Amycretin vs Semaglutide: Next-Gen Dual GLP-1/Amylin vs Proven GLP-1
Evidence-based comparison of amycretin (unimolecular GLP-1/amylin agonist) and semaglutide, including Phase 1b/2a weight loss data and development status.
Verdict at a Glance
Amycretin shows potentially superior weight loss (up to 24.3% in Phase 1b/2a) compared to semaglutide (14.9% in STEP 1), driven by its dual GLP-1/amylin mechanism in a single molecule. The ability to offer both injectable and oral formulations without fasting restrictions is a significant advantage. However, these are early-phase results with small sample sizes and short duration. Semaglutide remains the proven, FDA-approved standard with cardiovascular benefit and extensive safety data. Amycretin is Novo Nordisk's most promising pipeline asset, but Phase 3 confirmation is needed before definitive comparisons can be made.
| Best for | Pick | Why |
|---|---|---|
| Proven Treatment Today | Semaglutide | Semaglutide is FDA-approved, widely available, and backed by 25,000+ trial participants and 7+ years of post-marketing data. Amycretin is years from potential approval. |
| Cardiovascular Risk Reduction | Semaglutide | SELECT demonstrated 20% MACE reduction. Amycretin has no cardiovascular outcomes data and will not have any for years. |
| Maximum Weight Loss Potential (Future) | Amycretin | Phase 1b/2a showed up to 24.3% weight loss at 36 weeks with no plateau, suggesting even greater loss with longer treatment. If confirmed in Phase 3, this would substantially exceed semaglutide. |
| Convenient Oral Dosing (Future) | Amycretin | Oral amycretin is being developed without the fasting restrictions required by oral semaglutide (Rybelsus). If approved, it would combine superior efficacy with simpler oral administration. |
| Category | Amycretin | Semaglutide | Advantage |
|---|---|---|---|
| Mechanism of Action | Unimolecular dual GLP-1 and amylin receptor agonist. A single molecule that activates both pathways simultaneously. Available as both subcutaneous (weekly) and oral (daily) formulations. | Selective GLP-1 receptor agonist. Activates GLP-1 receptors only. Available as injectable (Ozempic/Wegovy, weekly) and oral (Rybelsus, daily with fasting restrictions). | Amycretin |
