Sermorelin vs Tesamorelin: GHRH Analogues Compared
Comparing sermorelin and tesamorelin as GHRH analogues, covering GH stimulation mechanisms, FDA approval status, visceral fat reduction, and clinical evidence.
Verdict at a Glance
Tesamorelin for proven metabolic indications with active FDA approval; sermorelin for broader GH research and combined GHRH/GHRP protocols through compounding access
| Best for | Pick | Why |
|---|---|---|
| HIV-Associated Lipodystrophy | Tesamorelin | Tesamorelin is the only FDA-approved treatment for HIV lipodystrophy, with Phase III data showing approximately 18% visceral fat reduction |
| Visceral Fat Reduction | Tesamorelin | Tesamorelin has the strongest clinical evidence for visceral adipose tissue reduction, with controlled trial data in HIV and emerging NASH data |
| Combined GHRH/GHRP Protocols | Sermorelin | Sermorelin shorter half-life makes it compatible with pulsatile dosing in combination with GHRPs like ipamorelin, and it is widely available through compounding pharmacies |
| GH Deficiency Diagnosis | Sermorelin | Sermorelin was specifically approved and validated for diagnostic GH stimulation testing, though the commercial product has been discontinued |
| NASH/Liver Fat Research | Tesamorelin | Tesamorelin is under investigation for nonalcoholic steatohepatitis, with clinical trials exploring liver fat reduction and fibrosis outcomes |
| Cost-Effective GH Stimulation | Sermorelin | Sermorelin is available through compounding pharmacies at substantially lower cost than branded tesamorelin (Egrifta) |
| Category | Sermorelin | Tesamorelin | Advantage |
|---|---|---|---|
| Mechanism of Action | GHRH(1-29) fragment; stimulates pituitary GH release through GHRH receptor; shorter analog of native GHRH preserving full biological activity | 44-amino acid GHRH analog with trans-3-hexenoic acid modification; enhanced stability against DPP-IV degradation; more potent than native GHRH | Tesamorelin |
