Ecnoglutide vs Semaglutide: Biased GLP-1 Agonist vs Proven Standard of Care
Evidence-based comparison of ecnoglutide (cAMP-biased GLP-1 agonist) and semaglutide (selective GLP-1 agonist), including SLIMMER Phase 3, STEP, and SELECT trial data.
Verdict at a Glance
Ecnoglutide's biased GLP-1 signaling represents a scientifically novel approach, and SLIMMER Phase 3 data (15.4% weight loss at 48 weeks) are comparable to semaglutide's STEP 1 results (14.9% at 68 weeks). However, the comparison is limited by population differences (Chinese adults vs global populations), different trial durations, and vastly different evidence bases. Semaglutide has proven cardiovascular benefit, 7+ years of safety data, and global availability. Ecnoglutide may offer a competitive alternative in certain markets, particularly China, but its biased signaling advantage has not yet been demonstrated in head-to-head comparison with semaglutide.
| Best for | Pick | Why |
|---|---|---|
| Proven Treatment Today | Semaglutide | Semaglutide is FDA-approved, globally available, and backed by 25,000+ trial participants and 7+ years of real-world data. Ecnoglutide is not approved in any market. |
| Cardiovascular Risk Reduction | Semaglutide | SELECT demonstrated 20% MACE reduction with semaglutide 2.4 mg in 17,604 patients. Ecnoglutide has no cardiovascular outcomes data. |
| Oral Treatment Option | Semaglutide | Rybelsus (oral semaglutide) is FDA-approved. Ecnoglutide is available only as a weekly injection with no oral formulation in development. |
