cleavage while preserving full GHRH-R agonist activity. Without the DAC moiety, there is no albumin binding and the peptide is cleared within approximately 30 minutes.
The mechanism at the receptor level is identical to CJC-1295 DAC: GHRH-R activation, Gs-cAMP-PKA signaling, and GH release. The critical difference is temporal. Each injection produces a discrete 1-2 hour GH pulse followed by return to baseline, closely mimicking the endogenous pattern of GHRH-stimulated pulsatile GH secretion.
This pulsatile pattern is important because GH physiology is inherently pulsatile. The amplitude and frequency of GH pulses, not just mean GH levels, influence downstream metabolic effects including hepatic IGF-1 production, lipolysis, and protein synthesis. Mod GRF 1-29 also shows strong synergy with ghrelin-mimetic peptides (ipamorelin, GHRP-6) when co-administered, as GHRH and ghrelin act through complementary pathways on somatotrophs.
Evidence and Research Comparison#
CJC-1295 DAC Research#
CJC-1295 DAC has the stronger clinical evidence base of the two. ConjuChem Biotechnologies conducted Phase 1 and Phase 2 clinical trials that demonstrated:
- Dose-dependent PK/PD: Single subcutaneous doses produced sustained, dose-proportional GH and IGF-1 elevation published in the Journal of Clinical Endocrinology and Metabolism
- Weekly dosing feasibility: Multiple weekly doses over 4-8 weeks showed progressive IGF-1 elevation without tachyphylaxis
- Safety: Generally well-tolerated at doses up to 120 mcg/kg
- Development status: The clinical program was discontinued before Phase 3 completion; the compound did not proceed to FDA approval
CJC-1295 without DAC Research#
Mod GRF 1-29 does not have an independent clinical development program. Its evidence base derives from:
- Structure-activity studies: The four amino acid modifications were characterized in research demonstrating improved metabolic stability with preserved receptor activity
- GHRH analog literature: Extensive research on native GRF(1-29) (sermorelin, which had prior FDA approval) provides pharmacological context for the modified sequence
- Combination studies: Preclinical and observational data on synergistic GH release when combined with ghrelin-mimetic peptides
- Research status: Remains at preclinical status with no independent regulatory filings
Side Effects and Safety Comparison#
CJC-1295 DAC Side Effects#
- Injection site reactions: Redness and swelling reported in clinical trials
- Sustained GH/IGF-1 elevation risks: Insulin resistance, fluid retention, joint pain, carpal tunnel-like symptoms are theoretical with chronic use
- Irreversibility: The 6-8 day half-life means any adverse effects persist for days to weeks after discontinuation
- Cancer consideration: Sustained IGF-1 elevation carries theoretical concern for cell proliferation; contraindicated with active malignancy
CJC-1295 without DAC Side Effects#
- Injection site reactions: Similar to DAC form but more frequent due to multiple daily injections
- Transient effects: Any GH-related side effects resolve within hours as the peptide clears
- Rapid reversibility: Short half-life provides inherent safety advantage; stopping the compound produces rapid return to baseline
- Lower sustained exposure: Less theoretical concern for chronic IGF-1-related risks due to intermittent rather than continuous elevation
Dosing and Administration Comparison#
CJC-1295 DAC Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection |
| Frequency | Once weekly |
| Clinical trial doses | 30-120 mcg/kg per week |
| Research doses | Typically 2 mg once weekly |
| Timing | No specific timing requirements |
| Reconstitution | Lyophilized powder with bacteriostatic water |
CJC-1295 without DAC Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection |
| Frequency | 2-3 times daily |
| Research doses | 100-300 mcg per injection |
| Optimal timing | Pre-sleep and fasted morning (somatostatin troughs) |
| Combination dosing | Often co-administered with ipamorelin (100-300 mcg) |
| Reconstitution | Lyophilized powder with bacteriostatic water |
Use Case Recommendations#
Choose CJC-1295 DAC When:#
- Dosing convenience is a priority and weekly injection is preferred over multiple daily doses
- Sustained IGF-1 elevation is the research goal rather than pulsatile GH release
- Clinical-grade evidence is important, as Phase 1-2 PK/PD data are available
- Standalone use without GHRP combination is planned
Choose CJC-1295 without DAC When:#
- Physiological GH pulsatility is the goal, mimicking natural GHRH signaling
- Combination protocols with ipamorelin or GHRP-6 are planned, where temporal synchronization matters
- Safety reversibility is prioritized, with rapid clearance if adverse effects occur
- Pulsatile signaling research rather than sustained axis stimulation is the focus
Can They Be Combined?#
Combining CJC-1295 DAC with CJC-1295 without DAC is pharmacologically redundant, as both activate the same GHRH receptor. The DAC form already provides continuous receptor stimulation, making additional pulsatile GHRH agonism unlikely to add benefit. This combination is not studied and not recommended.
