Ipamorelin vs CJC-1295 vs Sermorelin: Which GH Peptide Stack Works Best?

Introduction#
Three peptides dominate the growth hormone secretagogue conversation: ipamorelin, CJC-1295, and sermorelin. They are frequently discussed together because they represent the core building blocks of GH peptide protocols -- yet they work through different mechanisms and serve different roles.
Understanding how these three compounds compare -- and more importantly, how they complement each other -- is essential for evaluating GH peptide research. This article provides a detailed three-way comparison covering mechanisms, pharmacokinetics, clinical evidence, side effects, and the rationale behind combining them.
For a broader overview of all GH secretagogues including GHRP-2 and hexarelin, see Top 6 Growth Hormone Secretagogues Compared. For a beginner-friendly introduction, see Growth Hormone Peptides for Beginners.
Mechanism Comparison: Two Pathways, One Goal#
The most important distinction between these peptides is which receptor pathway they activate.
Ipamorelin: The Ghrelin Pathway (GHS-R1a)#
Ipamorelin is a pentapeptide that selectively activates the growth hormone secretagogue receptor (GHS-R1a), also known as the ghrelin receptor. When this receptor is activated, it triggers an intracellular signaling cascade that amplifies growth hormone release from pituitary somatotrophs.
What makes ipamorelin unique among ghrelin-pathway peptides is its selectivity. Clinical studies confirm it stimulates GH release without significantly affecting cortisol, prolactin, ACTH, FSH, LH, or TSH. This stands in contrast to other GHS-R1a agonists like GHRP-2 and hexarelin, which activate the same receptor but produce broader hormonal changes.
Sermorelin and CJC-1295: The GHRH Pathway#
Both sermorelin and CJC-1295 (No DAC) activate the growth hormone-releasing hormone receptor (GHRH-R) on pituitary somatotrophs. They are essentially doing the same job -- stimulating GH synthesis and release through GHRH signaling -- but with different pharmacokinetic profiles.
Sermorelin is a synthetic analog of the first 29 amino acids of endogenous GHRH (GRF 1-29). It faithfully mimics the natural GHRH signal but is rapidly degraded by dipeptidyl peptidase-IV (DPP-IV) and other enzymes, giving it a half-life of only 10-20 minutes.
CJC-1295 (No DAC), also called Modified GRF 1-29, is sermorelin with four amino acid substitutions at positions 2, 8, 15, and 27. These modifications protect the peptide from enzymatic degradation, extending its effective half-life to approximately 30+ minutes while preserving the same GHRH-receptor activation.
Sermorelin vs. CJC-1295: The GHRH Analog Showdown#
Since sermorelin and CJC-1295 (No DAC) both work through the GHRH receptor, the comparison between them comes down to pharmacokinetics, clinical evidence, and practical considerations.
Pharmacokinetics#
| Parameter | Sermorelin | CJC-1295 (No DAC) | CJC-1295 DAC |
|---|---|---|---|