| Research Evidence | Previously FDA-approved (Geref) for GH deficiency diagnosis; extensive clinical history; product commercially discontinued | Currently FDA-approved (Egrifta) for HIV lipodystrophy; ongoing NASH trials; active pharmaceutical product with post-marketing data | Tesamorelin |
| Side Effect Profile | Well-tolerated; injection site reactions; transient flushing; minimal systemic side effects; decades of clinical use data | Well-tolerated; injection site reactions; transient peripheral edema; arthralgia; monitored IGF-1 elevations; active pharmacovigilance | Comparable |
| Metabolic Effects | Physiological GH stimulation; body composition improvements observed in research; less studied for specific metabolic indications | Proven visceral fat reduction (~18% in HIV trials); improved lipid profiles; NASH/liver fat reduction under investigation | Tesamorelin |
| Regulatory Status | Geref discontinued (commercial reasons, not safety); available through compounding pharmacies; widely used off-label | FDA-approved (Egrifta) for HIV lipodystrophy; active commercial product; NDA holder Theratechnologies | Tesamorelin |

Introduction#
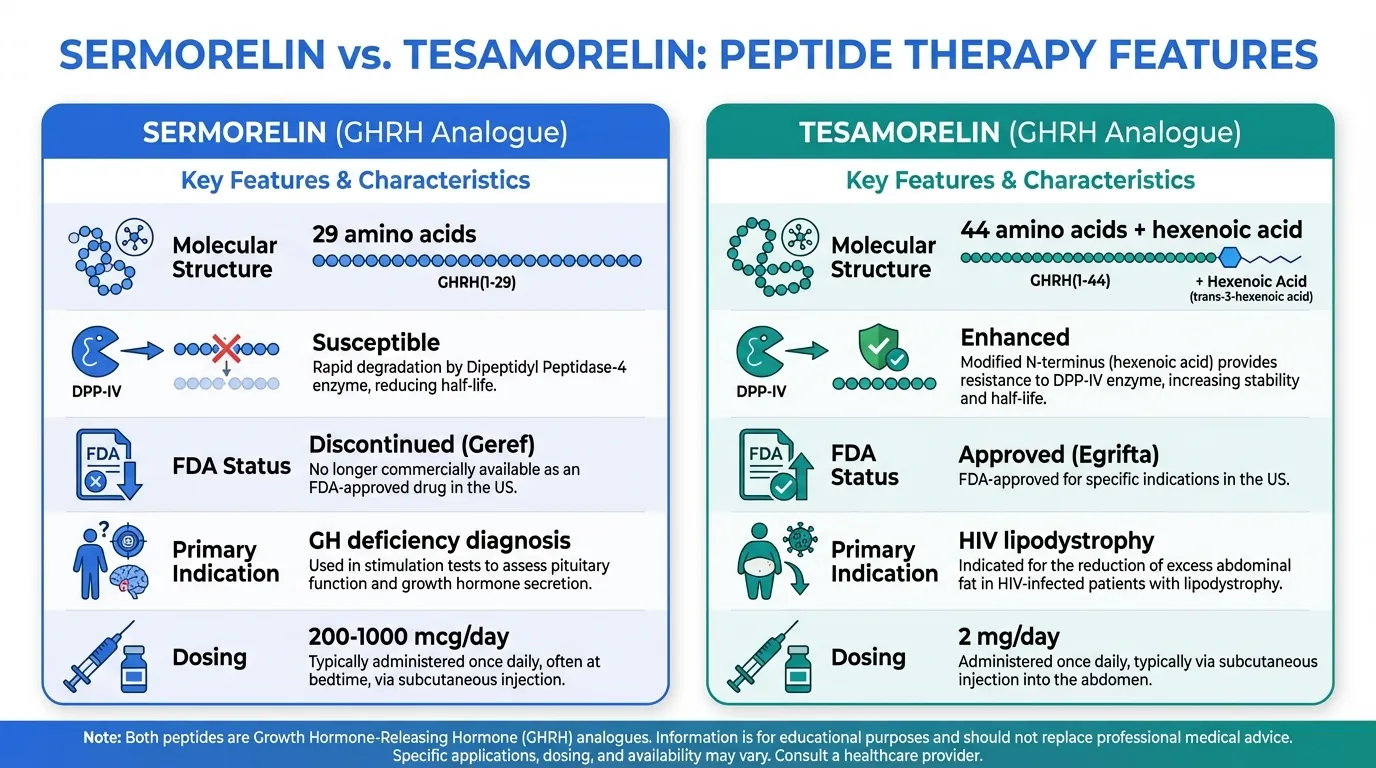
Sermorelin and Tesamorelin are both synthetic analogs of growth hormone-releasing hormone (GHRH) that stimulate endogenous GH production through the pituitary GHRH receptor. Despite sharing this fundamental mechanism, they differ substantially in molecular design, potency, clinical applications, regulatory status, and accessibility. Sermorelin is the shorter, simpler analog (29 amino acids) with historical FDA approval and broad compounding pharmacy availability, while tesamorelin is the larger, stabilized analog (44 amino acids) with current FDA approval for HIV lipodystrophy and emerging metabolic applications.
This comparison is particularly relevant because both peptides represent the GHRH pathway approach to GH stimulation, which preserves physiological pulsatile GH release and feedback mechanisms -- a key advantage over direct GH replacement.
