Thymic Peptides Explained: How Thymosin Alpha-1, Thymalin, and Thymulin Shape Immunity

Introduction#
The thymus gland occupies a paradoxical position in human biology. It is essential for developing the adaptive immune system — producing the T-cells that protect against infections, cancer, and autoimmune disease — yet it begins to shrink before we reach adulthood. By age 65, the thymus has lost roughly 95% of its functional tissue, replaced by fat in a process called thymic involution. This progressive decline is now understood to be a major driver of immunosenescence, the age-related weakening of immune function that leaves older adults vulnerable to infections, reduced vaccine responses, and increased cancer risk.
Thymic peptides — bioactive molecules derived from or modeled on thymic tissue — represent one of the most direct approaches to addressing this fundamental problem. Rather than broadly stimulating or suppressing the immune system, thymic peptides aim to restore the specific immune functions that decline as the thymus atrophies. This guide examines four thymic and immune peptides with distinct evidence profiles: Thymosin Alpha-1, Thymalin, Vilon, and the innate immune peptide LL-37 for comparison.
The Thymus: Why It Matters for Immunity#
Thymic Function#
The thymus is a bilobed organ located behind the sternum that serves as the primary site of T-cell development. Bone marrow-derived progenitor cells migrate to the thymus, where they undergo a complex maturation process involving positive and negative selection. Positive selection ensures T-cells can recognize antigens presented by the body's own MHC molecules, while negative selection eliminates T-cells that react too strongly to self-antigens — a critical safeguard against autoimmune disease.
The thymus produces several classes of T-cells:
- CD4+ helper T-cells — coordinate immune responses by activating other immune cells
- CD8+ cytotoxic T-cells — directly kill virus-infected and cancerous cells
- Regulatory T-cells (Tregs) — suppress excessive immune responses and maintain tolerance
- Natural killer T-cells (NKT) — bridge innate and adaptive immunity
Thymic Involution#
Thymic involution begins in childhood, accelerates after puberty, and continues throughout life. The process involves replacement of thymic epithelial tissue with adipose (fat) tissue, reducing the thymus's capacity to produce naive T-cells. Key consequences include:
- Reduced naive T-cell output — fewer new T-cells are produced to respond to novel pathogens
- Skewed T-cell repertoire — the remaining T-cell pool becomes dominated by memory cells specific to previously encountered antigens
- Impaired immune surveillance — reduced ability to detect and eliminate cancer cells
- Weakened vaccine responses — elderly adults generate fewer protective antibodies following vaccination
- Increased autoimmune susceptibility — paradoxically, the decline in thymic function can impair regulatory T-cell production, increasing autoimmune risk
Research on thymic involution has identified hormonal, cytokine-mediated, and transcriptional mechanisms. Sex steroids (particularly testosterone and estrogen) accelerate involution, while transcription factors like FOXN1 are required to maintain thymic epithelial cell identity. The realization that thymic involution is not purely degenerative but involves active regulatory processes has opened the door to interventions — including peptide-based approaches — that may partially reverse or slow the process.
Thymosin Alpha-1: The Clinical Standard#
Evidence Level: Extensive clinical data; approved in 35+ countries Classification: 28-amino acid thymic peptide Research Status: FDA Category 2 (excluded from US compounding); marketed internationally as Zadaxin
Discovery and Development#
Thymosin Alpha-1 (Ta1) was first isolated from thymic tissue by Allan Goldstein's laboratory at the George Washington University in the 1970s. It was identified as the most active component of "thymosin fraction 5," a crude thymic extract that had shown immunomodulatory activity in early studies. The 28-amino acid sequence was characterized, synthesized, and developed into a pharmaceutical product (Zadaxin/thymalfasin) that received regulatory approval in multiple countries beginning in the 1990s.