| Half-life | ~10-20 minutes | ~30+ minutes | ~6-8 days |
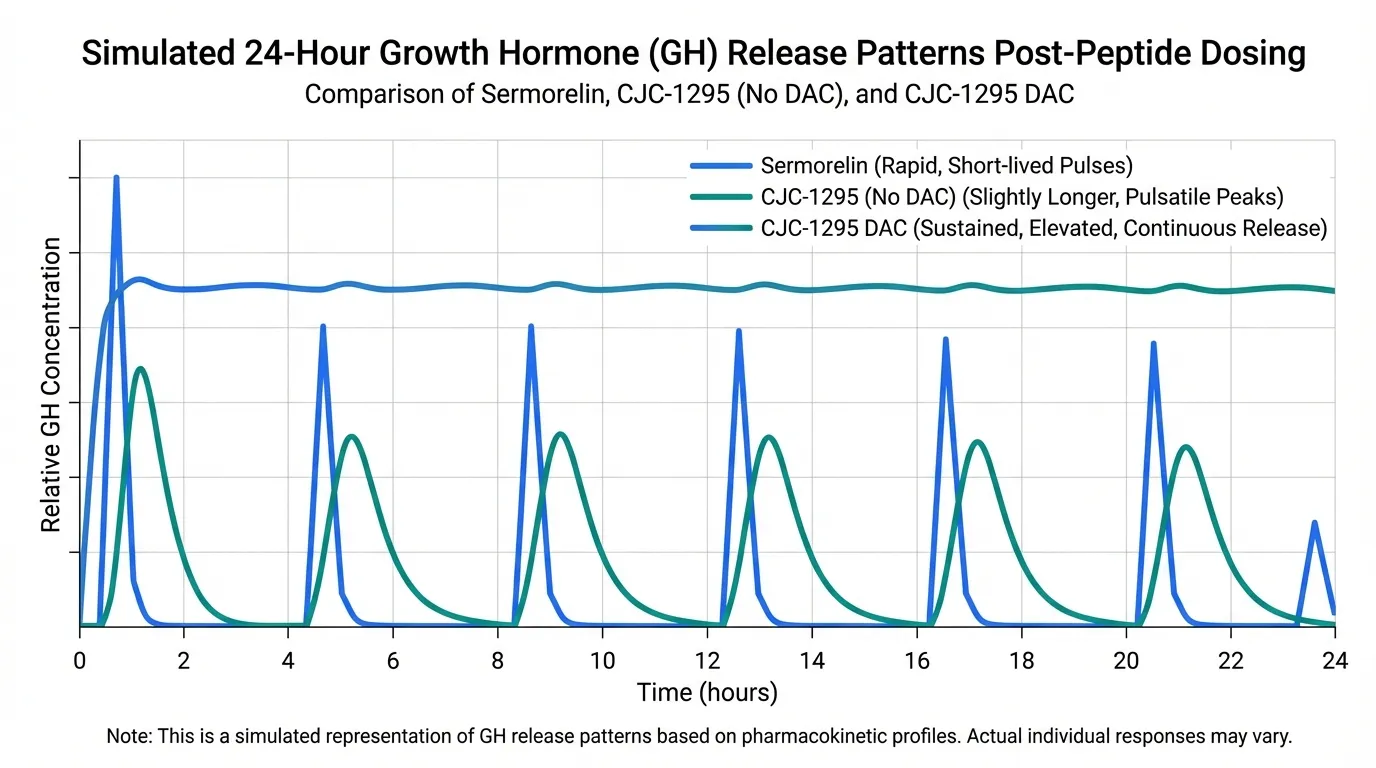
| GH Release Pattern | Pulsatile | Pulsatile | Sustained/continuous |
| DPP-IV Resistance | Low | High | High |
| Albumin Binding | No | No | Yes (via DAC) |
| Dosing Frequency | Multiple daily or before bed | 1-2x daily | 1-2x weekly |
Clinical Evidence#
Sermorelin has the stronger clinical evidence base. It was previously FDA-approved as Geref and has extensive published data from human trials in both children and adults with GH deficiency. Studies in aging adults demonstrated increased GH secretion and improved IGF-1 levels. Its withdrawal from the market was for commercial reasons, not safety or efficacy concerns.
CJC-1295 (No DAC) has more limited direct clinical trial data. Its mechanism of action through the GHRH receptor is well-established, but most of the published research focuses on the original GRF 1-29 (sermorelin) rather than the modified version. The pharmacokinetic advantage of improved enzymatic resistance is supported by preclinical data.
The DAC Question#
CJC-1295 with DAC (Drug Affinity Complex) binds to albumin, extending its half-life to approximately 6-8 days. While this offers dosing convenience, it creates sustained, non-pulsatile GH elevation that does not mimic the body's natural secretion pattern.
Most researchers favor the No DAC version for several reasons:
- Preserves pulsatile GH release, which is considered more physiologically appropriate
- Avoids potential receptor downregulation from continuous GH stimulation
- Allows precise timing of GH pulses (e.g., before sleep when natural GH secretion peaks)
- Better studied in combination with ghrelin-pathway peptides
Ipamorelin vs. Sermorelin: Different Pathways, Different Strengths#
Comparing ipamorelin to sermorelin is not an apples-to-apples comparison -- they work through entirely different receptor systems. The question is not which is "better" but which pathway best serves the research objective.
| Feature | Ipamorelin | Sermorelin |
|---|---|---|
| Receptor | GHS-R1a (ghrelin) | GHRH-R |
| Mechanism | Amplifies GH release signal | Directly triggers GH synthesis and release |
| GH Release Potency | Moderate | Moderate |
| Selectivity | Very high | High |
| Cortisol Effect | Minimal | Minimal |
| Prolactin Effect | Minimal | Minimal |
| Appetite Stimulation | Low | None |
| Half-Life | ~2 hours | ~10-20 minutes |
| FDA History | Never approved | Previously approved (Geref) |
| Best Role | GHRP component of combos | Standalone or GHRH component |
The key takeaway is that these two peptides are complementary rather than competitive. Ipamorelin amplifies GH release through the ghrelin receptor, while sermorelin triggers GH synthesis through the GHRH receptor. Research consistently shows that activating both pathways simultaneously produces synergistic effects.
For a detailed head-to-head analysis, see Ipamorelin vs Sermorelin.
