Semaglutide vs Survodutide: GLP-1 vs Dual Agonist Compared
Semaglutide vs survodutide: GLP-1 agonist vs GLP-1/glucagon dual agonist — weight loss efficacy, MASH potential, and trial data.
Verdict at a Glance
Semaglutide is the established standard with three FDA approvals, massive clinical evidence, and proven cardiovascular outcomes. Survodutide represents the next-generation approach, adding glucagon receptor agonism to GLP-1 signaling for potentially greater weight loss and a unique MASH indication. However, survodutide remains in Phase 3 without regulatory approval. For current clinical use, semaglutide has unmatched validation. For the future of metabolic therapeutics, survodutide's dual mechanism targeting both caloric intake and energy expenditure could prove transformative if Phase 3 data confirm the Phase 2 promise.
| Best for | Pick | Why |
|---|---|---|
| Current obesity treatment with proven efficacy | Semaglutide | FDA-approved as Wegovy with 14.9% weight loss in STEP trials; extensive safety database and real-world prescribing experience |
| MASH/NASH treatment research | Survodutide | Glucagon receptor activation directly targets hepatic steatosis; specific MASH Phase 3 program with histological endpoints |
| Cardiovascular risk reduction in obesity | Semaglutide | SELECT trial demonstrated 20% MACE reduction; only GLP-1 agonist with dedicated cardiovascular outcomes data in obesity population |
| Maximizing weight loss beyond GLP-1 monotherapy | Survodutide | Phase 2 data suggest up to 19% weight loss; dual mechanism targeting both appetite (GLP-1) and energy expenditure (glucagon) for greater net negative energy balance |
| Category | Semaglutide | Survodutide | Advantage |
|---|---|---|---|
| Mechanism of Action | Selective GLP-1 receptor agonist; C18 fatty diacid enables albumin binding for weekly dosing; activates Gs-cAMP-PKA in beta cells and hypothalamic appetite centers; delayed gastric emptying via vagal pathways | Dual GLP-1R/GCGR agonist with glucagon-favoring activity ratio (~4-5x GCGR vs GLP-1R); combines appetite suppression (GLP-1) with increased energy expenditure and hepatic fat oxidation (glucagon); once-weekly SC | Survodutide |
| Research Evidence | FDA-approved for T2D (Ozempic), obesity (Wegovy), and oral (Rybelsus); SUSTAIN, STEP, SELECT, and FLOW trial programs; cardiovascular and renal outcomes data; millions of prescriptions | Phase 3 trials for obesity and MASH (Boehringer Ingelheim); Phase 2 data showing up to 19% body weight reduction; MASH histological improvement data; no regulatory approvals yet | Semaglutide |
| Side Effect Profile | Well-characterized GI side effects (nausea 44%, diarrhea 30%, vomiting 24%); pancreatitis risk; gallbladder events; thyroid C-cell tumor warning; extensive real-world safety data | GI side effects similar to GLP-1 class; glucagon component may increase hepatic glucose output (mitigated by GLP-1); limited safety database from Phase 2; long-term safety profile unknown | Semaglutide |
| Weight Loss Efficacy | STEP 1 trial demonstrated 14.9% mean body weight reduction at 68 weeks (2.4 mg dose); consistent 15-17% range across STEP program | Phase 2 data showed up to 19% body weight reduction; glucagon-mediated energy expenditure provides additional mechanism beyond appetite suppression alone; Phase 3 confirmation pending | Survodutide |
| Liver/MASH Potential | Some evidence for hepatic fat reduction; not specifically developed for MASH; liver effects are secondary to weight loss and metabolic improvement | Specific Phase 3 program for MASH; glucagon receptor activation directly promotes hepatic fat oxidation and reduces steatosis; histological improvement demonstrated in Phase 2 | Survodutide |

Introduction#
Semaglutide and survodutide represent two generations of incretin-based obesity therapeutics. Semaglutide is the established GLP-1 receptor agonist with three FDA approvals and the most comprehensive clinical evidence base in its class. Survodutide adds glucagon receptor agonism to GLP-1 signaling, aiming to improve on GLP-1 monotherapy by increasing energy expenditure and directly targeting hepatic fat. This comparison highlights the trade-off between proven clinical validation and mechanistic advancement. For related dual agonist approaches, see our profiles on tirzepatide and mazdutide.
