LL-37 vs Thymosin Alpha-1: Immune Peptides Compared
LL-37 vs Thymosin Alpha-1 as immune peptides compared — antimicrobial mechanisms, T-cell modulation, and clinical research evidence.
Verdict at a Glance
Thymosin Alpha-1 has a decisive advantage in clinical validation, with regulatory approval in over 35 countries and a well-characterized safety profile from decades of therapeutic use. LL-37 offers a unique mechanism as a direct antimicrobial peptide with broad innate immune effects, but remains in preclinical development. For immune modulation research with clinical translation potential, Thymosin Alpha-1 is the evidence-backed choice. For antimicrobial peptide research and innate immunity studies, LL-37 provides irreplaceable mechanistic value.
| Best for | Pick | Why |
|---|---|---|
| Clinical immune support with regulatory backing | Thymosin Alpha-1 | Approved in 35+ countries with standardized dosing and decades of safety data from clinical use |
| Direct antimicrobial activity research | LL-37 | Only human cathelicidin with direct broad-spectrum antimicrobial, anti-biofilm, and LPS-neutralizing properties |
| Hepatitis B treatment adjunct | Thymosin Alpha-1 | Approved indication with Phase 3 clinical evidence for enhanced viral clearance |
| Wound healing and innate immunity research | LL-37 | Pleiotropic effects on epithelial repair, angiogenesis, and immune cell recruitment through multiple receptor pathways |
| Category | LL-37 | Thymosin Alpha-1 | Advantage |
|---|---|---|---|
| Mechanism of Action | Cationic antimicrobial peptide acting through direct membrane disruption, multiple GPCR/TLR pathways, and immune cell chemotaxis; broad pleiotropic effects on innate immunity and wound healing | Thymic peptide that activates dendritic cells via TLR2/TLR9 signaling, promotes T-cell maturation and differentiation, and modulates cytokine networks toward Th1 responses | Comparable |
| Research Evidence | Extensive basic science literature; preclinical antimicrobial and wound healing data; limited clinical trials; no regulatory approvals | Approved in 35+ countries for hepatitis B; over 4,400 patients in controlled clinical trials; marketed as Zadaxin with decades of clinical use | Thymosin Alpha-1 |
| Side Effect Profile | Limited human safety data; potential for mast cell activation and histamine release at higher concentrations; theoretical autoimmune risk from TLR activation | Well-established safety profile from decades of clinical use; generally well-tolerated with mild injection site reactions; no significant immunotoxicity reported | Thymosin Alpha-1 |
| Dosing Complexity | No standardized human dosing; research protocols vary widely; topical, injectable, and inhalational routes explored in preclinical studies | Standardized dosing of 1.6 mg subcutaneous twice weekly; well-established clinical protocols with clear treatment durations | Thymosin Alpha-1 |
| Antimicrobial Activity | Direct broad-spectrum antimicrobial activity against bacteria, fungi, and enveloped viruses through membrane disruption; anti-biofilm properties; LPS neutralization | No direct antimicrobial activity; enhances host immune responses against pathogens indirectly through T-cell and dendritic cell activation | LL-37 |

Introduction#
LL-37 and Thymosin Alpha-1 are both classified as immune peptides, but they represent fundamentally different approaches to immune modulation. LL-37 is the body's primary antimicrobial peptide, acting as a first-line innate defense that directly kills pathogens and orchestrates inflammatory responses. Thymosin Alpha-1 operates at the adaptive immunity level, enhancing T-cell maturation and dendritic cell function to strengthen the acquired immune response.
This comparison examines how these two immune peptides differ in mechanism, evidence base, and research applications, helping to clarify which addresses specific immunological questions more effectively.