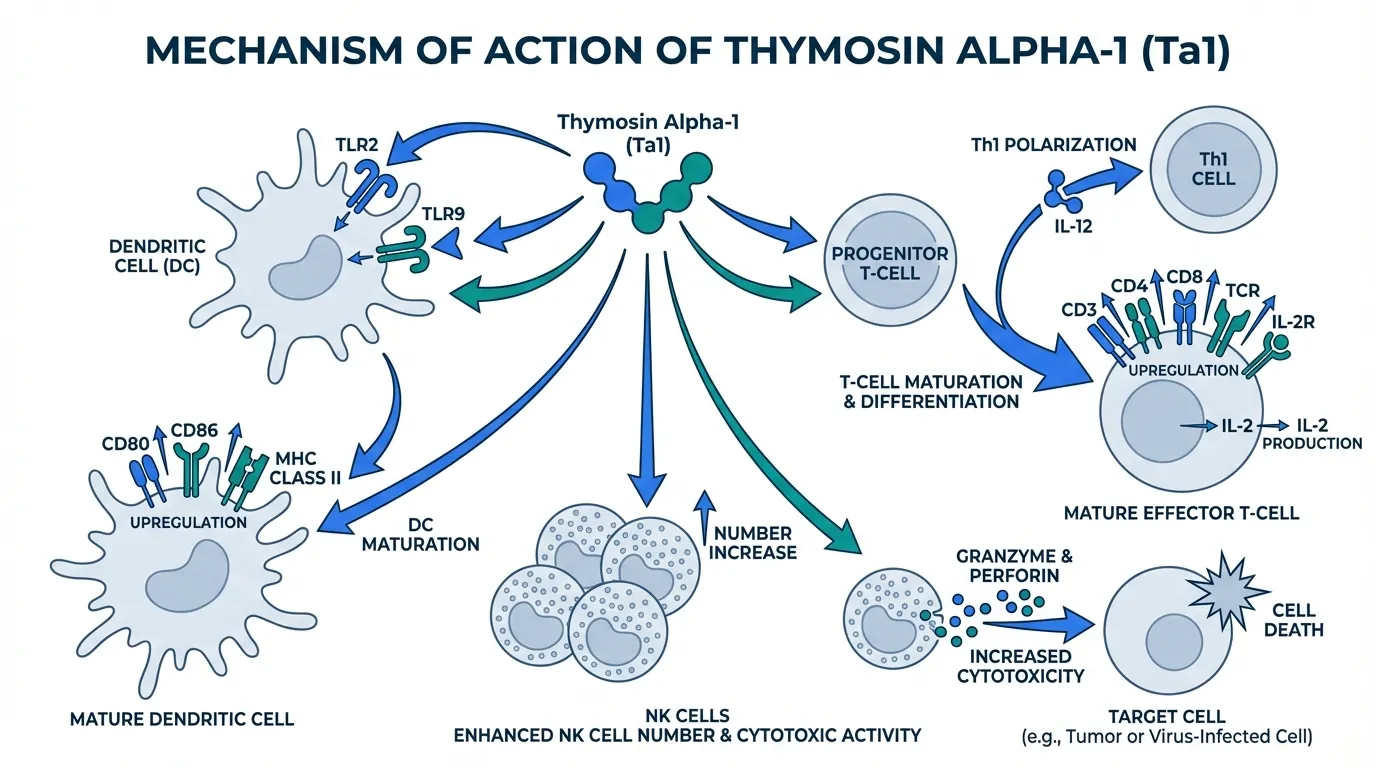
Mechanism of Action#
Ta1 enhances immune function through several interconnected pathways:
Dendritic cell activation: Ta1 activates Toll-like receptors TLR2 and TLR9 on dendritic cells, engaging both MyD88-dependent and TRIF-dependent signaling cascades. This promotes dendritic cell maturation, upregulating co-stimulatory molecules (CD80, CD86, MHC class II) that enhance antigen presentation to T-cells.
T-cell maturation: Ta1 promotes differentiation of immature thymocytes into mature, functional T-cells by upregulating CD3, CD4, CD8, and T-cell receptor expression. It supports IL-2 receptor expression and IL-2 production, critical signals for T-cell proliferation and survival.
Th1 polarization: Through enhanced IL-12 production by activated dendritic cells, Ta1 drives Th1-polarized immune responses. This cellular immunity bias is particularly relevant for viral infections and cancer, where cell-mediated immune responses are protective.