| Chinese Market Treatment | Ecnoglutide | SLIMMER Phase 3 was conducted in Chinese adults and demonstrated strong efficacy (15.4% weight loss at 48 weeks). Ecnoglutide may be the first locally developed GLP-1 agonist approved in China for obesity. |
| Biased Signaling Approach | Ecnoglutide | Ecnoglutide's cAMP-biased signaling may reduce receptor desensitization over time, potentially maintaining efficacy with chronic dosing. This remains a theoretical advantage requiring head-to-head validation. |
| Category | Ecnoglutide | Semaglutide | Advantage |
|---|---|---|---|
| Mechanism of Action | cAMP signaling-biased GLP-1 receptor agonist. Preferentially activates G protein-cAMP signaling over beta-arrestin recruitment, potentially reducing receptor desensitization. Made entirely of natural amino acids. | Selective GLP-1 receptor agonist with balanced G protein and beta-arrestin signaling. Activates GLP-1 receptors for appetite suppression, gastric emptying delay, and glucose homeostasis. C18 fatty diacid enables albumin binding for weekly dosing. | Ecnoglutide |
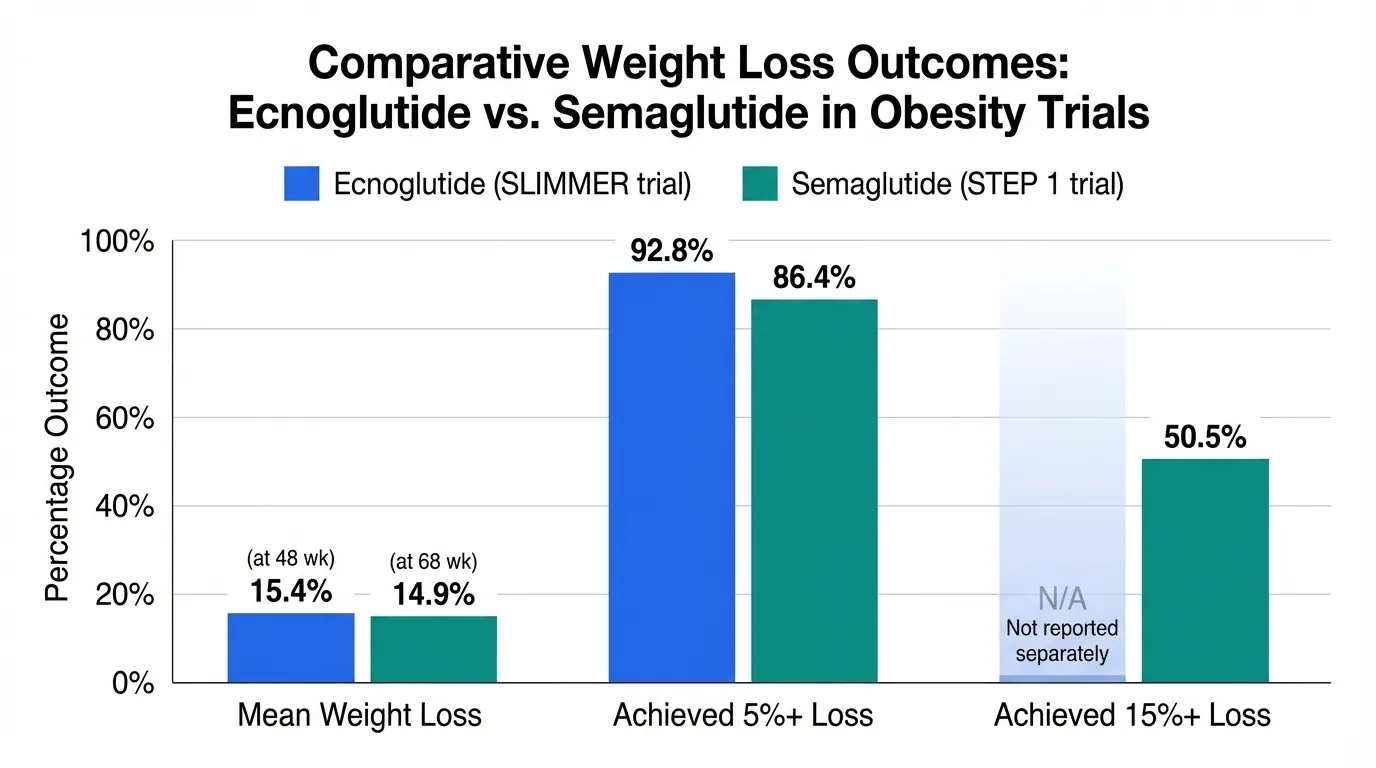
| Weight Loss Efficacy | SLIMMER Phase 3 showed 15.4% mean weight loss at 2.4 mg at 48 weeks (Chinese population), with 92.8% achieving 5% or more loss. Phase 2b showed 11.1% at 2.4 mg at 18 weeks, superior to liraglutide 3 mg. | STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. STEP 3 showed 16.0% with intensive lifestyle. 50.5% achieved 15% or more loss. Reproducible across multiple large Phase 3 trials. | Comparable |
