Mazdutide vs Semaglutide: GLP-1 Agonists Compared
Comparing mazdutide and semaglutide for weight loss and diabetes, covering dual vs single agonist mechanisms, clinical trial data, and side effect profiles.
Verdict at a Glance
Semaglutide for proven efficacy with extensive safety data and global availability; mazdutide shows promise for potentially greater weight loss through dual agonism but requires broader clinical validation
| Best for | Pick | Why |
|---|---|---|
| Proven Weight Management | Semaglutide | Semaglutide has the largest clinical evidence base among GLP-1 agonists, with multiple Phase III trials, cardiovascular outcome data, and years of real-world post-marketing experience |
| Type 2 Diabetes with Cardiovascular Risk | Semaglutide | The SELECT trial demonstrated a 20% reduction in MACE events, making semaglutide the only GLP-1 RA with proven cardiovascular benefit in non-diabetic obese patients |
| Maximum Weight Loss Potential | Mazdutide | Phase III data showing up to 20.1% body weight reduction suggests the dual GLP-1/glucagon mechanism may achieve greater weight loss than single GLP-1 agonism, though head-to-head data is lacking |
| Metabolic Syndrome with Hepatic Steatosis | Mazdutide | Glucagon receptor agonism may provide additional hepatic benefits through increased fatty acid oxidation and energy expenditure, though clinical evidence for this indication is still emerging |
| Oral Administration Option | Semaglutide | Rybelsus provides the only oral GLP-1 RA option; mazdutide is currently injectable-only with no oral formulation in development |
| Category | Mazdutide | Semaglutide | Advantage |
|---|---|---|---|
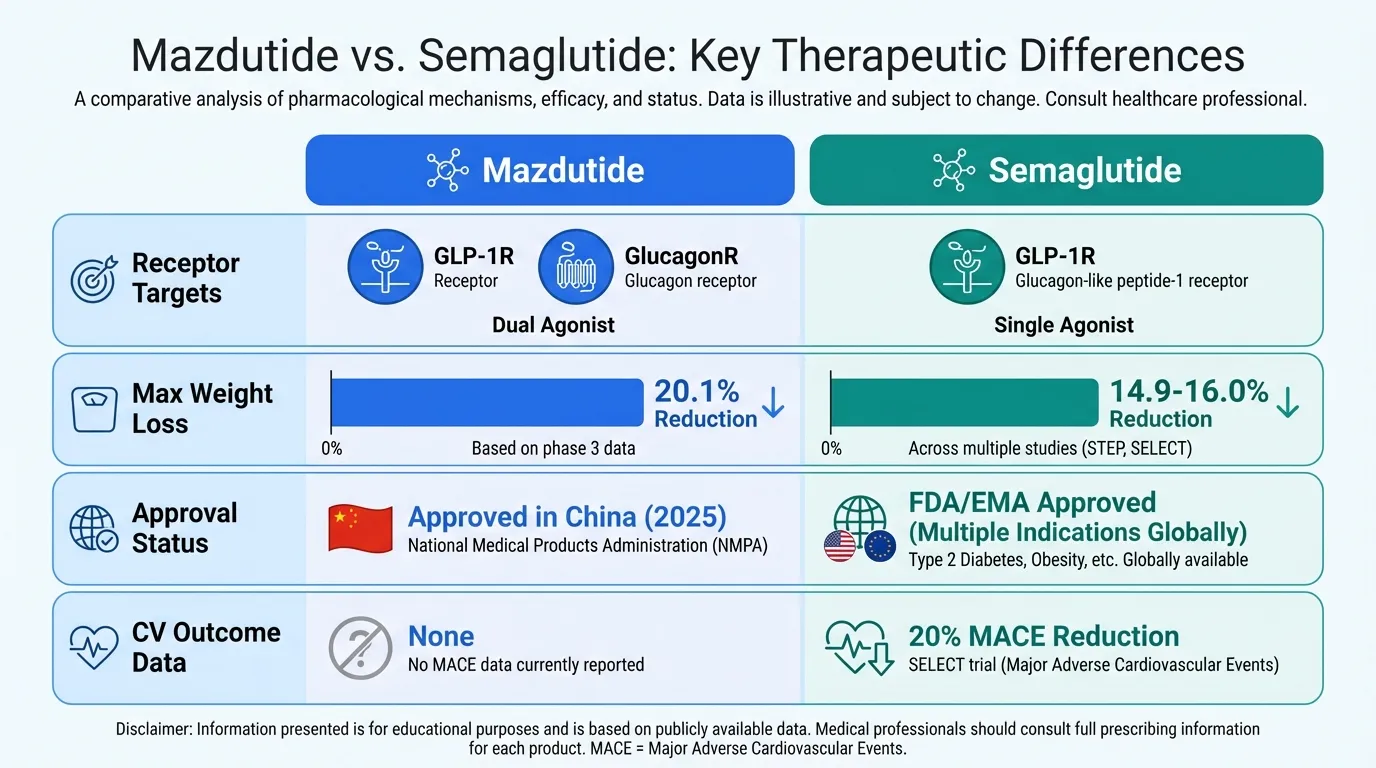
| Mechanism of Action | Dual GLP-1 and glucagon receptor agonist; oxyntomodulin analog providing synergistic metabolic effects through two receptor pathways | Selective GLP-1 receptor agonist; single-target incretin mimetic with well-characterized appetite and glycemic control mechanism | Mazdutide |