NK cell enhancement: Ta1 increases natural killer cell number and cytotoxic activity, contributing to innate immune surveillance against virus-infected and transformed cells.
Clinical Evidence#
Ta1 has one of the most robust clinical evidence profiles among immunomodulatory peptides:
- Hepatitis B — Phase 3 trials demonstrated enhanced HBV clearance when combined with interferon-alpha. This is the primary approved indication in most countries where Ta1 is marketed.
- Hepatitis C — Clinical evidence supports improved sustained virological response rates as part of combination antiviral therapy.
- Vaccine adjuvant — Studies in elderly and immunocompromised populations demonstrated enhanced vaccine immunogenicity, including improved responses to influenza vaccination.
- Cancer immunotherapy — Investigated as an adjunct to chemotherapy and other cancer treatments, with some evidence for improved immune reconstitution and clinical outcomes.
- Sepsis — Exploratory trials have examined Ta1 for immune restoration in critically ill septic patients with lymphopenia.
- COVID-19 — During the pandemic, Ta1 was studied in several observational studies for immune restoration in severe COVID-19 patients, with reports of improved lymphocyte counts.
A comprehensive 2024 review examining data from more than 30 clinical trials involving over 11,000 human subjects confirmed Ta1's consistent immunomodulatory effects across diverse clinical populations.
Regulatory Status#
Despite extensive international clinical use and a favorable safety record spanning decades, the FDA placed Thymosin Alpha-1 in Category 2 in 2024, classifying it as a biological product excluded from the compounding framework. This decision is being challenged by medical organizations and patient advocacy groups. Outside the United States, Ta1 remains approved and actively used in over 35 countries. For more context on this regulatory situation, see Peptides Under FDA Scrutiny.
Thymalin: The Bioregulator Approach#
Evidence Level: Limited clinical data; primarily Russian/Eastern European research Classification: Thymic extract containing dipeptide bioregulators Research Status: Not FDA-approved; used clinically in Russia
Background#
Thymalin was developed at the St. Petersburg Institute of Bioregulation and Gerontology under the direction of Vladimir Khavinson. Unlike Thymosin Alpha-1, which is a single well-defined peptide, Thymalin was originally derived as a polypeptide complex from bovine thymus tissue. The active components were subsequently identified as short peptides, primarily the dipeptides Glu-Trp (thymogen) and Lys-Glu (Vilon).
The bioregulation theory behind Thymalin proposes that short peptides (2-4 amino acids) can influence gene expression in specific tissues by interacting with DNA and chromatin structures. This framework, developed primarily by Khavinson and colleagues, suggests that thymic peptides regulate the expression of genes involved in immune cell development and thymic function.
Mechanism of Action#
According to the bioregulator model, Thymalin's dipeptide components interact with specific DNA sequences in thymic epithelial cells and immune cells, modulating the expression of genes involved in:
- Thymic epithelial cell maintenance — potentially counteracting age-related loss of thymic tissue
- T-cell differentiation — supporting the maturation of naive T-cells
- Cytokine regulation — modulating the balance of pro-inflammatory and anti-inflammatory signaling
- Immune cell proliferation — enhancing the production of lymphocytes
In vitro studies from the Khavinson group have demonstrated that thymalin and its component peptides can alter gene expression patterns in cultured thymic cells and lymphocytes. However, the proposed direct peptide-DNA interaction mechanism has not been fully characterized at the molecular level and remains controversial in the broader scientific community.
Clinical Research#
Thymalin's clinical evidence comes predominantly from Russian and CIS medical literature:
Long-term observational studies: The most frequently cited evidence involves a study of elderly subjects who received thymalin and epithalamin (a pineal gland peptide) over a multi-year period. The study reported improvements in immune function biomarkers, including increased CD4+ T-cell counts and improved lymphocyte proliferative responses. Mortality rates were also reported to be lower in the treatment group over a 6-year follow-up period.
Immune restoration in elderly patients: Several studies have examined thymalin for restoring immune function in elderly patients with immunodeficiency. Results have generally shown improvements in T-cell subset ratios and immune function laboratory markers.