| Development Stage and Evidence | Phase 3 SLIMMER completed (664 patients, 48 weeks, Lancet Diabetes Endocrinol). Phase 2 T2D completed. Phase 2b obesity completed in Australia/NZ. Not approved in any market. No global Phase 3 program. | FDA-approved since 2017 for T2D, 2021 for obesity. Over 25,000 clinical trial participants across SUSTAIN, PIONEER, STEP, SELECT programs. 7+ years of post-marketing surveillance. Global standard of care. | Semaglutide |
| Safety Profile | GI adverse events most common. Biased signaling may theoretically reduce receptor desensitization. SLIMMER showed acceptable safety in 664 patients. Limited long-term and post-marketing data. | Well-characterized over 7+ years. Proven CV safety (SELECT, 20% MACE reduction in 17,604 patients). Known GI side effect profile with extensive post-marketing surveillance identifying rare events. | Semaglutide |
| Cost and Accessibility | Not approved or commercially available in any market. Development focused primarily on China. No global regulatory filings. Uses natural amino acids, potentially simplifying manufacturing. | Widely available globally as Ozempic (T2D), Wegovy (obesity), and Rybelsus (oral). Multiple formulations. Established supply chain though shortages have occurred. Insurance coverage expanding. | Semaglutide |

Introduction#
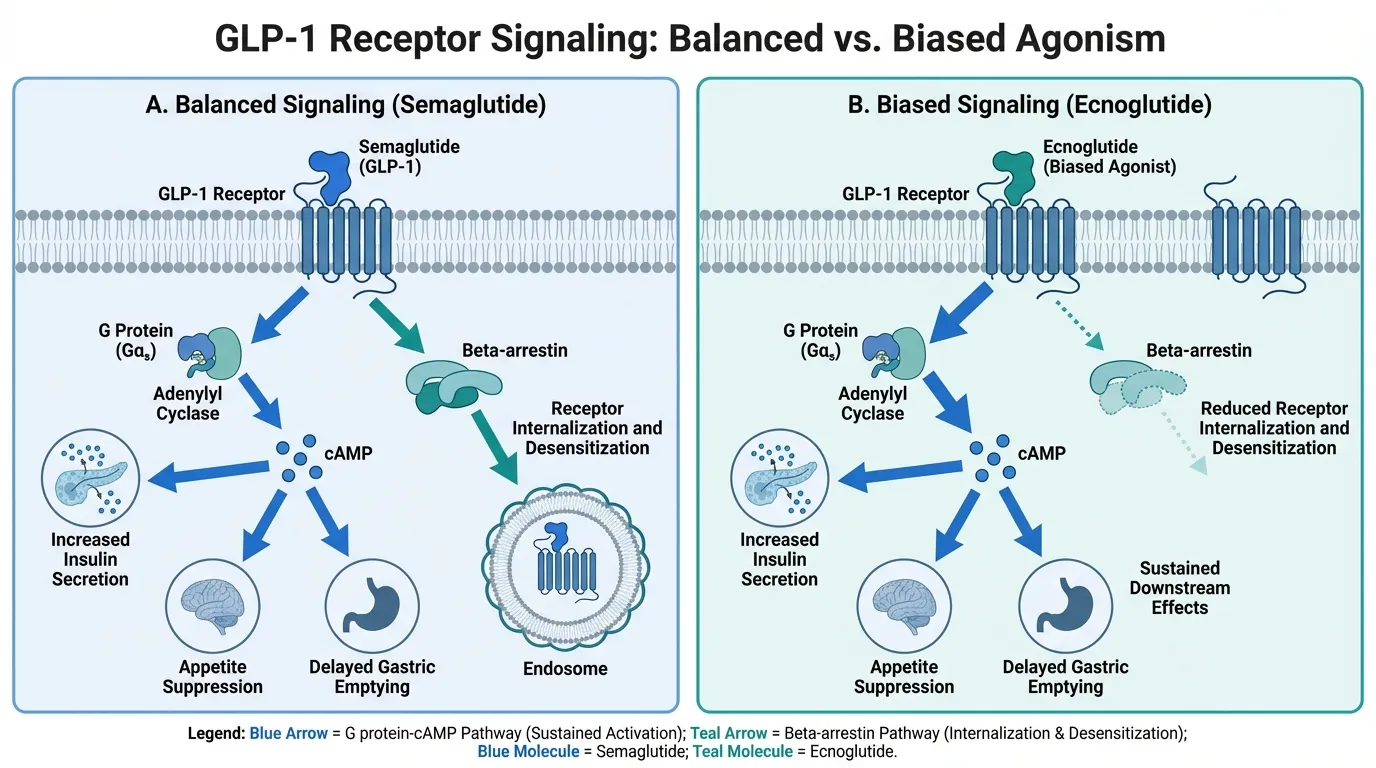
Ecnoglutide (XW003, Sciwind Biosciences) and semaglutide (Novo Nordisk) are both GLP-1 receptor agonists for obesity and type 2 diabetes, but they differ fundamentally in their signaling pharmacology. Semaglutide is the established global standard of care with balanced GLP-1 receptor signaling. Ecnoglutide is a novel cAMP signaling-biased agonist that preferentially activates G protein pathways over beta-arrestin recruitment, which may reduce receptor desensitization and potentially improve long-term efficacy.