| Research Evidence | Phase III trials in China showing up to 20.1% weight loss; approved in China (2025); limited global clinical data | Extensive Phase III program (STEP, SUSTAIN, SELECT); FDA/EMA-approved; cardiovascular outcome data; thousands of patients studied | Semaglutide |
| Side Effect Profile | GI side effects (nausea, diarrhea, vomiting) common; limited long-term safety data; glucagon component may add hepatic considerations | Well-characterized GI side effects; extensive post-marketing safety data; proven cardiovascular safety in SELECT trial | Semaglutide |
| Weight Loss Efficacy | Up to 20.1% body weight reduction at 60 weeks (9 mg dose) in Phase III trials; potentially greater efficacy from dual mechanism | 14.9% weight reduction in STEP 1 (2.4 mg); 16.0% in STEP 5; consistent efficacy across multiple large-scale RCTs | Mazdutide |
| Regulatory Status | Approved in China (June 2025) for weight management; not yet approved in US/EU; global Phase III trials ongoing | FDA-approved as Ozempic (T2D), Wegovy (obesity), Rybelsus (oral); EMA and global approvals; established formulary presence | Semaglutide |

Introduction#
The landscape of incretin-based therapies for obesity and type 2 diabetes is expanding rapidly beyond single-target GLP-1 receptor agonists. Mazdutide (IBI362/LY3305677) represents the dual GLP-1/glucagon receptor agonist approach, while semaglutide (Ozempic/Wegovy) remains the benchmark single-target GLP-1 RA against which all newer agents are measured.
This comparison examines how mazdutide's dual agonist mechanism compares to semaglutide's established single-target approach across efficacy, safety, evidence quality, and clinical availability. Both are once-weekly subcutaneous peptides with C18-C20 fatty acid modifications for albumin binding and extended half-life, but they diverge fundamentally in their receptor pharmacology and the breadth of their clinical evidence.
