Exenatide vs Semaglutide: First GLP-1 Agonist vs Current Standard
Evidence-based comparison of exenatide (Byetta/Bydureon) and semaglutide (Ozempic/Wegovy), covering the evolution from exendin-4-based to human GLP-1-based analogs, DURATION vs STEP trial data, and cardiovascular outcomes.
Verdict at a Glance
Semaglutide is substantially superior to exenatide in weight loss efficacy (14.9% vs 2-4%), glycemic control (SUSTAIN 3 head-to-head), cardiovascular outcomes (proven superiority vs non-inferiority only), and dosing convenience (pre-filled weekly pen vs reconstitution). Exenatide holds historical significance as the first GLP-1 agonist (FDA 2005) and may still serve as a lower-cost alternative in markets where newer agents are unavailable. However, for most clinical applications, semaglutide has effectively superseded exenatide.
| Best for | Pick | Why |
|---|---|---|
| Maximum weight loss | Semaglutide | 14.9% mean weight loss in STEP 1 vs 2-4% with exenatide; semaglutide is the only one approved for obesity treatment |
| Type 2 diabetes with cardiovascular risk | Semaglutide | Proven 20% MACE reduction in SELECT (obesity) and 26% in SUSTAIN 6 (T2D), while exenatide only achieved non-inferiority in EXSCEL |
| Budget-conscious diabetes treatment | Exenatide | Lower cost and generic availability make exenatide accessible when newer agents are unaffordable or not covered by formulary |
| Oral medication preference | Semaglutide | Rybelsus (oral semaglutide) offers injection-free GLP-1 therapy; exenatide has no oral formulation |
| Historical perspective or formulary restrictions | Exenatide | May remain on formularies where newer agents face access restrictions; 20 years of post-marketing safety data |
| Category | Exenatide | Semaglutide | Advantage |
|---|---|---|---|
| Mechanism of Action | Synthetic version of exendin-4, a GLP-1 receptor agonist originally isolated from Gila monster (Heloderma suspectum) venom. 53% homology to human GLP-1. Available as twice-daily immediate-release (Byetta) or once-weekly extended-release microsphere (Bydureon). FDA approved 2005. | Synthetic analog of human GLP-1 with 94% homology. C18 fatty diacid modification enables strong albumin binding and a 165-hour half-life for once-weekly injection. Also available as daily oral tablet (Rybelsus). FDA approved 2017. Represents a generational advance in GLP-1 design. | Semaglutide |
| Weight Loss Efficacy | Modest weight loss of 2-4 kg (2-4%) over 24-30 weeks in DURATION trials. Not FDA-approved for weight management. Weight loss is a secondary benefit in diabetes treatment, not a primary indication. | STEP 1 demonstrated 14.9% mean weight loss at 2.4 mg over 68 weeks. FDA-approved for chronic weight management (Wegovy). Approximately 4-5 fold greater weight reduction than exenatide in cross-trial comparisons. | Semaglutide |
| Glycemic Control | DURATION-1 showed HbA1c reduction of 1.9% with Bydureon over 30 weeks. Effective for type 2 diabetes glycemic control. Proven across multiple DURATION trials with consistent HbA1c lowering of 1.1-2.0%. | SUSTAIN trials showed HbA1c reduction of 1.5-1.8% at 0.5-1.0 mg over 30-56 weeks. PIONEER trials confirmed oral semaglutide efficacy. Superior to many comparators including exenatide ER in the SUSTAIN 3 trial (1.5% vs 0.9% HbA1c reduction). | Semaglutide |
| Cardiovascular Outcomes | EXSCEL trial (14,752 patients) showed trend toward MACE reduction (HR 0.91) but did not achieve statistical superiority (p=0.06). Achieved non-inferiority only. 14% reduction in all-cause mortality was a secondary finding. | SELECT trial (17,604 patients) demonstrated statistically significant 20% MACE reduction in overweight/obese adults without diabetes. SUSTAIN 6 showed 26% MACE reduction in T2D. Proven cardiovascular superiority. | Semaglutide |
| Practical Considerations | Lower cost, longer market availability (2005), and established generic competition. Bydureon requires reconstitution (pen version simplifies this). Available as an option when newer agents are inaccessible or not covered by insurance. | Higher cost but markedly superior efficacy. Pre-filled pen requires no reconstitution. Weekly injection or daily oral options. Wider insurance coverage for obesity indication. Dominant market position. | Comparable |

Introduction#
Exenatide and semaglutide represent two generations of GLP-1 receptor agonist therapy, separated by more than a decade of pharmaceutical development. Exenatide (Byetta/Bydureon) was the first GLP-1 receptor agonist to reach the market (FDA 2005), derived from the venom peptide exendin-4 found in the Gila monster lizard. Semaglutide (Ozempic/Wegovy/Rybelsus) arrived in 2017 as a second-generation human GLP-1 analog with fundamentally improved pharmacokinetics and clinical outcomes.