| Weight Loss Efficacy | Phase 1b/2a showed up to 24.3% weight loss at highest SC dose (60 mg) at 36 weeks, with no plateau observed. Phase 2 in T2D showed up to 14.5% at 36 weeks. Published in The Lancet. | STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. STEP 3 showed 16.0% with intensive lifestyle. Proven, reproducible efficacy across multiple large Phase 3 trials. | Amycretin |
| Development Stage | Phase 1b/2a completed (obesity, Lancet). Phase 2 completed (T2D). Phase 3 planned for obesity (2025) and T2D (2026). Not approved. Limited safety data from early-phase trials. | FDA-approved since 2017 for T2D, 2021 for obesity. Over 25,000 clinical trial participants across SUSTAIN, PIONEER, STEP, SELECT programs. 7+ years of post-marketing surveillance. | Semaglutide |
| Dosing Convenience | Available as once-weekly subcutaneous injection AND once-daily oral tablet. Both formulations being developed in parallel. Oral amycretin does not require the SNAC enhancer used by oral semaglutide. | Injectable (Ozempic/Wegovy) is once-weekly SC. Oral (Rybelsus) requires fasting, max 4 oz water, 30-min wait. The SNAC-based formulation has strict dosing requirements. | Amycretin |
| Safety Profile | GI adverse events most common, consistent with GLP-1/amylin class. High frequency of GI events reported in early trials but mostly mild-moderate. Limited long-term safety data. | Well-characterized over 7+ years. Proven CV safety (SELECT, 20% MACE reduction). Known GI side effect profile. Extensive post-marketing surveillance with rare events identified. | Semaglutide |

Introduction#
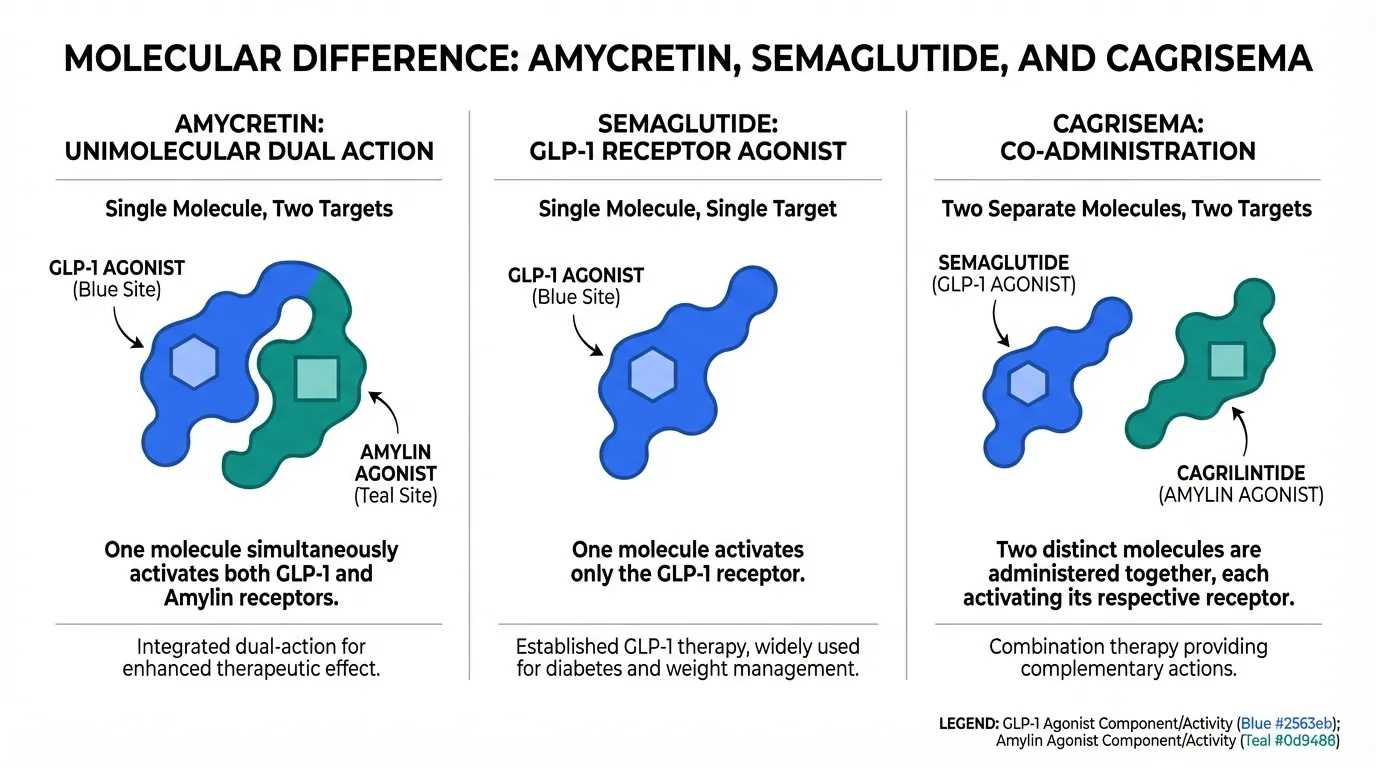
Amycretin and semaglutide are both developed by Novo Nordisk, representing the company's current and future generations of obesity treatment. Semaglutide is the proven GLP-1 agonist powering Ozempic, Wegovy, and Rybelsus. Amycretin is a next-generation unimolecular dual GLP-1/amylin receptor agonist that showed up to 24.3% weight loss in early trials, substantially exceeding semaglutide and potentially exceeding even CagriSema.
The key difference from CagriSema (which combines separate cagrilintide and semaglutide) is that amycretin integrates both GLP-1 and amylin agonism into a single molecule, enabling both subcutaneous and oral formulations.