Ipamorelin vs. CJC-1295: The Stack Components#
When ipamorelin and CJC-1295 (No DAC) are discussed together, it is usually in the context of combining them rather than choosing between them. This is the most commonly studied GH peptide combination, and the rationale is straightforward:
- CJC-1295 (No DAC) primes pituitary somatotrophs through GHRH-receptor activation, increasing GH synthesis capacity
- Ipamorelin amplifies the release signal through GHS-R1a activation
- Simultaneous activation of both receptors produces synergistic GH output exceeding the sum of individual effects
This synergy has been demonstrated in research combining GHRH analogs with ghrelin-receptor agonists. The CJC-1295 + ipamorelin pairing specifically leverages CJC-1295's improved stability over sermorelin and ipamorelin's superior selectivity over GHRP-2 or hexarelin.
For a deep dive on this combination, see CJC-1295 and Ipamorelin Stack.
Three-Way Comparison Table#
| Feature | Ipamorelin | CJC-1295 (No DAC) | Sermorelin |
|---|---|---|---|
| Pathway | Ghrelin (GHS-R1a) | GHRH | GHRH |
| Half-Life | ~2 hours | ~30+ minutes | ~10-20 minutes |
| GH Release | Moderate, dose-dependent | Moderate | Moderate |
| Selectivity | Very high | High | High |
| Cortisol/Prolactin | Minimal | Minimal | Minimal |
| Appetite Effect | Low | None | None |
| Tachyphylaxis Risk | Low | Low | Low |
| Clinical Evidence | Phase 2 trials | Limited direct trials | Extensive (formerly FDA-approved) |
| Primary Role | GHRP component in stacks | GHRH component in stacks | Standalone or GHRH component |
| DPP-IV Resistance | N/A (different pathway) | High | Low |
| Administration | Subcutaneous injection | Subcutaneous injection | Subcutaneous injection |
| Regulatory Status | Investigational | Investigational | Withdrawn (commercial) |
Where Tesamorelin Fits#
Tesamorelin merits discussion as the clinical benchmark for GHRH-pathway secretagogues. As the only FDA-approved GH secretagogue (marketed as Egrifta for HIV-associated lipodystrophy), it provides Phase 3 trial data that other GHRH analogs lack.
Key clinical results include:
- Approximately 15-18% reduction in visceral adipose tissue over 26 weeks vs. placebo
- Improvements in verbal memory and executive function in aging adults (separate study)
- Well-characterized side effect profile from large randomized controlled trials
Tesamorelin works through the same GHRH receptor as sermorelin and CJC-1295 but is only available by prescription for its approved indication. For researchers who value the highest standard of clinical validation, tesamorelin's data set provides the reference point for what GHRH-pathway activation can achieve.
For a direct comparison, see Sermorelin vs Tesamorelin.
Stacking Rationale: Why Combinations Outperform Singles#
The principle behind GH peptide stacking is grounded in receptor biology:
The Synergy Mechanism#
GHRH-receptor activation and GHS-R1a activation converge on the same pituitary somatotroph cells but through different intracellular signaling cascades. GHRH signaling primarily works through the cAMP/PKA pathway, while ghrelin-receptor signaling involves the PLC/IP3/PKC pathway. When both pathways are activated simultaneously, the downstream signals amplify each other, producing a GH release response that is significantly greater than either signal alone.
Common Stack Configurations#
| Stack | GHRH Component | GHRP Component | Notes |
|---|---|---|---|
| CJC-1295 + Ipamorelin | CJC-1295 (No DAC) | Ipamorelin | Most popular combination; clean profile with synergistic release |
| Sermorelin + Ipamorelin | Sermorelin | Ipamorelin | Stronger clinical pedigree for the GHRH component |
| CJC-1295 + GHRP-2 | CJC-1295 (No DAC) | GHRP-2 | Higher GH output but more cortisol/prolactin effects |
| Sermorelin alone | Sermorelin | None | Single-agent approach with established safety data |
| Ipamorelin alone | None | Ipamorelin | Single-agent approach prioritizing selectivity |
Why CJC-1295 (No DAC) + Ipamorelin Dominates#
This specific combination has become the most commonly discussed GH peptide stack because it optimizes for both efficacy and tolerability:
- CJC-1295 (No DAC) provides the GHRH signal with improved stability over sermorelin
- Ipamorelin provides the ghrelin-pathway signal with the cleanest selectivity profile available
- Both components have low tachyphylaxis risk, supporting sustained use
- Neither component significantly affects cortisol, prolactin, or appetite
- Pulsatile GH release is preserved (unlike CJC-1295 DAC combinations)
Practical Considerations#
Administration#
All three peptides are administered via subcutaneous injection. Key differences in timing and frequency stem from their half-lives:
- Ipamorelin (~2 hour half-life): Typically studied with 1-3 administrations per day
- CJC-1295 (No DAC) (~30+ minute half-life): Often administered 1-2x daily, timed to align with natural GH pulse windows
- Sermorelin (~10-20 minute half-life): Short window of action often leads to evening-only administration to coincide with the sleep-associated GH pulse
Storage#
All are lyophilized peptides reconstituted with bacteriostatic water. Standard peptide storage applies: reconstituted vials refrigerated at 2-8 degrees Celsius, used within 4-6 weeks. For detailed reconstitution instructions, see How to Reconstitute Peptides.