Quick Comparison Table#
| Feature | Sermorelin | Tesamorelin |
|---|---|---|
| Structure | 29 amino acids (3357.88 Da) | 44 amino acids + hexenoic acid (5135.9 Da) |
| Mechanism | GHRH(1-29) fragment | Modified full-length GHRH analog |
| DPP-IV stability | Susceptible to degradation | Enhanced stability (hexenoic acid) |
| FDA status | Discontinued (Geref) | Approved (Egrifta) |
| Primary indication | GH deficiency diagnosis | HIV lipodystrophy |
| Dosing | SC, 200-1000 mcg/day (research) | SC, 2 mg/day |
| Availability | Compounding pharmacies | Prescription pharmaceutical |
Mechanism of Action Comparison#
Sermorelin#
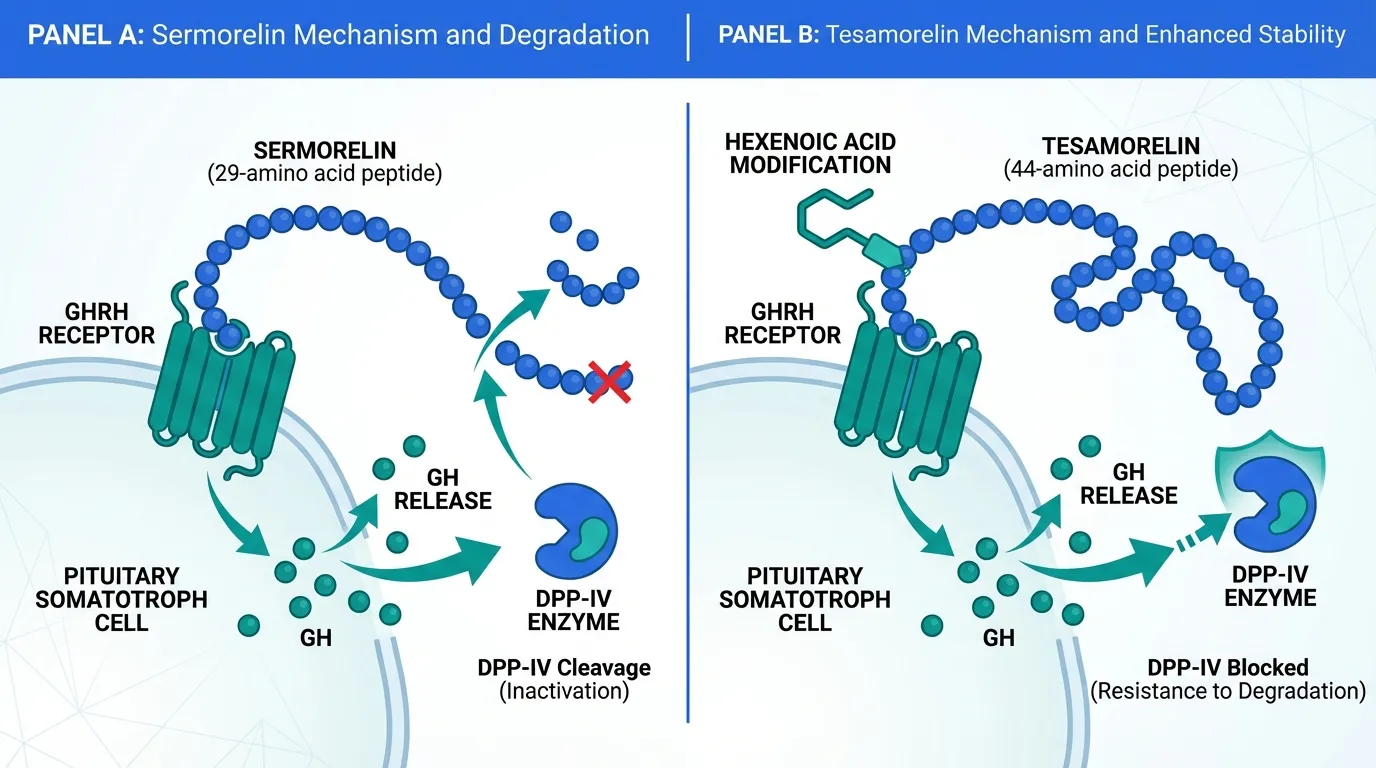
Sermorelin (GRF 1-29) is a truncated analog of native GHRH, consisting of the first 29 amino acids that contain the full biological activity domain. It binds to the GHRH receptor on pituitary somatotrophs, activating Gs-coupled adenylyl cyclase signaling, elevating cAMP, and stimulating GH synthesis and secretion.