This comparison examines the substantial differences between these agents, including the SUSTAIN 3 head-to-head trial, independent program data, cardiovascular outcomes, and the practical implications of choosing between a pioneering agent and its modern successor.
Mechanism of Action Comparison#
Exenatide: Exendin-4 Based#
Exenatide is a synthetic 39-amino acid peptide identical to exendin-4, a naturally occurring GLP-1 receptor agonist found in the saliva of the Gila monster (Heloderma suspectum). It shares only 53% amino acid homology with human GLP-1 but is a full agonist at the GLP-1 receptor. Exendin-4 is naturally resistant to DPP-4 degradation due to its non-human sequence.
- Byetta (immediate-release): Half-life of 2.4 hours, requiring twice-daily subcutaneous injection 60 minutes before meals
- Bydureon (extended-release): Exenatide encapsulated in biodegradable poly(D,L-lactide-co-glycolide) microspheres that release the peptide over weeks, enabling once-weekly dosing with a half-life of approximately 2 weeks
Semaglutide: Human GLP-1 Based#
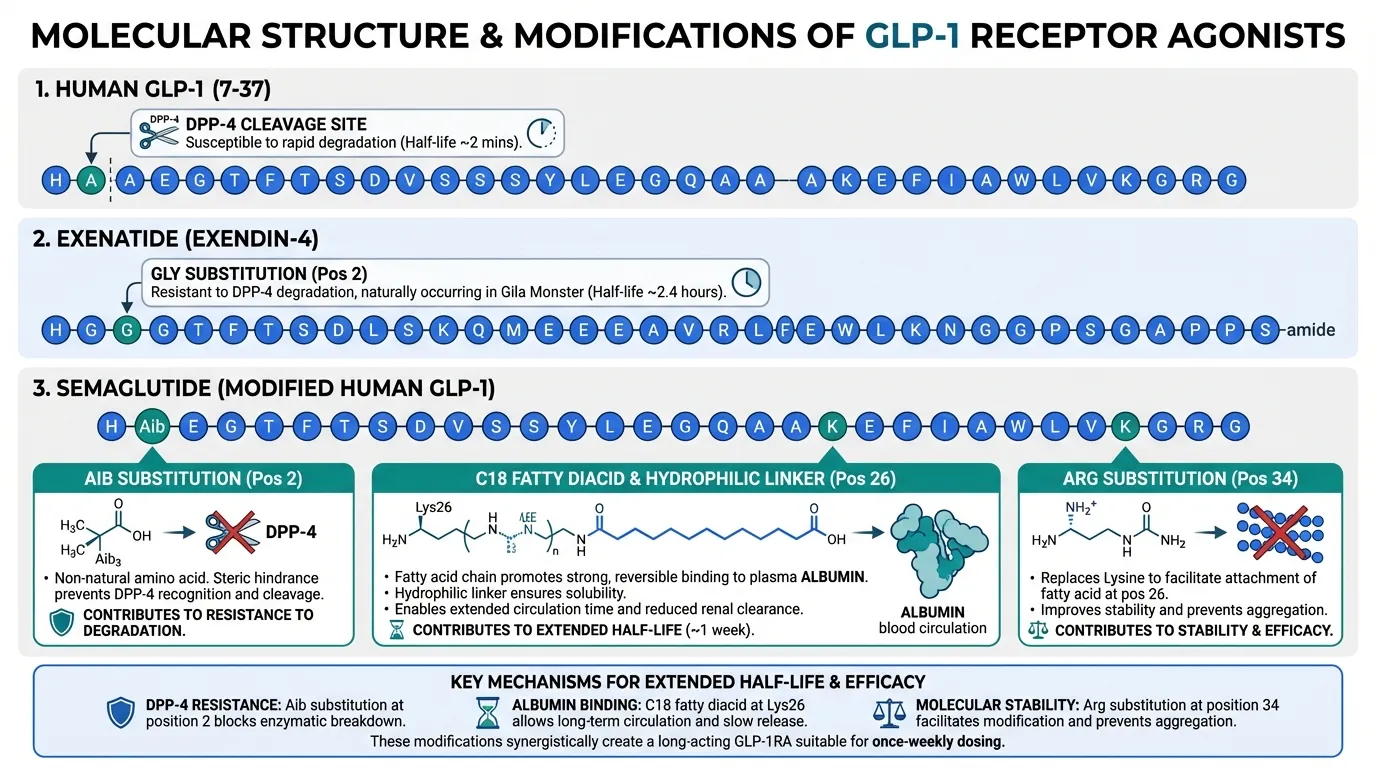
Semaglutide is a 31-amino acid peptide with 94% homology to native human GLP-1. Three key modifications optimize its pharmacokinetics:
- Aib substitution at position 2 resists DPP-4 cleavage
- C18 fatty diacid via a hydrophilic linker at Lys26 enables strong, non-covalent albumin binding
- Arg substitution at position 34 prevents fatty acid binding at the wrong site
These modifications produce a half-life of approximately 165 hours (7 days), enabling true once-weekly pharmacokinetics without microsphere encapsulation, plus a daily oral formulation (Rybelsus) using the SNAC absorption enhancer.