Key Takeaways#
- Ipamorelin, CJC-1295 (No DAC), and sermorelin represent two complementary pathways for stimulating growth hormone release -- not three competing alternatives
- Ipamorelin works through the ghrelin receptor (GHS-R1a) with exceptional selectivity, making it the preferred GHRP component in combinations
- Sermorelin and CJC-1295 (No DAC) both activate the GHRH receptor; CJC-1295 offers improved enzymatic resistance while sermorelin has a longer clinical track record
- The CJC-1295 (No DAC) + ipamorelin combination is the most studied stack, leveraging synergistic GH release from simultaneous dual-pathway activation
- CJC-1295 DAC provides dosing convenience but at the cost of non-pulsatile GH elevation, which is considered less physiological
- Tesamorelin serves as the FDA-approved benchmark, demonstrating what GHRH-pathway activation can achieve in rigorous clinical trials
- Single-agent approaches work, but combination protocols consistently produce greater GH output in published research
This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. The peptides discussed are investigational compounds (except tesamorelin for its approved indication) and should only be used under appropriate medical supervision. Always consult a qualified healthcare provider before making decisions about peptide therapy.
Related Resources#

{kind=link}
Frequently Asked Questions About Ipamorelin vs CJC-1295 vs Sermorelin: Which GH Peptide Stack Works Best?
Is CJC-1295 better than sermorelin?
CJC-1295 (No DAC) has a longer effective half-life than sermorelin (approximately 30+ minutes vs. 10-20 minutes) due to amino acid modifications that resist enzymatic degradation. This means it sustains GH stimulation longer per dose. However, sermorelin has a longer clinical track record with extensive human trial data and was previously FDA-approved. Both activate the same GHRH receptor, so the choice depends on whether clinical validation or improved pharmacokinetics is the higher priority.
Why do people combine CJC-1295 with ipamorelin?
CJC-1295 activates the GHRH receptor while ipamorelin activates the ghrelin receptor (GHS-R1a). Research shows that simultaneous activation of both pathways produces synergistic GH release significantly greater than either peptide alone. Ipamorelin is chosen as the ghrelin-pathway component because it is the most selective option, producing minimal cortisol, prolactin, and appetite effects compared to GHRP-2 or hexarelin.
Should I use CJC-1295 with DAC or without DAC?
Most research protocols favor CJC-1295 without DAC (also called Modified GRF 1-29) because it preserves the body's natural pulsatile GH release pattern. The DAC version extends the half-life to 6-8 days, creating continuous GH elevation that does not mimic physiological secretion and may lead to receptor downregulation over time. The No DAC version is also more commonly paired with ipamorelin in combination protocols.
What is the best GH peptide for someone who wants just one compound?
For a single-compound approach, ipamorelin offers the cleanest ghrelin-pathway activation with minimal side effects, while sermorelin provides the strongest clinical evidence base among GHRH-pathway options. Tesamorelin is the only FDA-approved option but requires a prescription and is indicated specifically for HIV-associated lipodystrophy. The choice depends on whether selectivity, clinical validation, or regulatory status is the primary consideration.
How does tesamorelin compare to CJC-1295 and sermorelin?
Tesamorelin is the only FDA-approved GH secretagogue with Phase 3 trial data showing 15-18% visceral fat reduction over 26 weeks. It works through the same GHRH receptor as CJC-1295 and sermorelin but has the strongest regulatory and clinical evidence backing. However, it is only approved for HIV-associated lipodystrophy and requires a prescription, making it less accessible for general research purposes than the other GHRH analogs.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Growth Hormone Peptides for Beginners: Which Secretagogue Is Right for You?
A beginner-friendly guide to growth hormone secretagogues including ipamorelin, sermorelin, CJC-1295, and more. Learn how GH peptides work, compare options, and understand which secretagogue may fit your research goals.
Best Growth Hormone Peptides Ranked: 2026 Evidence-Based Guide
A ranked comparison of 8 growth hormone secretagogues and related peptides — from FDA-approved tesamorelin to IGF-1 LR3 — evaluating each on mechanism of action, clinical evidence strength, key advantages, and known drawbacks.
Peptide Stacking Guide 2026: Best Combinations by Goal
The definitive 2026 guide to peptide stacking organized by goal. Fat loss, muscle growth, healing, anti-aging, and cognitive stacks with evidence levels, dosing timing, and safety considerations.
You Might Also Like
Related content you may find interesting