Combination with epithalamin/epitalon: Some studies have investigated thymalin in combination with Epitalon (the synthetic version of epithalamin), reporting synergistic effects on immune parameters and longevity markers.
Important Limitations#
Thymalin's evidence base carries significant caveats:
- The majority of clinical data comes from a single research group (Khavinson and colleagues)
- Studies generally lack the randomization, blinding, and sample sizes expected by international standards
- Independent replication by Western research groups is largely absent
- The bioregulator peptide framework, while internally consistent, has limited acceptance in mainstream immunology
- The animal-derived original product carries theoretical immunogenicity concerns
Researchers should treat thymalin as an early-stage compound with provocative but unvalidated findings. The gap between its theoretical framework and the confirmatory evidence expected by international regulatory standards remains substantial.
Vilon: The Synthetic Dipeptide Bioregulator#
Evidence Level: Preclinical and limited clinical (Russian studies) Classification: Synthetic dipeptide (Lys-Glu) Research Status: Not FDA-approved; research compound
Background and Mechanism#
Vilon is a synthetic dipeptide (Lys-Glu, also written as KE) identified as one of the active components of the Thymalin complex. It represents the most reductionist approach in the bioregulator peptide field — a two-amino-acid peptide proposed to regulate thymic gene expression.
According to the bioregulator model, Vilon interacts with specific DNA sequences in thymic epithelial cells to modulate the expression of genes involved in immune cell development. In vitro studies have reported that Vilon can:
- Stimulate proliferation of thymic epithelial cells in culture
- Modulate the expression of differentiation markers on T-cell precursors
- Influence cytokine production by immune cells
- Alter gene expression patterns in aging thymic tissue
Research Status#
Vilon's research profile is narrower than Thymalin's. Published studies include:
- Gene expression studies — In vitro experiments demonstrating that the KE dipeptide alters transcription of specific genes in thymic cells and lymphocytes
- Aging studies — Research in aged animals showing partial restoration of thymic morphology and function following Vilon administration
- Immune parameter changes — Clinical observations of improved T-cell subset ratios in elderly subjects receiving Vilon
The same methodological limitations that apply to Thymalin research apply to Vilon studies. The evidence remains preliminary and has not been subjected to rigorous independent validation.
Vilon vs. Thymalin#
Vilon can be understood as the minimal active unit of the thymalin concept. Where Thymalin is a complex mixture of thymic peptides, Vilon is a single defined dipeptide. The advantages of this approach include reproducible synthesis, defined molecular identity, and simplified pharmacology. The disadvantage is that if Thymalin's effects depend on the complex interplay of multiple peptide components, Vilon alone may not replicate the full range of activity.
Comparing Thymic Peptides with Innate Immune Peptides#
While thymic peptides target the adaptive immune system — specifically T-cell development and function — other immune peptides operate through entirely different mechanisms. LL-37, for example, is the only human cathelicidin antimicrobial peptide, functioning as a first-line innate immune defense that directly kills pathogens through membrane disruption.
The distinction is important:
| Feature | Thymic Peptides (Ta1, Thymalin) | LL-37 |
|---|---|---|
| Immune arm | Adaptive (T-cells, DCs) | Innate (antimicrobial) |
| Direct pathogen killing | No | Yes (broad-spectrum) |
| Mechanism | Immune cell modulation | Membrane disruption, signaling |
| Age-related decline | Addresses thymic involution | Not directly age-related |
| Clinical approval | Ta1 approved in 35+ countries | No approvals |
| Best studied for | Viral hepatitis, immunodeficiency | Infections, biofilms, wound healing |
For a detailed comparison between LL-37 and Thymosin Alpha-1, see our LL-37 vs Thymosin Alpha-1 comparison.
Thymic Involution: The Core Problem#
Understanding thymic involution is essential context for evaluating thymic peptides. The process unfolds across the lifespan:
Childhood (birth to puberty): The thymus is at peak size and activity, producing a diverse repertoire of naive T-cells. T-cell receptor diversity is maximal.