Pharmacokinetic Comparison#
| Property | Exenatide (Byetta) | Exenatide ER (Bydureon) | Semaglutide (injection) |
|---|---|---|---|
| Source | Exendin-4 (Gila monster) | Exendin-4 (Gila monster) | Human GLP-1 analog |
| GLP-1 homology | 53% | 53% | 94% |
| Half-life | 2.4 hours | ~2 weeks (release-limited) | ~165 hours |
| Dosing | Twice daily | Once weekly | Once weekly |
| Delivery | Pre-filled pen | Reconstitution required | Pre-filled pen |
| Oral option | No | No | Yes (Rybelsus) |
Weight Loss Efficacy#
Exenatide#
Exenatide was never developed primarily for weight management. In the DURATION program for type 2 diabetes:
- DURATION-1: Exenatide ER (Bydureon) 2 mg weekly produced 3.7 kg weight loss over 30 weeks
- DURATION-5: Bydureon produced 2.3 kg weight loss over 24 weeks
- Three-year data: Sustained weight reduction of approximately 2.3 kg (5.1 lbs) from baseline
Exenatide is not FDA-approved for chronic weight management. Its weight loss effect is considered modest and secondary to its glucose-lowering indication.
Semaglutide#
Semaglutide was specifically developed and approved for weight management at higher doses:
- STEP 1 (1,961 adults without T2D): 14.9% mean weight loss at 2.4 mg over 68 weeks; 86.4% achieved 5% or more loss; 50.5% achieved 15% or more
- STEP 2 (1,210 adults with T2D): 9.6% mean weight loss at 2.4 mg over 68 weeks
- STEP 3 (with intensive behavioral therapy): 16.0% mean weight loss
The magnitude difference is approximately 4-5 fold in favor of semaglutide. This reflects both the higher dose used for obesity (2.4 mg vs typical diabetes doses) and the superior pharmacological properties of the molecule.
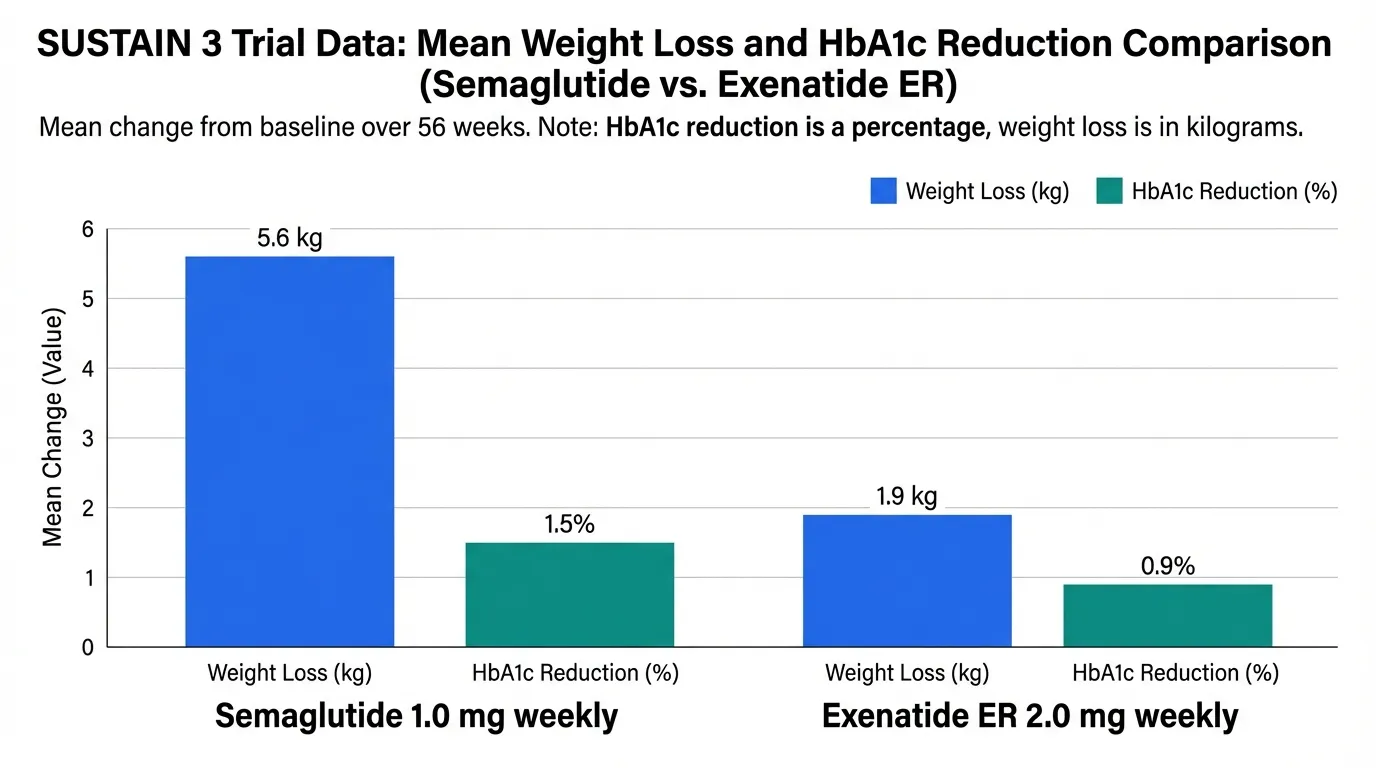
SUSTAIN 3: Head-to-Head for Diabetes#
The SUSTAIN 3 trial directly compared semaglutide 1.0 mg weekly to exenatide ER 2.0 mg weekly in 813 patients with type 2 diabetes over 56 weeks. Semaglutide was superior for both glycemic control (HbA1c reduction 1.5% vs 0.9%) and weight loss (5.6 kg vs 1.9 kg).
Cardiovascular Outcomes#
EXSCEL Trial (Exenatide)#
The EXSCEL trial (Holman et al., NEJM 2017) enrolled 14,752 patients with type 2 diabetes (73.1% with prior cardiovascular disease) and followed them for a median of 3.2 years:
- Primary MACE endpoint: HR 0.91 (95% CI 0.83-1.00), p=0.06 for superiority
- Met non-inferiority but narrowly missed superiority (p=0.06)