As a faithful reproduction of the active GHRH fragment, sermorelin preserves the physiological pattern of pulsatile GH release and maintains intact negative feedback through IGF-1 and somatostatin. This means GH levels cannot rise to supraphysiological ranges under normal circumstances, an inherent safety feature of the GHRH pathway.
The primary pharmacological limitation of sermorelin is its susceptibility to dipeptidyl peptidase-IV (DPP-IV) degradation, which cleaves the N-terminal tyrosine-alanine dipeptide and inactivates the molecule. This rapid proteolytic metabolism results in a short plasma half-life and limits bioavailability.
Tesamorelin#
Tesamorelin (TH9507) is a full-length GHRH analog (all 44 amino acids) with a trans-3-hexenoic acid group conjugated to the N-terminal tyrosine. This lipophilic modification specifically protects against DPP-IV cleavage, the primary route of GHRH inactivation, resulting in enhanced potency and a longer duration of action compared to native GHRH and sermorelin.
The improved stability translates to more consistent GH stimulation per dose, supporting once-daily dosing at a fixed 2 mg dose. Like sermorelin, tesamorelin preserves pulsatile GH release and physiological feedback, but achieves more reliable pharmacological effects due to its resistance to enzymatic degradation.
Evidence and Research Comparison#
Sermorelin Clinical Evidence#
- FDA approval history: Approved as Geref for diagnostic evaluation of GH deficiency; commercially discontinued for business reasons (not safety concerns)
- GH stimulation: Well-validated dose-response in healthy and GH-deficient subjects
- Anti-aging research: Studied in aging populations for GH-mediated improvements in body composition, sleep quality, and skin thickness
- Combination protocols: Extensive use with GHRP peptides (ipamorelin, GHRP-2) for synergistic GH release
- Long clinical history: Decades of clinical pharmacology data and established safety profile
Tesamorelin Clinical Evidence#
- Phase III HIV lipodystrophy: Pivotal trials demonstrated approximately 18% reduction in visceral adipose tissue (VAT), improved lipid profiles (triglycerides, total cholesterol/HDL ratio), and maintained lean mass
- NASH investigation: Active clinical trials examining liver fat reduction and fibrosis in nonalcoholic steatohepatitis
- Cognitive function: Exploratory studies suggesting GH-mediated cognitive improvements in HIV patients
- Post-marketing data: Active pharmacovigilance from commercial use as Egrifta since 2010 approval
- Long-term safety: 26-week and extension studies with established safety monitoring protocols
Side Effects and Safety Comparison#
Sermorelin Side Effects#
- Injection site reactions: Most common; redness, swelling at injection site
- Transient flushing: Vasomotor response occasionally reported
- Headache: Infrequent
- Minimal systemic effects: Physiological GH release mechanism limits risk of GH excess
- Decades of safety data: Long clinical history without significant safety signals
Tesamorelin Side Effects#
- Injection site reactions: Most common adverse event in clinical trials
- Peripheral edema: Transient; GH-mediated fluid retention
- Arthralgia: Joint pain reported in some patients; GH-related
- IGF-1 elevation: Requires monitoring; typically returns to normal after discontinuation
- Glucose effects: May increase fasting glucose in some patients; monitored in HIV population
- Active pharmacovigilance: Post-marketing safety reporting since 2010
Dosing and Administration Comparison#
Sermorelin Dosing#
- Research doses: 200-1000 mcg per day, subcutaneous, typically at bedtime
- Combination dosing: Often administered with ipamorelin (200-300 mcg) for synergistic GH release
- Frequency: Daily or divided into multiple injections
- Availability: Compounding pharmacies; no branded product currently available
Tesamorelin Dosing#
- Approved dose: 2 mg subcutaneous injection once daily
- Fixed dosing: No dose titration required; single dose for all patients
- Administration: Self-injection into abdomen; rotate injection sites
- Commercial product: Available as Egrifta (lyophilized powder + diluent) or Egrifta SV (solution)
Can They Be Combined?#
Combining sermorelin and tesamorelin would not be rational as both target the same GHRH receptor with the same mechanism. The appropriate comparison is whether to use one GHRH analog alone or combine a GHRH analog with a GHS peptide (GHRP pathway) for synergistic GH release. Sermorelin is more commonly used in this combined approach due to its compounding availability and lower cost.