Puberty to middle age: Thymic tissue begins to be replaced by adipose tissue. Naive T-cell output declines but remains sufficient to maintain immune competence in most individuals. The rate of involution correlates with sex steroid levels.
Middle age to elderly (50+): Thymic function is substantially reduced. The naive T-cell pool contracts significantly, and the T-cell repertoire becomes increasingly dominated by memory cells. This period correlates with increased susceptibility to new infections, reduced vaccine efficacy, and rising cancer incidence.
Advanced age (75+): Functional thymic tissue may be nearly absent. The immune system relies almost entirely on the existing memory T-cell pool. New pathogen responses are severely impaired.
The clinical consequences of thymic involution are profound. Elderly adults have 10-fold higher mortality from influenza compared to younger adults, respond poorly to novel vaccines, and have increased rates of reactivation of latent infections (such as varicella-zoster virus causing shingles). The COVID-19 pandemic starkly illustrated the consequences of immunosenescence, with dramatically higher mortality in older populations.
Molecular Mechanisms of Involution#
Research has identified several molecular drivers of thymic involution:
- FOXN1 decline — This transcription factor is essential for thymic epithelial cell identity. Its expression decreases with age, leading to loss of thymic epithelial cells and their replacement by adipocytes.
- Sex steroid signaling — Testosterone and estrogen promote thymic involution. Surgical or chemical castration can temporarily reverse thymic atrophy in animal models.
- Inflammatory cytokines — Chronic low-grade inflammation ("inflammaging") contributes to thymic damage through cytokines like IL-6 and TNF-alpha.
- Wnt signaling disruption — Age-related changes in Wnt pathway activity impair thymic epithelial cell renewal.
These molecular insights provide the rationale for peptide-based interventions: if thymic involution is driven by specific molecular changes rather than inevitable tissue death, targeted peptide therapies might modulate these pathways to preserve or restore thymic function.
Practical Research Considerations#
Evidence Hierarchy#
When evaluating thymic peptides, researchers should recognize the substantial differences in evidence quality:
Tier 1 — Thymosin Alpha-1: Extensive clinical trials (11,000+ subjects), international regulatory approval, well-characterized mechanism, defined molecular identity, and decades of post-marketing safety data. This is the only thymic peptide that meets conventional evidence standards for clinical immunomodulation.
Tier 2 — Thymalin: Limited clinical data from primarily one research group, some regulatory approval in Russia, interesting long-term observational data but significant methodological limitations. The evidence is provocative but insufficient for definitive conclusions.
Tier 3 — Vilon: Primarily in vitro and preclinical data with limited human studies. The bioregulator concept is intellectually interesting but lacks rigorous validation by independent groups.
Safety Considerations#
Thymosin Alpha-1 has the most extensive safety data, with decades of clinical use demonstrating mild side effects (primarily injection site reactions) and no significant immunotoxicity. Thymalin and Vilon have more limited safety documentation, and the animal-derived origins of original Thymalin preparations raise theoretical concerns about immunogenicity and batch-to-batch variability.
All thymic peptides carry a theoretical risk of immune overstimulation, particularly in individuals with autoimmune conditions. By enhancing T-cell function, these peptides could potentially exacerbate autoimmune pathology. This concern is more theoretical than evidence-based for Thymosin Alpha-1, which has generally been shown to have immunomodulatory rather than purely immunostimulatory effects, but it warrants consideration.
FDA Regulatory Context#
Thymosin Alpha-1's placement in FDA Category 2 has complicated access in the United States. Researchers and clinicians should be aware that:
- Ta1 cannot be compounded by US pharmacies under the current FDA framework
- International access remains available in countries where Zadaxin is approved
- Regulatory challenges may affect future access to other thymic peptides
- The distinction between thymic peptides as biological products versus synthetic peptides has regulatory implications
Emerging Research Directions#
Several areas of thymic peptide research are actively developing:
Thymic regeneration: Rather than supplementing thymic hormones externally, some research aims to regenerate thymic tissue directly. Growth factors, cytokines, and transcription factor manipulation (particularly FOXN1 upregulation) are being explored alongside peptide approaches.