Quick Comparison#
| Feature | Semaglutide | Survodutide |
|---|---|---|
| Class | GLP-1 receptor agonist | GLP-1/glucagon dual agonist |
| Molecular Weight | 4.1 kDa | 4.2 kDa |
| Developer | Novo Nordisk | Boehringer Ingelheim / Zealand Pharma |
| FDA Status | 3 approvals (Ozempic, Wegovy, Rybelsus) | Phase 3 (no approvals) |
| Weight Loss | 14.9% (STEP 1) | Up to 19% (Phase 2) |
| Dosing | Weekly SC or daily oral | Weekly SC |
| MASH Program | No dedicated program | Phase 3 for MASH |
| CV Outcomes | SELECT trial (20% MACE reduction) | No outcomes data |
| Brand Names | Ozempic, Wegovy, Rybelsus | BI 456906 (development code) |
Mechanism of Action Comparison#
Semaglutide#
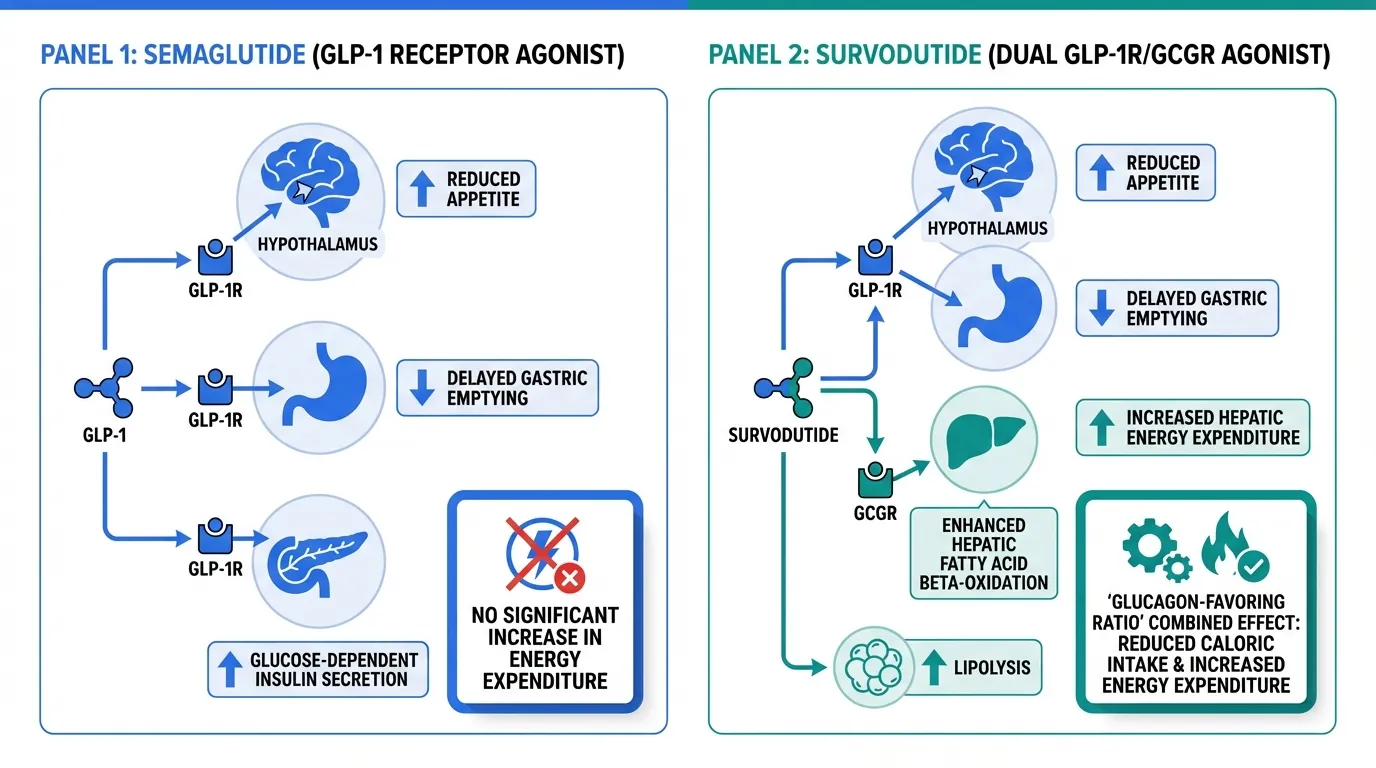
Semaglutide is a 31-amino acid GLP-1 receptor agonist with a C18 fatty diacid modification that enables albumin binding and a 7-day half-life. It selectively activates the GLP-1 receptor (GLP-1R), a class B GPCR, through Gs-cAMP-PKA signaling.