Quick Comparison Table#
| Feature | Mazdutide | Semaglutide |
|---|---|---|
| Receptor targets | GLP-1R + Glucagon receptor | GLP-1R only |
| Structure | 33 amino acids, C20 fatty diacid (4563 Da) | 31 amino acids, C18 fatty diacid (4114 Da) |
| Max weight loss | Up to 20.1% (60 weeks, 9 mg) | 14.9-16.0% (STEP trials, 2.4 mg) |
| Approval status | Approved in China (2025) | FDA/EMA approved (multiple indications) |
| CV outcome data | None | SELECT trial: 20% MACE reduction |
| Dosing | Once weekly SC (3-9 mg) | Once weekly SC (0.25-2.4 mg) or oral |
| Developer | Innovent Biologics / Eli Lilly | Novo Nordisk |
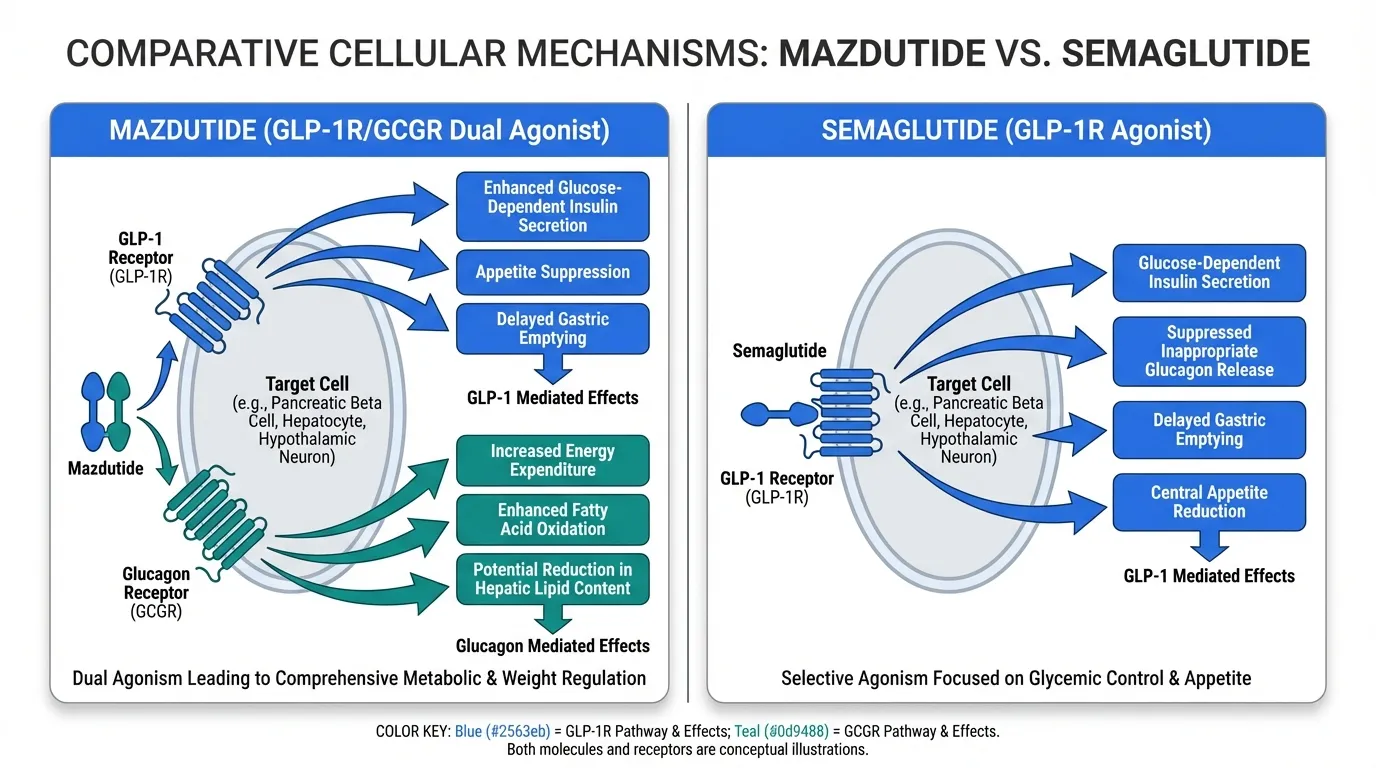
Mechanism of Action Comparison#
Mazdutide#
Mazdutide is a synthetic oxyntomodulin analog that simultaneously activates both the GLP-1 receptor and the glucagon receptor. The GLP-1 component provides the established incretin effects: enhanced glucose-dependent insulin secretion, suppressed glucagon release (paradoxically, the GLP-1-mediated pancreatic glucagon suppression coexists with hepatic glucagon receptor activation), delayed gastric emptying, and central appetite suppression through hypothalamic signaling.
The glucagon receptor agonism adds metabolic effects not achievable with GLP-1 alone: increased hepatic glucose output (counterbalanced by GLP-1-mediated insulin secretion), enhanced fatty acid oxidation, increased energy expenditure, and potential reduction in hepatic lipid content. This dual mechanism aims to achieve greater weight loss through complementary pathways -- GLP-1 reducing caloric intake while glucagon increases energy expenditure.
Semaglutide#
Semaglutide is a selective GLP-1 receptor agonist that mimics the endogenous incretin hormone GLP-1. It binds exclusively to the GLP-1R, a class B GPCR expressed on pancreatic beta cells, hypothalamic neurons, and gastrointestinal tract cells.