The more relevant combination question is CJC-1295 without DAC combined with a ghrelin-mimetic peptide like ipamorelin. GHRH and ghrelin act through complementary receptors (GHRH-R and GHS-R1a) on somatotrophs, producing synergistic GH release that exceeds the effect of either compound alone. This combination is widely used in research settings. CJC-1295 DAC can also theoretically be combined with GHRPs, but the sustained nature of DAC-mediated signaling makes precise timing coordination less meaningful.
For related GHRH analog comparisons, see our profiles on sermorelin and our sermorelin vs tesamorelin comparison.
Verdict#
CJC-1295 DAC and CJC-1295 without DAC represent the same pharmacological tool with different pharmacokinetic delivery. CJC-1295 DAC offers convenience and sustained GH/IGF-1 elevation backed by Phase 1-2 clinical data, but sacrifices physiological pulsatility and carries irreversibility risk from its long half-life. Mod GRF 1-29 preserves the natural pulsatile GH pattern and offers rapid safety reversibility, but requires multiple daily injections and has weaker clinical evidence.
Neither compound has been FDA-approved. Both are prohibited by WADA. The choice between them reflects a fundamental pharmacological trade-off between sustained convenience and physiological fidelity. Explore our half-life comparison tool to visualize how these half-life differences affect dosing schedules.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Convenience and sustained GH/IGF-1 elevation
CJC-1295 DAC
Weekly dosing with demonstrated sustained IGF-1 elevation for 6-14 days per dose; Phase 1-2 clinical PK/PD data available
Physiological pulsatile GH release
CJC-1295 without DAC
30-minute half-life produces discrete GH pulses that closely mimic natural GHRH signaling; rapid clearance preserves hormonal cycling
Combination with GHRP peptides
CJC-1295 without DAC
Synergistic GH release when co-administered with ipamorelin or GHRP-6 at matched timing; pulsatile release allows temporal coordination
Minimal injection burden
CJC-1295 DAC
Single weekly injection versus 2-3 daily injections; substantially lower compliance burden for sustained research protocols
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About CJC-1295 DAC vs CJC-1295 No DAC: GHRH Analog Comparison
Which is better, CJC-1295 DAC or CJC-1295 without DAC?
CJC-1295 DAC and CJC-1295 without DAC share an identical core GHRH agonist sequence but produce fundamentally different pharmacokinetic profiles. The DAC version offers weekly dosing convenience and sustained GH/IGF-1 elevation, supported by Phase 1-2 clinical data. The non-DAC version (Mod GRF 1-29) produces physiological pulsatile GH release with rapid clearance and better safety reversibility, but requires multiple daily injections. The choice depends on whether sustained GH axis stimulati... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between CJC-1295 DAC and CJC-1295 without DAC?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to CJC-1295 DAC; Side Effect Profile: advantage goes to CJC-1295 without DAC. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider CJC-1295 DAC over CJC-1295 without DAC?
For the scenario of "Convenience and sustained GH/IGF-1 elevation," research data suggests CJC-1295 DAC may be more relevant. Weekly dosing with demonstrated sustained IGF-1 elevation for 6-14 days per dose; Phase 1-2 clinical PK/PD data available. This is based on currently available evidence and individual circumstances may differ.
How do CJC-1295 DAC and CJC-1295 without DAC differ in their mechanisms of action?
CJC-1295 DAC: GHRH-R agonist with Drug Affinity Complex enabling albumin binding; sustained receptor activation over 6-8 days; continuous GH axis stimulation modulated by somatostatin cycling. CJC-1295 without DAC: Same GHRH-R agonist core (29aa with 4 DPP-IV resistant substitutions); 30-minute half-life produces discrete GH pulses mimicking physiological GHRH signaling; rapid clearance after each dose.
Which has fewer side effects, CJC-1295 DAC or CJC-1295 without DAC?
In terms of side effects and tolerability, the advantage goes to CJC-1295 without DAC. CJC-1295 DAC: Long half-life means adverse effects persist for days; theoretical risks of sustained GH/IGF-1 elevation include insulin resistance, fluid retentio.... CJC-1295 without DAC: Short half-life allows rapid clearance if adverse effects occur; transient GH elevation limits duration of any side effects; more physiological on/....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.