Combination protocols: The potential for combining thymic peptides with other immunomodulatory approaches — including checkpoint inhibitors in oncology, vaccine adjuvants for elderly populations, and antimicrobial peptides like LL-37 for complex infections — represents an active area of investigation.
Biomarker-guided therapy: Advances in immune monitoring (T-cell receptor sequencing, flow cytometry panels, cytokine profiling) may enable more precise identification of patients who would benefit from thymic peptide therapy and more objective measurement of treatment responses.
Synthetic biology approaches: New peptide design and delivery technologies, including peptide-polymer conjugates and nanoparticle delivery systems, may address pharmacokinetic limitations of current thymic peptides.
Conclusion#
Thymic peptides represent a mechanistically rational approach to one of the most consequential aspects of immune aging. The thymus is not merely a passive organ that degenerates — it is an actively regulated tissue whose decline drives measurable immune dysfunction. Peptides derived from or modeled on thymic tissue aim to restore the specific immune functions lost through involution.
The evidence landscape varies dramatically across compounds. Thymosin Alpha-1 stands apart with clinical validation spanning decades and multiple countries, while Thymalin and Vilon remain early-stage compounds with intriguing but methodologically limited data. Researchers should calibrate their expectations accordingly, recognizing both the therapeutic potential of thymic peptides and the substantial evidence gaps that remain for most compounds in this class.
For comparisons with other immune-modulating peptides, see our guides on top immune-boosting peptides and the LL-37 vs Thymosin Alpha-1 comparison. For general information about peptide mechanisms, visit our What Are Peptides educational page.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- Thymosin Alpha-1 Overview and Research Guide
- Thymosin Alpha-1 Dosing Protocols
- Thymosin Alpha-1 Side Effects and Safety
- Thymalin Overview and Research Guide
- Thymalin Dosing Protocols
- Thymalin Side Effects and Safety
- Vilon Overview and Research Guide
- Vilon Dosing Protocols
- Vilon Side Effects and Safety
- LL-37 Overview and Research Guide
- LL-37 Dosing Protocols
- LL-37 Side Effects and Safety

{kind=link}
Frequently Asked Questions About Thymic Peptides Explained: How Thymosin Alpha-1, Thymalin, and Thymulin Shape Immunity
What does this article cover?
Comprehensive guide to thymic peptides including Thymosin Alpha-1, Thymalin, and Vilon — mechanisms, thymic involution, and immune restoration research. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers Thymosin Alpha-1, Thymalin, Vilon, LL-37. Key context: Thymosin Alpha-1 (Most clinically validated thymic peptide with approval in 35+ countries for hepatitis and immune ...); Thymalin (Thymic extract-derived bioregulator studied for immune restoration and anti-aging applications in...); Vilon (Synthetic dipeptide bioregulator (Lys-Glu) studied for thymic gene expression regulation and immu...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Thymic Peptides Explained: How Thymosin Alpha-1, Thymalin, and Thymulin Shape Immunity." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Most clinically validated thymic peptide with approval in 35+ countries for hepatitis and immune .... Thymic extract-derived bioregulator studied for immune restoration and anti-aging applications in.... Synthetic dipeptide bioregulator (Lys-Glu) studied for thymic gene expression regulation and immu.... These takeaways are based on the research data available at the time of publication.
What is Thymosin Alpha-1 and why is it significant?
Thymosin Alpha-1 is a peptide discussed in this article because: Most clinically validated thymic peptide with approval in 35+ countries for hepatitis and immune modulation. For a complete profile of Thymosin Alpha-1, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Top Immune-Boosting Peptides: Research Overview
Top immune-boosting peptides including Thymosin Alpha-1, Thymalin, LL-37, KPV, and Glutathione — evidence levels and mechanisms reviewed.

Immune-Modulating Peptides: Thymosin Alpha-1, KPV, LL-37, and Beyond
Comprehensive research review of immune-modulating peptides including thymosin alpha-1, KPV, LL-37, thymalin, VIP, and glutathione. Clinical evidence, mechanisms of immune regulation, and implications for autoimmune and inflammatory conditions.

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
You Might Also Like
Related content you may find interesting