The mechanism produces glucose-dependent insulin secretion, suppressed inappropriate glucagon release, delayed gastric emptying, and powerful central appetite reduction through hypothalamic and brainstem satiety circuits. Semaglutide's C18 fatty diacid chain at Lys26 enables strong albumin binding, resulting in a half-life of approximately 7 days and supporting once-weekly dosing.
Evidence and Research Comparison#
Mazdutide Clinical Evidence#
Mazdutide's evidence base, while growing, is primarily from Chinese clinical trials:
- Phase III obesity trial: At the 9 mg dose, participants achieved up to 20.1% body weight reduction at 60 weeks, with dose-dependent effects across the 3 mg, 6 mg, and 9 mg arms
- Phase III diabetes trial: Significant HbA1c reductions of up to -2.15% versus placebo in patients with type 2 diabetes, alongside meaningful weight loss
- China approval: Approved in June 2025 for chronic weight management in Chinese adults with obesity
- Global trials: International Phase III programs are ongoing but results have not yet been reported
Semaglutide Clinical Evidence#
Semaglutide has one of the most comprehensive clinical evidence programs in metabolic medicine:
- STEP program: Multiple Phase III trials across diverse populations. STEP 1 (n=1,961) demonstrated 14.9% mean weight loss at 68 weeks. STEP 5 showed 16.0% at 104 weeks, demonstrating sustained efficacy
- SUSTAIN program: Established glycemic control superiority over comparators in type 2 diabetes across multiple trials
- SELECT trial: Landmark cardiovascular outcome trial (n=17,604) showing 20% reduction in major adverse cardiovascular events in overweight/obese adults without diabetes
- Real-world data: Years of post-marketing surveillance across millions of prescriptions globally
- Oral formulation: Rybelsus demonstrated oral bioavailability, expanding administration options
Evidence Quality Assessment#
The gap in evidence quality is substantial. Semaglutide benefits from over a decade of clinical development, large multi-ethnic trial populations, cardiovascular outcome data, and extensive post-marketing surveillance. Mazdutide's data, while promising, is limited to Chinese populations and lacks cardiovascular outcome data, long-term safety follow-up, and head-to-head comparisons with established GLP-1 RAs.
Side Effects and Safety Comparison#
Mazdutide Side Effects#
Clinical trial data shows a side effect profile consistent with incretin-based therapies, though the glucagon component introduces considerations:
- Gastrointestinal: Nausea, diarrhea, and vomiting are the most common adverse events, similar to other GLP-1 RAs
- Hepatic considerations: Glucagon receptor activation affects hepatic metabolism; long-term hepatic safety monitoring is ongoing
- Dose-dependent tolerability: Higher doses (9 mg) show greater GI side effects but also greater efficacy
- Limited long-term data: Post-marketing surveillance is limited to the Chinese market since 2025
Semaglutide Side Effects#
Semaglutide's safety profile is the most extensively characterized among GLP-1 RAs:
- Gastrointestinal: Nausea (approximately 44% in STEP 1), diarrhea, vomiting, and constipation; typically transient during dose escalation
- Cardiovascular: Proven safety and benefit (SELECT trial); transient heart rate increases of 1-4 bpm
- Pancreatitis: Rare cases reported; monitoring recommended
- Gallbladder events: Increased cholelithiasis risk observed across GLP-1 RA class
- Thyroid: Boxed warning for medullary thyroid carcinoma based on rodent data; not observed in human studies
Dosing and Administration Comparison#
Mazdutide Dosing#
- Once-weekly subcutaneous injection
- Dose escalation from 3 mg to 6 mg to 9 mg
- Administered in the abdomen, thigh, or upper arm
- No oral formulation available
Semaglutide Dosing#
- Injectable (Ozempic/Wegovy): Once-weekly SC; dose escalation from 0.25 mg to target dose of 1.0 mg (diabetes) or 2.4 mg (obesity)
- Oral (Rybelsus): Daily oral tablet; 3 mg, 7 mg, or 14 mg doses taken on an empty stomach with minimal water
- Auto-injector pens available for self-administration
Use Case Recommendations#
When Semaglutide Is Preferred#
- First-line obesity treatment: Extensive evidence supports efficacy and safety
- Cardiovascular risk reduction: Only GLP-1 RA with proven MACE reduction in non-diabetic obese patients
- Patients requiring oral option: Rybelsus provides non-injectable alternative
- Clinical settings requiring proven safety data: Post-marketing experience across millions of patients
When Mazdutide May Be Considered#
- Research into dual agonist mechanisms: The GLP-1/glucagon approach represents a distinct pharmacological strategy
- Patients in approved markets: Currently limited to China
- Potential for greater weight loss: If head-to-head data confirms the efficacy signal from Phase III trials
Can They Be Combined?#
Combining mazdutide with semaglutide would not be appropriate as both activate the GLP-1 receptor, creating overlapping pharmacology with additive GI side effects and no clear benefit over either agent alone. The comparison is best understood as an either/or choice between single and dual agonist approaches.