The therapeutic effects arise through three primary mechanisms: central appetite suppression via hypothalamic GLP-1R activation (reducing food intake by 20-35%), delayed gastric emptying through vagal pathways (enhancing satiety per meal), and glucose-dependent insulin secretion from pancreatic beta cells (improving glycemic control). These mechanisms work in concert to produce the consistent 15-17% body weight reduction observed across the STEP clinical program.
Notably, semaglutide does not substantially increase energy expenditure. The weight loss is driven almost entirely by reduced caloric intake through appetite suppression and slowed gastric transit.
Survodutide#
Survodutide (BI 456906) is a dual agonist that activates both the GLP-1 receptor and the glucagon receptor (GCGR), with an activity ratio favoring glucagon receptor activation approximately 4-5 fold over GLP-1R. This glucagon-favoring ratio is a deliberate pharmacological design choice that distinguishes survodutide from other dual agonists.
The GLP-1 component provides appetite suppression, delayed gastric emptying, and glucose-dependent insulin secretion, similar to semaglutide. The glucagon component adds three distinct mechanisms: increased hepatic energy expenditure and thermogenesis (increasing resting metabolic rate by an estimated 100-200 kcal/day), enhanced hepatic fatty acid beta-oxidation (directly reducing liver fat), and lipolysis in both hepatic and adipose tissue.
The critical pharmacological balance is that the GLP-1R activation offsets the hyperglycemic tendency of glucagon receptor agonism. The net metabolic effect combines reduced caloric intake (GLP-1) with increased energy expenditure (glucagon), creating a greater negative energy balance than either mechanism alone. This dual approach is particularly relevant for MASH, where hepatic steatosis is directly targeted by glucagon-mediated fat oxidation.
Evidence and Research Comparison#
Semaglutide Research#
Semaglutide has one of the most extensive clinical evidence bases of any peptide therapeutic:
- SUSTAIN trials: Seven Phase 3 studies in type 2 diabetes demonstrating HbA1c reduction and weight loss
- STEP trials: Four Phase 3 studies in obesity; STEP 1 showed 14.9% body weight reduction at 2.4 mg weekly
- SELECT trial: Cardiovascular outcomes study showing 20% MACE reduction in patients with obesity and established CVD without diabetes
- FLOW trial: Kidney outcomes data demonstrating renal protective effects
- Oral formulation: Rybelsus provides an oral dosing option at 7-14 mg daily
- Real-world data: Millions of prescriptions written, providing extensive post-marketing safety surveillance
Survodutide Research#
Survodutide's evidence base is growing but not yet mature:
- Phase 2 obesity trial: Demonstrated dose-dependent weight loss up to approximately 19% body weight reduction, exceeding typical GLP-1 monotherapy results
- Phase 2 MASH data: Histological improvement in liver biopsies, including reduction in hepatic steatosis and inflammation scores
- Phase 3 programs: Active Phase 3 trials for both obesity and MASH, with results anticipated to define the compound's clinical profile
- Mechanism validation: Clinical data support the dual mechanism concept, with evidence of both appetite reduction and increased energy expenditure