Mechanism of Action Comparison#
Amycretin#
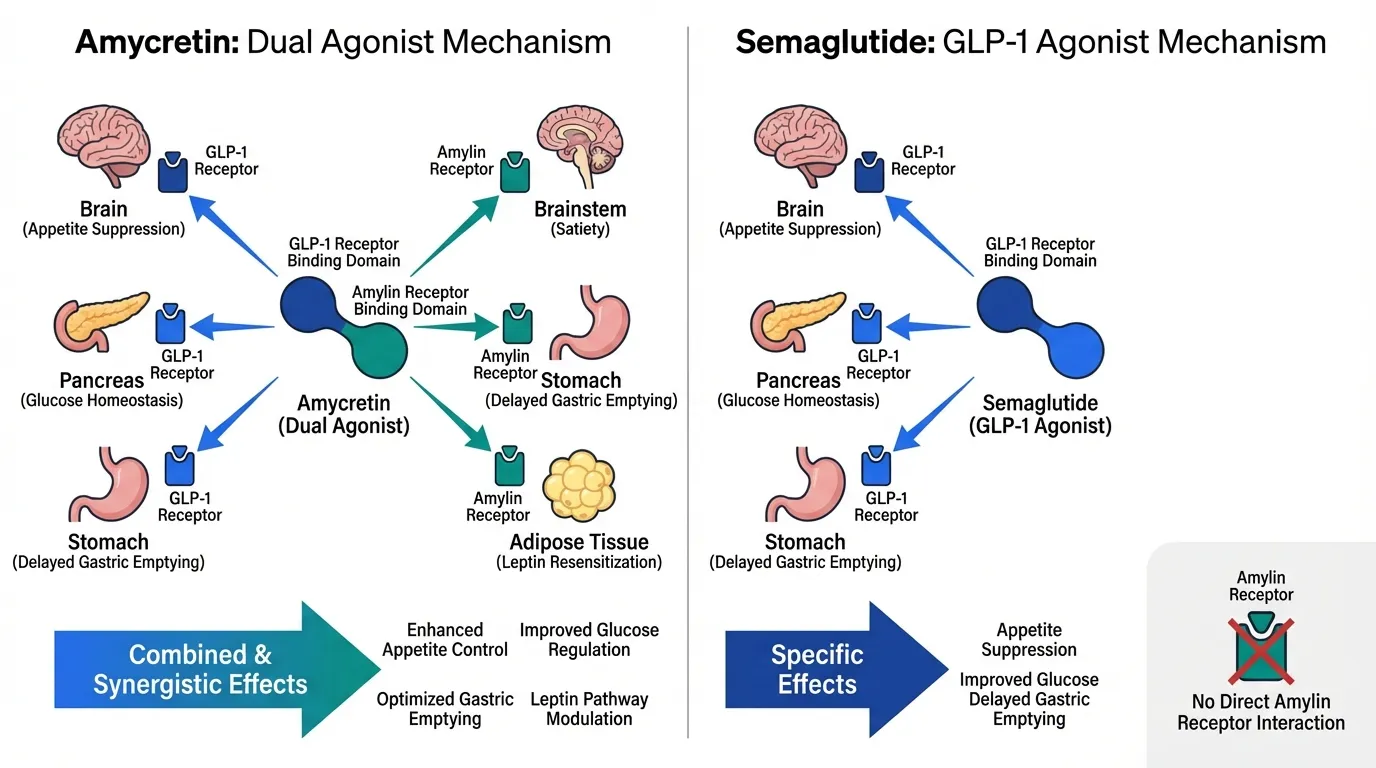
Amycretin is a unimolecular agonist that simultaneously activates both GLP-1 and amylin receptors through a single peptide. The GLP-1 component provides appetite suppression and glucose homeostasis. The amylin component adds brainstem-mediated satiety, gastric emptying delay, and leptin resensitization. Unlike CagriSema, both activities are built into one molecule.
Semaglutide#
Semaglutide is a selective GLP-1 receptor agonist with no amylin activity. It provides appetite suppression, delayed gastric emptying, and glucose homeostasis through a single receptor pathway.