For researchers interested in the dual agonist landscape, survodutide (GLP-1/glucagon) and tirzepatide (GLP-1/GIP) represent alternative dual-target strategies worth examining.
Verdict#
Semaglutide remains the gold standard among incretin-based therapies, backed by an unmatched clinical evidence program that includes cardiovascular outcome data, long-term safety surveillance, multiple formulations, and global regulatory approvals. It is the appropriate first choice for most clinical and research applications in metabolic disease.
Mazdutide represents a promising next-generation approach, and its Phase III weight loss data (up to 20.1%) suggests that dual GLP-1/glucagon agonism may achieve meaningfully greater weight reduction than GLP-1 alone. However, the absence of cardiovascular outcome data, limited ethnic diversity in clinical trials, and restricted availability currently limit its positioning.
The field would benefit from head-to-head trials comparing these agents directly, as the cross-trial comparison of 20.1% versus 14.9-16.0% weight loss, while suggestive, cannot account for differences in trial design, patient populations, and dose optimization.
Explore full profiles of Mazdutide and Semaglutide, or see how they compare to Tirzepatide and Survodutide. Use our GLP-1 Saturation Calculator for steady-state pharmacokinetic modeling.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Proven Weight Management
Semaglutide
Semaglutide has the largest clinical evidence base among GLP-1 agonists, with multiple Phase III trials, cardiovascular outcome data, and years of real-world post-marketing experience
Type 2 Diabetes with Cardiovascular Risk
Semaglutide
The SELECT trial demonstrated a 20% reduction in MACE events, making semaglutide the only GLP-1 RA with proven cardiovascular benefit in non-diabetic obese patients
Maximum Weight Loss Potential
Mazdutide
Phase III data showing up to 20.1% body weight reduction suggests the dual GLP-1/glucagon mechanism may achieve greater weight loss than single GLP-1 agonism, though head-to-head data is lacking
Metabolic Syndrome with Hepatic Steatosis
Mazdutide
Glucagon receptor agonism may provide additional hepatic benefits through increased fatty acid oxidation and energy expenditure, though clinical evidence for this indication is still emerging
Oral Administration Option
Semaglutide
Rybelsus provides the only oral GLP-1 RA option; mazdutide is currently injectable-only with no oral formulation in development
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Mazdutide vs Semaglutide: GLP-1 Agonists Compared
What are the key differences between Mazdutide and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Mazdutide; Research Evidence: advantage goes to Semaglutide; Side Effect Profile: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Mazdutide?
For the scenario of "Proven Weight Management," research data suggests Semaglutide may be more relevant. Semaglutide has the largest clinical evidence base among GLP-1 agonists, with multiple Phase III trials, cardiovascular outcome data, and years of real-world post-marketing experience. This is based on currently available evidence and individual circumstances may differ.
How do Mazdutide and Semaglutide differ in their mechanisms of action?
Mazdutide: Dual GLP-1 and glucagon receptor agonist; oxyntomodulin analog providing synergistic metabolic effects through two receptor pathways. Semaglutide: Selective GLP-1 receptor agonist; single-target incretin mimetic with well-characterized appetite and glycemic control mechanism.
Which has fewer side effects, Mazdutide or Semaglutide?
In terms of side effects and tolerability, the advantage goes to Semaglutide. Mazdutide: GI side effects (nausea, diarrhea, vomiting) common; limited long-term safety data; glucagon component may add hepatic considerations. Semaglutide: Well-characterized GI side effects; extensive post-marketing safety data; proven cardiovascular safety in SELECT trial.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.