The SLIMMER Phase 3 trial positioned ecnoglutide as a competitive GLP-1 agonist, with 15.4% weight loss at 48 weeks that approaches semaglutide's established efficacy, though the comparison is limited by differences in trial populations and duration.
Mechanism of Action Comparison#
Ecnoglutide#
Ecnoglutide is a long-acting, cAMP signaling-biased GLP-1 receptor agonist. It preferentially activates the G protein-cAMP pathway over beta-arrestin recruitment at the GLP-1 receptor. This biased signaling profile may reduce receptor internalization and desensitization, theoretically maintaining receptor responsiveness with chronic treatment. Ecnoglutide is composed entirely of natural amino acids with a C18 fatty diacid at Lys26 for albumin binding and extended half-life.
Semaglutide#
Semaglutide activates GLP-1 receptors with balanced G protein and beta-arrestin signaling. It suppresses appetite, delays gastric emptying, and enhances glucose-dependent insulin secretion. A C18 fatty diacid linker enables albumin binding for once-weekly pharmacokinetics.
Biased vs Balanced Signaling#
| Feature | Ecnoglutide | Semaglutide |
|---|---|---|
| Receptor target | GLP-1R (biased) | GLP-1R (balanced) |
| G protein-cAMP | Preferentially activated | Fully activated |
| Beta-arrestin | Reduced recruitment | Full recruitment |
| Receptor desensitization | Potentially reduced | Standard |
| Amino acid composition | All natural | Modified backbone |
| Administration | Weekly SC injection | Weekly SC or daily oral |
Weight Loss Data#
| Parameter | Ecnoglutide (SLIMMER) | Semaglutide (STEP 1) |
|---|---|---|
| Mean weight loss | 15.4% at 48 wk | 14.9% at 68 wk |
| Achieved 5%+ loss | 92.8% | 86.4% |
| Achieved 15%+ loss | Not reported separately | 50.5% |
| Population | Chinese adults | Global (multinational) |
| Sample size | 664 patients | 1,961 patients |
| Trial phase | Phase 3 | Phase 3 |
| Publication | Lancet Diabetes Endocrinol | NEJM |
Important caveat: The SLIMMER trial was conducted in a Chinese population only, which may have different body composition, baseline BMI distribution, and metabolic characteristics compared to the global populations studied in STEP trials. Cross-trial comparison is inherently limited.
Safety Comparison#
| Parameter | Ecnoglutide | Semaglutide |
|---|---|---|
| Total patients studied | ~1,000 | 25,000+ |
| GI events | Most common AE | Most common AE |
| CV outcomes data | None | SELECT (20% MACE reduction) |
| Long-term data | Up to 48 weeks | 7+ years |
| Post-marketing surveillance | None | Extensive |
Key Differences Summary#
- Signaling bias: Ecnoglutide is cAMP-biased; semaglutide has balanced signaling
- Weight loss: Comparable Phase 3 results (~15%), but different populations and durations
- Evidence base: Semaglutide has 25,000+ patients and 7+ years; ecnoglutide has ~1,000 patients
- CV benefit: Semaglutide has proven 20% MACE reduction; ecnoglutide has no CV data
- Availability: Semaglutide is globally available; ecnoglutide is not approved anywhere
- Formulations: Semaglutide has SC + oral; ecnoglutide is SC-only
- Geographic focus: Ecnoglutide development focused on China; semaglutide is global
Conclusion#
Ecnoglutide's cAMP-biased signaling is a scientifically intriguing approach that could theoretically offer advantages in long-term receptor responsiveness. The SLIMMER Phase 3 results are competitive with semaglutide, but the comparison is limited by the Chinese-only population, shorter trial duration, and absence of cardiovascular outcomes data. Semaglutide remains the proven global standard with an unmatched evidence base, cardiovascular benefit, multiple formulations, and years of real-world experience. Ecnoglutide may become an important regional competitor, particularly in China, but global head-to-head data against semaglutide would be needed to establish clinical superiority based on its biased signaling profile.