Clinical Evidence#
Amycretin Phase 1b/2a (Obesity, Lancet)#
125 adults with overweight or obesity. Once-weekly subcutaneous amycretin up to 60 mg for 36 weeks.
| Outcome | Amycretin (highest dose) | Placebo |
|---|---|---|
| Weight loss | Up to 24.3% | 1.1% |
| Weight plateau | Not reached at 36 weeks | N/A |
| Tolerability | Consistent with GLP-1/amylin class | N/A |
Amycretin Phase 2 (Type 2 Diabetes)#
448 adults with T2D inadequately controlled on metformin. SC and oral formulations evaluated.
| Outcome | SC Amycretin (highest dose) | Placebo |
|---|---|---|
| Weight loss | Up to 14.5% | 2.6% |
| Weight plateau | Not reached at 36 weeks | N/A |
Semaglutide STEP 1#
1,961 adults with obesity or overweight. Semaglutide 2.4 mg weekly for 68 weeks.
| Outcome | Semaglutide 2.4 mg | Placebo |
|---|---|---|
| Weight loss | 14.9% | 2.4% |
| Achieved 15%+ | 50.5% | 4.9% |
Key Differences Summary#
- Weight loss: Amycretin up to 24.3% (Phase 1b/2a, 36 wk) vs semaglutide 14.9% (Phase 3, 68 wk)
- Mechanism: Amycretin is dual GLP-1/amylin; semaglutide is GLP-1-only
- Molecule: Amycretin is unimolecular (single peptide); CagriSema requires two
- Formulations: Both have SC and oral; amycretin oral may not need fasting restrictions
- Approval: Semaglutide is FDA-approved; amycretin is entering Phase 3
- Evidence: Semaglutide has 25,000+ trial participants; amycretin has <600
- CV outcomes: Semaglutide has SELECT (20% MACE reduction); amycretin has no CV data
Conclusion#
Amycretin represents the most exciting pipeline asset in obesity medicine, with 24.3% weight loss in early trials suggesting it could substantially exceed every approved treatment. However, Phase 1b/2a results in 125 patients must be confirmed in large Phase 3 trials. Semaglutide remains the proven standard of care with an unmatched evidence base and cardiovascular benefit. Amycretin's earliest potential approval is several years away, making semaglutide the only option for patients who need treatment today.
Detailed Category Analysis#
Mechanism of Action#
Amycretin: Unimolecular dual GLP-1 and amylin receptor agonist. A single molecule that activates both pathways simultaneously. Available as both subcutaneous (weekly) and oral (daily) formulations.
Semaglutide: Selective GLP-1 receptor agonist. Activates GLP-1 receptors only. Available as injectable (Ozempic/Wegovy, weekly) and oral (Rybelsus, daily with fasting restrictions).
Advantage: Amycretin
Weight Loss Efficacy#
Amycretin: Phase 1b/2a showed up to 24.3% weight loss at highest SC dose (60 mg) at 36 weeks, with no plateau observed. Phase 2 in T2D showed up to 14.5% at 36 weeks. Published in The Lancet.
Semaglutide: STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. STEP 3 showed 16.0% with intensive lifestyle. Proven, reproducible efficacy across multiple large Phase 3 trials.
Advantage: Amycretin
Development Stage#
Amycretin: Phase 1b/2a completed (obesity, Lancet). Phase 2 completed (T2D). Phase 3 planned for obesity (2025) and T2D (2026). Not approved. Limited safety data from early-phase trials.
Semaglutide: FDA-approved since 2017 for T2D, 2021 for obesity. Over 25,000 clinical trial participants across SUSTAIN, PIONEER, STEP, SELECT programs. 7+ years of post-marketing surveillance.
Advantage: Semaglutide
Dosing Convenience#
Amycretin: Available as once-weekly subcutaneous injection AND once-daily oral tablet. Both formulations being developed in parallel. Oral amycretin does not require the SNAC enhancer used by oral semaglutide.
Semaglutide: Injectable (Ozempic/Wegovy) is once-weekly SC. Oral (Rybelsus) requires fasting, max 4 oz water, 30-min wait. The SNAC-based formulation has strict dosing requirements.
Advantage: Amycretin
Safety Profile#
Amycretin: GI adverse events most common, consistent with GLP-1/amylin class. High frequency of GI events reported in early trials but mostly mild-moderate. Limited long-term safety data.
Semaglutide: Well-characterized over 7+ years. Proven CV safety (SELECT, 20% MACE reduction). Known GI side effect profile. Extensive post-marketing surveillance with rare events identified.