Verdict#
Tesamorelin is the superior choice when a specific metabolic indication requires proven GHRH-mediated intervention -- HIV lipodystrophy (FDA-approved), visceral fat reduction, and emerging NASH applications. Its enhanced stability, standardized pharmaceutical manufacturing, and active regulatory approval provide clinical confidence that sermorelin cannot match.
Sermorelin remains highly relevant for broader GH optimization research, particularly in combined GHRH/GHRP protocols where its synergy with ipamorelin or GHRP-2 is well-documented. Its availability through compounding pharmacies at significantly lower cost makes it the practical choice for researchers and clinicians outside the specific indications where tesamorelin excels.
Both peptides share the fundamental advantage of preserving physiological GH pulsatility, distinguishing them from direct GH replacement and making the GHRH pathway approach an attractive alternative for GH restoration.
Explore the full profiles of Sermorelin and Tesamorelin, or see how they compare to GHS peptides like Ipamorelin and GHRP-2. Use our Half-Life Comparison Tool for peptide pharmacokinetic comparisons.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
HIV-Associated Lipodystrophy
Tesamorelin
Tesamorelin is the only FDA-approved treatment for HIV lipodystrophy, with Phase III data showing approximately 18% visceral fat reduction
Visceral Fat Reduction
Tesamorelin
Tesamorelin has the strongest clinical evidence for visceral adipose tissue reduction, with controlled trial data in HIV and emerging NASH data
Combined GHRH/GHRP Protocols
Sermorelin
Sermorelin shorter half-life makes it compatible with pulsatile dosing in combination with GHRPs like ipamorelin, and it is widely available through compounding pharmacies
GH Deficiency Diagnosis
Sermorelin
Sermorelin was specifically approved and validated for diagnostic GH stimulation testing, though the commercial product has been discontinued
NASH/Liver Fat Research
Tesamorelin
Tesamorelin is under investigation for nonalcoholic steatohepatitis, with clinical trials exploring liver fat reduction and fibrosis outcomes
Cost-Effective GH Stimulation
Sermorelin
Sermorelin is available through compounding pharmacies at substantially lower cost than branded tesamorelin (Egrifta)
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About Sermorelin vs Tesamorelin: GHRH Analogues Compared
What are the key differences between Sermorelin and Tesamorelin?
The main differences across comparison categories are: Mechanism of Action: advantage goes to Tesamorelin; Research Evidence: advantage goes to Tesamorelin; Side Effect Profile: advantage goes to neither (tie). 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Tesamorelin over Sermorelin?
For the scenario of "HIV-Associated Lipodystrophy," research data suggests Tesamorelin may be more relevant. Tesamorelin is the only FDA-approved treatment for HIV lipodystrophy, with Phase III data showing approximately 18% visceral fat reduction. This is based on currently available evidence and individual circumstances may differ.
How do Sermorelin and Tesamorelin differ in their mechanisms of action?
Sermorelin: GHRH(1-29) fragment; stimulates pituitary GH release through GHRH receptor; shorter analog of native GHRH preserving full biological activity. Tesamorelin: 44-amino acid GHRH analog with trans-3-hexenoic acid modification; enhanced stability against DPP-IV degradation; more potent than native GHRH.
Which has fewer side effects, Sermorelin or Tesamorelin?
In terms of side effects and tolerability, the advantage goes to neither (comparable). Sermorelin: Well-tolerated; injection site reactions; transient flushing; minimal systemic side effects; decades of clinical use data. Tesamorelin: Well-tolerated; injection site reactions; transient peripheral edema; arthralgia; monitored IGF-1 elevations; active pharmacovigilance.
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.