- Limitation: No regulatory approvals; no cardiovascular or renal outcomes data; limited long-term safety data
Side Effects and Safety Comparison#
Semaglutide Side Effects#
Well-characterized from large Phase 3 programs and millions of real-world prescriptions:
- GI effects: Nausea (44%), diarrhea (30%), vomiting (24%), constipation; typically dose-related and diminishing over time
- Serious risks: Pancreatitis (rare), gallbladder events, thyroid C-cell tumor boxed warning (from rodent studies)
- Dose escalation: Slow titration (0.25 mg escalating monthly) mitigates GI tolerability
- Strength: The safety database is massive, with well-defined risk-benefit profile across multiple patient populations
Survodutide Side Effects#
Less well-characterized with limited clinical exposure:
- GI effects: Expected GLP-1 class effects (nausea, vomiting, diarrhea) observed in Phase 2
- Glucagon-specific concerns: Potential for hepatic glucose output increase (mitigated by GLP-1 component), theoretical impact on blood glucose in diabetic populations
- Heart rate: Glucagon receptor agonism may affect heart rate; monitoring needed in Phase 3
- Unknown long-term risks: No outcomes data; rare adverse events not yet detectable from smaller trial populations
- Limitation: Phase 2 safety data insufficient for comprehensive risk-benefit assessment
Dosing and Administration Comparison#
Semaglutide Dosing#
| Parameter | Details |
|---|---|
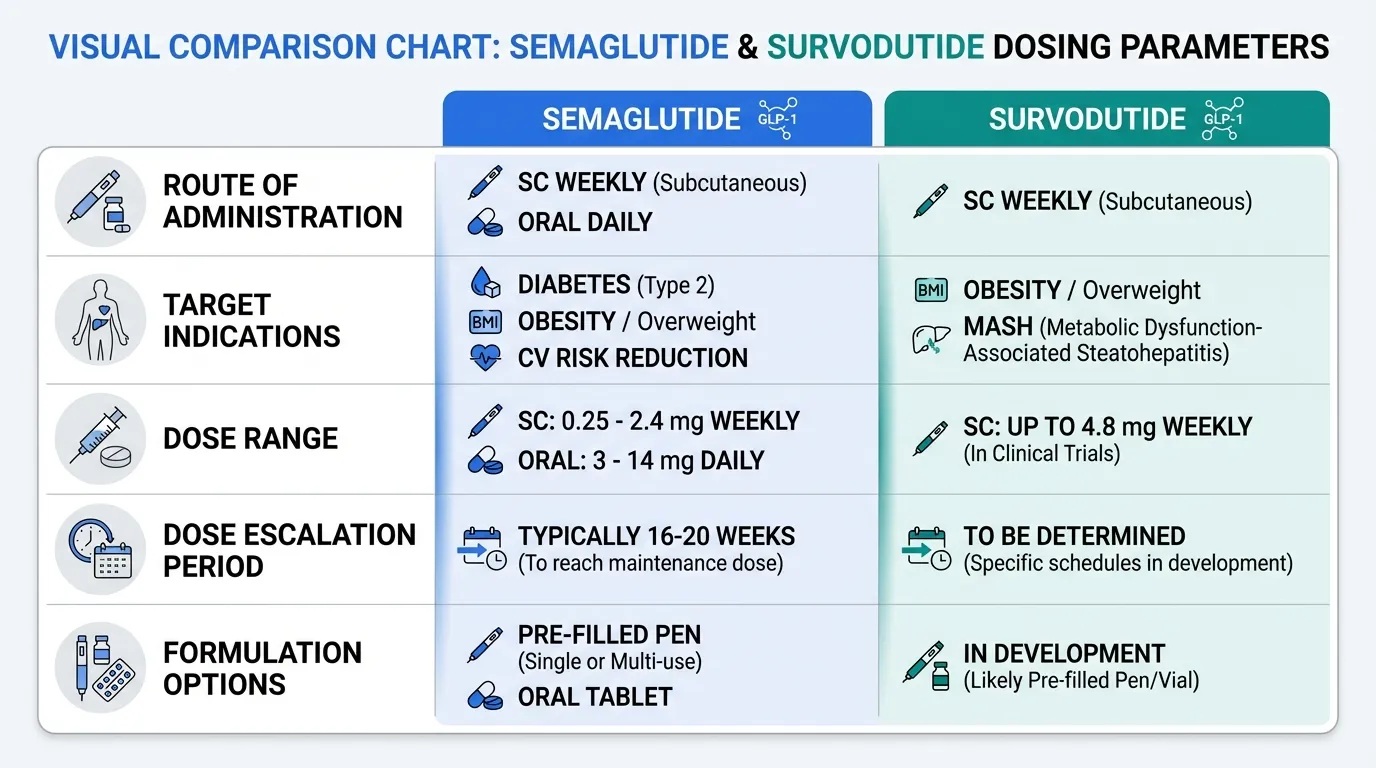
| Route | SC weekly (Ozempic/Wegovy) or oral daily (Rybelsus) |
| Diabetes (Ozempic) | 0.25 mg escalating to 1-2 mg weekly |
| Obesity (Wegovy) | 0.25 mg escalating to 2.4 mg weekly |
| Oral (Rybelsus) | 3 mg escalating to 7-14 mg daily |
| Escalation | Monthly dose increases over 16-20 weeks |
| Formulation options | Pre-filled pen (SC) or oral tablet |
Survodutide Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous weekly |
| Phase 2 doses | Escalating doses up to 4.8 mg weekly |
| Dose escalation | Gradual escalation to target dose |
| Oral option | None currently in development |
| Development stage | Dosing still being optimized in Phase 3 |
Use Case Recommendations#
Choose Semaglutide When:#
- Proven efficacy with FDA-approved dosing is required for current clinical use
- Cardiovascular risk reduction is a treatment goal (SELECT trial evidence)
- Oral dosing is preferred (Rybelsus option)
- Comprehensive safety data and well-characterized risk profile are priorities
- Type 2 diabetes is the primary indication alongside weight management
Choose Survodutide When:#
- MASH/NASH is a primary treatment target, where glucagon-mediated hepatic fat oxidation provides a differentiated mechanism
- Maximum weight loss beyond GLP-1 monotherapy is the goal, pending Phase 3 confirmation
- Energy expenditure enhancement is desired alongside appetite suppression
- Clinical trial participation is an option for accessing the compound before potential approval
Can They Be Combined?#
Combining semaglutide with survodutide is not pharmacologically rational, as survodutide already contains GLP-1R agonist activity. Adding a pure GLP-1 agonist would provide redundant GLP-1R stimulation without additional glucagon component, likely increasing GI side effects without proportional benefit.