Detailed Category Analysis#
Mechanism of Action#
Ecnoglutide: cAMP signaling-biased GLP-1 receptor agonist. Preferentially activates G protein-cAMP signaling over beta-arrestin recruitment, potentially reducing receptor desensitization. Made entirely of natural amino acids.
Semaglutide: Selective GLP-1 receptor agonist with balanced G protein and beta-arrestin signaling. Activates GLP-1 receptors for appetite suppression, gastric emptying delay, and glucose homeostasis. C18 fatty diacid enables albumin binding for weekly dosing.
Advantage: Ecnoglutide
Weight Loss Efficacy#
Ecnoglutide: SLIMMER Phase 3 showed 15.4% mean weight loss at 2.4 mg at 48 weeks (Chinese population), with 92.8% achieving 5% or more loss. Phase 2b showed 11.1% at 2.4 mg at 18 weeks, superior to liraglutide 3 mg.
Semaglutide: STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. STEP 3 showed 16.0% with intensive lifestyle. 50.5% achieved 15% or more loss. Reproducible across multiple large Phase 3 trials.
Advantage: Neither (tie)
Development Stage and Evidence#
Ecnoglutide: Phase 3 SLIMMER completed (664 patients, 48 weeks, Lancet Diabetes Endocrinol). Phase 2 T2D completed. Phase 2b obesity completed in Australia/NZ. Not approved in any market. No global Phase 3 program.
Semaglutide: FDA-approved since 2017 for T2D, 2021 for obesity. Over 25,000 clinical trial participants across SUSTAIN, PIONEER, STEP, SELECT programs. 7+ years of post-marketing surveillance. Global standard of care.
Advantage: Semaglutide
Safety Profile#
Ecnoglutide: GI adverse events most common. Biased signaling may theoretically reduce receptor desensitization. SLIMMER showed acceptable safety in 664 patients. Limited long-term and post-marketing data.
Semaglutide: Well-characterized over 7+ years. Proven CV safety (SELECT, 20% MACE reduction in 17,604 patients). Known GI side effect profile with extensive post-marketing surveillance identifying rare events.
Advantage: Semaglutide
Cost and Accessibility#
Ecnoglutide: Not approved or commercially available in any market. Development focused primarily on China. No global regulatory filings. Uses natural amino acids, potentially simplifying manufacturing.
Semaglutide: Widely available globally as Ozempic (T2D), Wegovy (obesity), and Rybelsus (oral). Multiple formulations. Established supply chain though shortages have occurred. Insurance coverage expanding.
Advantage: Semaglutide
Summary and Verdict#
Ecnoglutide's biased GLP-1 signaling represents a scientifically novel approach, and SLIMMER Phase 3 data (15.4% weight loss at 48 weeks) are comparable to semaglutide's STEP 1 results (14.9% at 68 weeks). However, the comparison is limited by population differences (Chinese adults vs global populations), different trial durations, and vastly different evidence bases. Semaglutide has proven cardiovascular benefit, 7+ years of safety data, and global availability. Ecnoglutide may offer a competitive alternative in certain markets, particularly China, but its biased signaling advantage has not yet been demonstrated in head-to-head comparison with semaglutide.
Best For Recommendations#
Proven Treatment Today#
Recommendation: Semaglutide
Reason: Semaglutide is FDA-approved, globally available, and backed by 25,000+ trial participants and 7+ years of real-world data. Ecnoglutide is not approved in any market.
Cardiovascular Risk Reduction#
Recommendation: Semaglutide
Reason: SELECT demonstrated 20% MACE reduction with semaglutide 2.4 mg in 17,604 patients. Ecnoglutide has no cardiovascular outcomes data.