Advantage: Semaglutide
Summary and Verdict#
Amycretin shows potentially superior weight loss (up to 24.3% in Phase 1b/2a) compared to semaglutide (14.9% in STEP 1), driven by its dual GLP-1/amylin mechanism in a single molecule. The ability to offer both injectable and oral formulations without fasting restrictions is a significant advantage. However, these are early-phase results with small sample sizes and short duration. Semaglutide remains the proven, FDA-approved standard with cardiovascular benefit and extensive safety data. Amycretin is Novo Nordisk's most promising pipeline asset, but Phase 3 confirmation is needed before definitive comparisons can be made.
Best For Recommendations#
Proven Treatment Today#
Recommendation: Semaglutide
Reason: Semaglutide is FDA-approved, widely available, and backed by 25,000+ trial participants and 7+ years of post-marketing data. Amycretin is years from potential approval.
Cardiovascular Risk Reduction#
Recommendation: Semaglutide
Reason: SELECT demonstrated 20% MACE reduction. Amycretin has no cardiovascular outcomes data and will not have any for years.
Maximum Weight Loss Potential (Future)#
Recommendation: Amycretin
Reason: Phase 1b/2a showed up to 24.3% weight loss at 36 weeks with no plateau, suggesting even greater loss with longer treatment. If confirmed in Phase 3, this would substantially exceed semaglutide.
Convenient Oral Dosing (Future)#
Recommendation: Amycretin
Reason: Oral amycretin is being developed without the fasting restrictions required by oral semaglutide (Rybelsus). If approved, it would combine superior efficacy with simpler oral administration.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Proven Treatment Today
Semaglutide
Semaglutide is FDA-approved, widely available, and backed by 25,000+ trial participants and 7+ years of post-marketing data. Amycretin is years from potential approval.
Cardiovascular Risk Reduction
Semaglutide
SELECT demonstrated 20% MACE reduction. Amycretin has no cardiovascular outcomes data and will not have any for years.
Maximum Weight Loss Potential (Future)
Amycretin
Phase 1b/2a showed up to 24.3% weight loss at 36 weeks with no plateau, suggesting even greater loss with longer treatment. If confirmed in Phase 3, this would substantially exceed semaglutide.
Convenient Oral Dosing (Future)
Amycretin
Oral amycretin is being developed without the fasting restrictions required by oral semaglutide (Rybelsus). If approved, it would combine superior efficacy with simpler oral administration.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Amycretin vs Semaglutide: Next-Gen Dual GLP-1/Amylin vs Proven GLP-1
Which is better, Amycretin or Semaglutide?
Amycretin shows potentially superior weight loss (up to 24.3% in Phase 1b/2a) compared to semaglutide (14.9% in STEP 1), driven by its dual GLP-1/amylin mechanism in a single molecule. The ability to offer both injectable and oral formulations without fasting restrictions is a significant advantage. However, these are early-phase results with small sample sizes and short duration. Semaglutide remains the proven, FDA-approved standard with cardiovascular benefit and extensive safety data. Amyc... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Amycretin and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Amycretin; Weight Loss Efficacy: advantage goes to Amycretin; Development Stage: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Amycretin?
For the scenario of "Proven Treatment Today," research data suggests Semaglutide may be more relevant. Semaglutide is FDA-approved, widely available, and backed by 25,000+ trial participants and 7+ years of post-marketing data. Amycretin is years from potential approval.. This is based on currently available evidence and individual circumstances may differ.
How do Amycretin and Semaglutide differ in their mechanisms of action?
Amycretin: Unimolecular dual GLP-1 and amylin receptor agonist. A single molecule that activates both pathways simultaneously. Available as both subcutaneous (weekly) and oral (daily) formulations.. Semaglutide: Selective GLP-1 receptor agonist. Activates GLP-1 receptors only. Available as injectable (Ozempic/Wegovy, weekly) and oral (Rybelsus, daily with fasting restrictions)..
Which has fewer side effects, Amycretin or Semaglutide?
In terms of side effects and tolerability, the advantage goes to Semaglutide. Amycretin: GI adverse events most common, consistent with GLP-1/amylin class. High frequency of GI events reported in early trials but mostly mild-moderate. L.... Semaglutide: Well-characterized over 7+ years. Proven CV safety (SELECT, 20% MACE reduction). Known GI side effect profile. Extensive post-marketing surveillanc....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.