The relevant clinical question is whether survodutide's dual mechanism will prove superior to semaglutide monotherapy in head-to-head comparison. No direct comparative trials have been published. Cross-trial comparisons suggest survodutide may achieve greater absolute weight loss, but differences in trial design, patient populations, and endpoints make direct comparison unreliable.
For other metabolic peptide comparisons, see mazdutide vs semaglutide and mazdutide vs tirzepatide. Explore our GLP-1 saturation calculator for semaglutide pharmacokinetic modeling.
Verdict#
Semaglutide is the proven standard with unmatched clinical validation across diabetes, obesity, and cardiovascular outcomes. Survodutide represents a mechanistic evolution that addresses a key limitation of GLP-1 monotherapy by adding glucagon-mediated energy expenditure and direct hepatic fat reduction.
For current clinical use, semaglutide has no peer in terms of evidence quality, regulatory status, and real-world experience. For the future of metabolic therapeutics, survodutide's Phase 2 data are encouraging, particularly for MASH where the glucagon mechanism provides a uniquely differentiated approach. The critical question is whether Phase 3 trials will confirm the Phase 2 efficacy signal and establish an acceptable safety profile for this glucagon-favoring dual agonist. Until then, semaglutide remains the evidence-based benchmark against which survodutide and all other metabolic peptides are measured.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Current obesity treatment with proven efficacy
Semaglutide
FDA-approved as Wegovy with 14.9% weight loss in STEP trials; extensive safety database and real-world prescribing experience
MASH/NASH treatment research
Survodutide
Glucagon receptor activation directly targets hepatic steatosis; specific MASH Phase 3 program with histological endpoints
Cardiovascular risk reduction in obesity
Semaglutide
SELECT trial demonstrated 20% MACE reduction; only GLP-1 agonist with dedicated cardiovascular outcomes data in obesity population
Maximizing weight loss beyond GLP-1 monotherapy
Survodutide
Phase 2 data suggest up to 19% weight loss; dual mechanism targeting both appetite (GLP-1) and energy expenditure (glucagon) for greater net negative energy balance
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Semaglutide vs Survodutide: GLP-1 vs Dual Agonist Compared
Which is better, Semaglutide or Survodutide?
Semaglutide is the established standard with three FDA approvals, massive clinical evidence, and proven cardiovascular outcomes. Survodutide represents the next-generation approach, adding glucagon receptor agonism to GLP-1 signaling for potentially greater weight loss and a unique MASH indication. However, survodutide remains in Phase 3 without regulatory approval. For current clinical use, semaglutide has unmatched validation. For the future of metabolic therapeutics, survodutide's dual mec... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Semaglutide and Survodutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Survodutide; Research Evidence: advantage goes to Semaglutide; Side Effect Profile: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Survodutide?
For the scenario of "Current obesity treatment with proven efficacy," research data suggests Semaglutide may be more relevant. FDA-approved as Wegovy with 14.9% weight loss in STEP trials; extensive safety database and real-world prescribing experience. This is based on currently available evidence and individual circumstances may differ.
How do Semaglutide and Survodutide differ in their mechanisms of action?
Semaglutide: Selective GLP-1 receptor agonist; C18 fatty diacid enables albumin binding for weekly dosing; activates Gs-cAMP-PKA in beta cells and hypothalamic appetite centers; delayed gastric emptying via vag.... Survodutide: Dual GLP-1R/GCGR agonist with glucagon-favoring activity ratio (~4-5x GCGR vs GLP-1R); combines appetite suppression (GLP-1) with increased energy expenditure and hepatic fat oxidation (glucagon); ....
Which has fewer side effects, Semaglutide or Survodutide?
In terms of side effects and tolerability, the advantage goes to Semaglutide. Semaglutide: Well-characterized GI side effects (nausea 44%, diarrhea 30%, vomiting 24%); pancreatitis risk; gallbladder events; thyroid C-cell tumor warning; e.... Survodutide: GI side effects similar to GLP-1 class; glucagon component may increase hepatic glucose output (mitigated by GLP-1); limited safety database from P....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.