- All-cause mortality was reduced by 14% (HR 0.86, p=0.016) in a secondary analysis
EXSCEL confirmed cardiovascular safety but did not prove cardiovascular benefit -- a critical distinction.
SELECT Trial (Semaglutide)#
The SELECT trial (Lincoff et al., NEJM 2023) enrolled 17,604 adults with overweight/obesity and established cardiovascular disease, but without diabetes:
- Primary MACE endpoint: HR 0.80 (95% CI 0.72-0.90), p<0.001
- 20% reduction in MACE -- statistically significant superiority
- First trial to demonstrate GLP-1 agonist cardiovascular benefit in non-diabetic obesity
The difference in cardiovascular evidence is substantial: exenatide achieved only non-inferiority, while semaglutide demonstrated clear superiority.
Dosing and Administration#
Exenatide#
- Byetta: 5 mcg twice daily for 1 month, then 10 mcg twice daily; inject 60 minutes before meals
- Bydureon: 2 mg once weekly; any time of day regardless of meals; requires reconstitution (microsphere suspension)
- Bydureon BCise: Auto-injector that simplifies reconstitution
Semaglutide#
- Ozempic (T2D): 0.25 mg weekly for 4 weeks, then 0.5 mg, max 2.0 mg weekly
- Wegovy (obesity): 0.25 mg weekly, titrate monthly to 2.4 mg weekly (16-week escalation)
- Rybelsus (T2D): 3 mg daily oral for 30 days, then 7 mg, max 14 mg; empty stomach
- Pre-filled pen, no reconstitution needed
Safety Comparison#
Both agents share the GLP-1 agonist class side effect profile: nausea, vomiting, diarrhea, constipation, and abdominal pain, predominantly during dose escalation. Key differences:
| Safety Aspect | Exenatide | Semaglutide |
|---|---|---|
| GI adverse events | ~40-50% | ~50-70% (higher dose) |
| Injection site reactions | Common with Bydureon (nodules) | Rare |
| Anti-drug antibodies | Common (~45% with Bydureon) | Rare (<1%) |
| Pancreatitis signal | Post-marketing reports | Post-marketing reports |
| Thyroid C-cell warning | Boxed warning (rodent data) | Boxed warning (rodent data) |
| Post-marketing experience | 20+ years (since 2005) | 8+ years (since 2017) |
Exenatide ER (Bydureon) is notable for injection site reactions, including subcutaneous nodules at the injection site caused by the microsphere formulation. Anti-drug antibodies develop in approximately 45% of patients treated with Bydureon, though they rarely affect efficacy.