Oral Treatment Option#
Recommendation: Semaglutide
Reason: Rybelsus (oral semaglutide) is FDA-approved. Ecnoglutide is available only as a weekly injection with no oral formulation in development.
Chinese Market Treatment#
Recommendation: Ecnoglutide
Reason: SLIMMER Phase 3 was conducted in Chinese adults and demonstrated strong efficacy (15.4% weight loss at 48 weeks). Ecnoglutide may be the first locally developed GLP-1 agonist approved in China for obesity.
Biased Signaling Approach#
Recommendation: Ecnoglutide
Reason: Ecnoglutide's cAMP-biased signaling may reduce receptor desensitization over time, potentially maintaining efficacy with chronic dosing. This remains a theoretical advantage requiring head-to-head validation.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Proven Treatment Today
Semaglutide
Semaglutide is FDA-approved, globally available, and backed by 25,000+ trial participants and 7+ years of real-world data. Ecnoglutide is not approved in any market.
Cardiovascular Risk Reduction
Semaglutide
SELECT demonstrated 20% MACE reduction with semaglutide 2.4 mg in 17,604 patients. Ecnoglutide has no cardiovascular outcomes data.
Oral Treatment Option
Semaglutide
Rybelsus (oral semaglutide) is FDA-approved. Ecnoglutide is available only as a weekly injection with no oral formulation in development.
Chinese Market Treatment
Ecnoglutide
SLIMMER Phase 3 was conducted in Chinese adults and demonstrated strong efficacy (15.4% weight loss at 48 weeks). Ecnoglutide may be the first locally developed GLP-1 agonist approved in China for obesity.
Biased Signaling Approach
Ecnoglutide
Ecnoglutide's cAMP-biased signaling may reduce receptor desensitization over time, potentially maintaining efficacy with chronic dosing. This remains a theoretical advantage requiring head-to-head validation.
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Ecnoglutide vs Semaglutide: Biased GLP-1 Agonist vs Proven Standard of Care
Which is better, Ecnoglutide or Semaglutide?
Ecnoglutide's biased GLP-1 signaling represents a scientifically novel approach, and SLIMMER Phase 3 data (15.4% weight loss at 48 weeks) are comparable to semaglutide's STEP 1 results (14.9% at 68 weeks). However, the comparison is limited by population differences (Chinese adults vs global populations), different trial durations, and vastly different evidence bases. Semaglutide has proven cardiovascular benefit, 7+ years of safety data, and global availability. Ecnoglutide may offer a compe... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Ecnoglutide and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Ecnoglutide; Weight Loss Efficacy: advantage goes to neither (tie); Development Stage and Evidence: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Ecnoglutide?
For the scenario of "Proven Treatment Today," research data suggests Semaglutide may be more relevant. Semaglutide is FDA-approved, globally available, and backed by 25,000+ trial participants and 7+ years of real-world data. Ecnoglutide is not approved in any market.. This is based on currently available evidence and individual circumstances may differ.
How do Ecnoglutide and Semaglutide differ in their mechanisms of action?
Ecnoglutide: cAMP signaling-biased GLP-1 receptor agonist. Preferentially activates G protein-cAMP signaling over beta-arrestin recruitment, potentially reducing receptor desensitization. Made entirely of natur.... Semaglutide: Selective GLP-1 receptor agonist with balanced G protein and beta-arrestin signaling. Activates GLP-1 receptors for appetite suppression, gastric emptying delay, and glucose homeostasis. C18 fatty ....
Which has fewer side effects, Ecnoglutide or Semaglutide?
In terms of side effects and tolerability, the advantage goes to Semaglutide. Ecnoglutide: GI adverse events most common. Biased signaling may theoretically reduce receptor desensitization. SLIMMER showed acceptable safety in 664 patients.... Semaglutide: Well-characterized over 7+ years. Proven CV safety (SELECT, 20% MACE reduction in 17,604 patients). Known GI side effect profile with extensive pos....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.