Key Differences Summary#
| Feature | Exenatide | Semaglutide |
|---|---|---|
| Origin | Gila monster venom peptide | Human GLP-1 analog |
| FDA approval | 2005 (first GLP-1 agonist) | 2017 |
| Obesity indication | No | Yes (Wegovy) |
| Weight loss | 2-4% (T2D trials) | 14.9% (STEP 1, obesity) |
| HbA1c reduction | 1.1-2.0% | 1.5-1.8% (superior in SUSTAIN 3) |
| CV outcomes | Non-inferiority only (EXSCEL) | Superiority proven (SELECT) |
| Oral formulation | No | Yes (Rybelsus) |
| Injection site nodules | Yes (Bydureon) | No |
| Cost | Lower (generics available) | Higher (patent-protected) |
Conclusion#
Exenatide holds an important place in pharmaceutical history as the first GLP-1 receptor agonist, proving that this receptor could be targeted for type 2 diabetes treatment and opening the door for all subsequent agents. However, semaglutide has comprehensively surpassed exenatide in every clinical dimension: weight loss efficacy (approximately 4-5 fold greater), glycemic control (superior in SUSTAIN 3 head-to-head), cardiovascular outcomes (proven superiority vs non-inferiority), dosing convenience (pre-filled pen without reconstitution), and formulation options (oral available). Exenatide may still serve a role in cost-constrained settings or when newer agents are unavailable, but semaglutide is the clear standard of care for new GLP-1 agonist prescriptions.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Maximum weight loss
Semaglutide
14.9% mean weight loss in STEP 1 vs 2-4% with exenatide; semaglutide is the only one approved for obesity treatment
Type 2 diabetes with cardiovascular risk
Semaglutide
Proven 20% MACE reduction in SELECT (obesity) and 26% in SUSTAIN 6 (T2D), while exenatide only achieved non-inferiority in EXSCEL
Budget-conscious diabetes treatment
Exenatide
Lower cost and generic availability make exenatide accessible when newer agents are unaffordable or not covered by formulary
Oral medication preference
Semaglutide
Rybelsus (oral semaglutide) offers injection-free GLP-1 therapy; exenatide has no oral formulation
Historical perspective or formulary restrictions
Exenatide
May remain on formularies where newer agents face access restrictions; 20 years of post-marketing safety data
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Exenatide vs Semaglutide: First GLP-1 Agonist vs Current Standard
Which is better, Exenatide or Semaglutide?
Semaglutide is substantially superior to exenatide in weight loss efficacy (14.9% vs 2-4%), glycemic control (SUSTAIN 3 head-to-head), cardiovascular outcomes (proven superiority vs non-inferiority only), and dosing convenience (pre-filled weekly pen vs reconstitution). Exenatide holds historical significance as the first GLP-1 agonist (FDA 2005) and may still serve as a lower-cost alternative in markets where newer agents are unavailable. However, for most clinical applications, semaglutide ... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between Exenatide and Semaglutide?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Semaglutide; Weight Loss Efficacy: advantage goes to Semaglutide; Glycemic Control: advantage goes to Semaglutide. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Semaglutide over Exenatide?
For the scenario of "Maximum weight loss," research data suggests Semaglutide may be more relevant. 14.9% mean weight loss in STEP 1 vs 2-4% with exenatide; semaglutide is the only one approved for obesity treatment. This is based on currently available evidence and individual circumstances may differ.
How do Exenatide and Semaglutide differ in their mechanisms of action?
Exenatide: Synthetic version of exendin-4, a GLP-1 receptor agonist originally isolated from Gila monster (Heloderma suspectum) venom. 53% homology to human GLP-1. Available as twice-daily immediate-release (.... Semaglutide: Synthetic analog of human GLP-1 with 94% homology. C18 fatty diacid modification enables strong albumin binding and a 165-hour half-life for once-weekly injection. Also available as daily oral tabl....
In what scenario might Semaglutide be preferred?
For "Type 2 diabetes with cardiovascular risk," Semaglutide may be more appropriate. Proven 20% MACE reduction in SELECT (obesity) and 26% in SUSTAIN 6 (T2D), while exenatide only achieved non-inferiority in EXSCEL. Individual factors and clinical context should guide any decisions.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.