Quick Comparison#
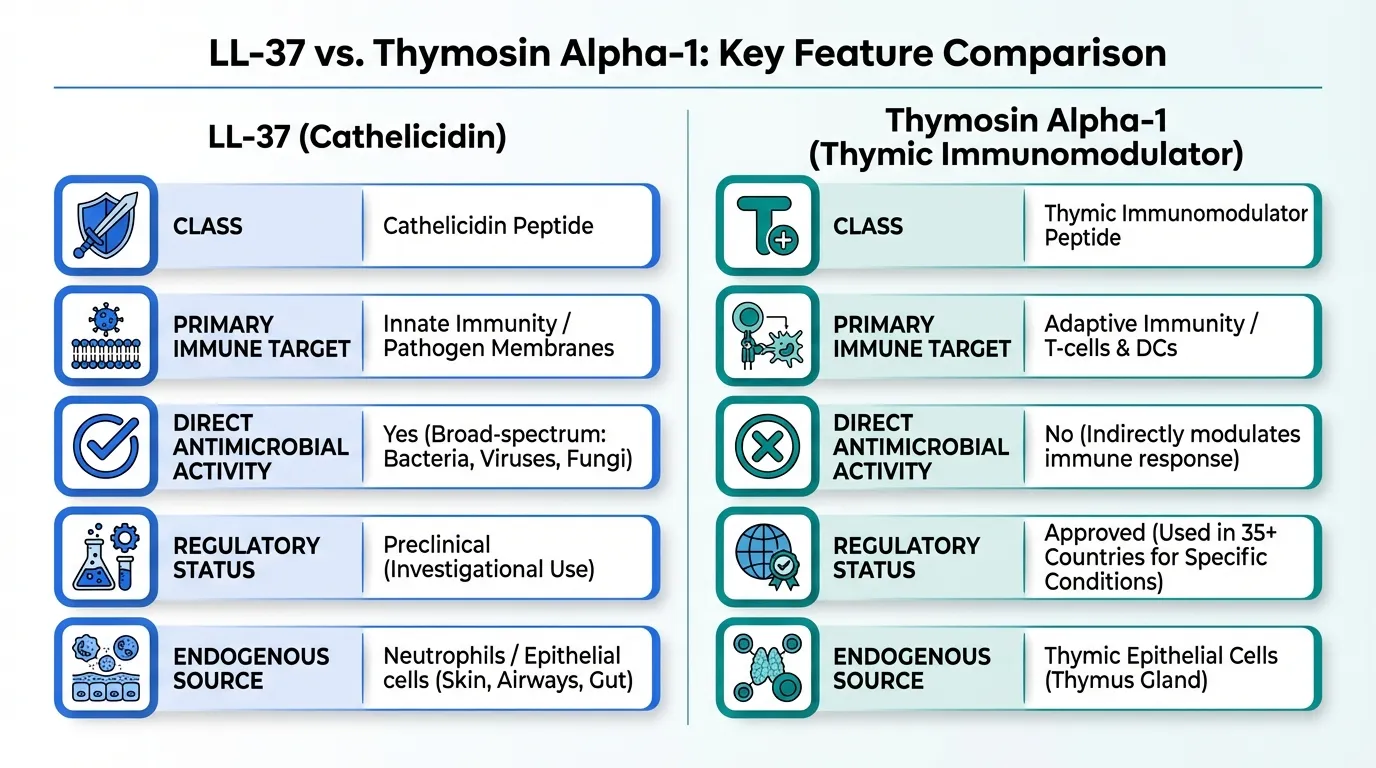
| Feature | LL-37 | Thymosin Alpha-1 |
|---|---|---|
| Structure | 37 amino acids, 4.5 kDa | 28 amino acids, 3.1 kDa |
| Class | Cathelicidin antimicrobial peptide | Thymic immunomodulator |
| Primary Target | Innate immunity, pathogen membranes | Adaptive immunity, T-cells and DCs |
| Direct Antimicrobial | Yes (broad-spectrum) | No |
| Regulatory Status | Preclinical | Approved in 35+ countries |
| Brand Name | None | Zadaxin |
| Key Receptors | FPR2, CXCR2, P2X7, TLRs, EGFR | TLR2, TLR9 |
| Administration | Various research routes | Subcutaneous (1.6 mg 2x/week) |
| Endogenous Source | Neutrophils, epithelial cells | Thymic epithelial cells |
Mechanism of Action Comparison#
LL-37#
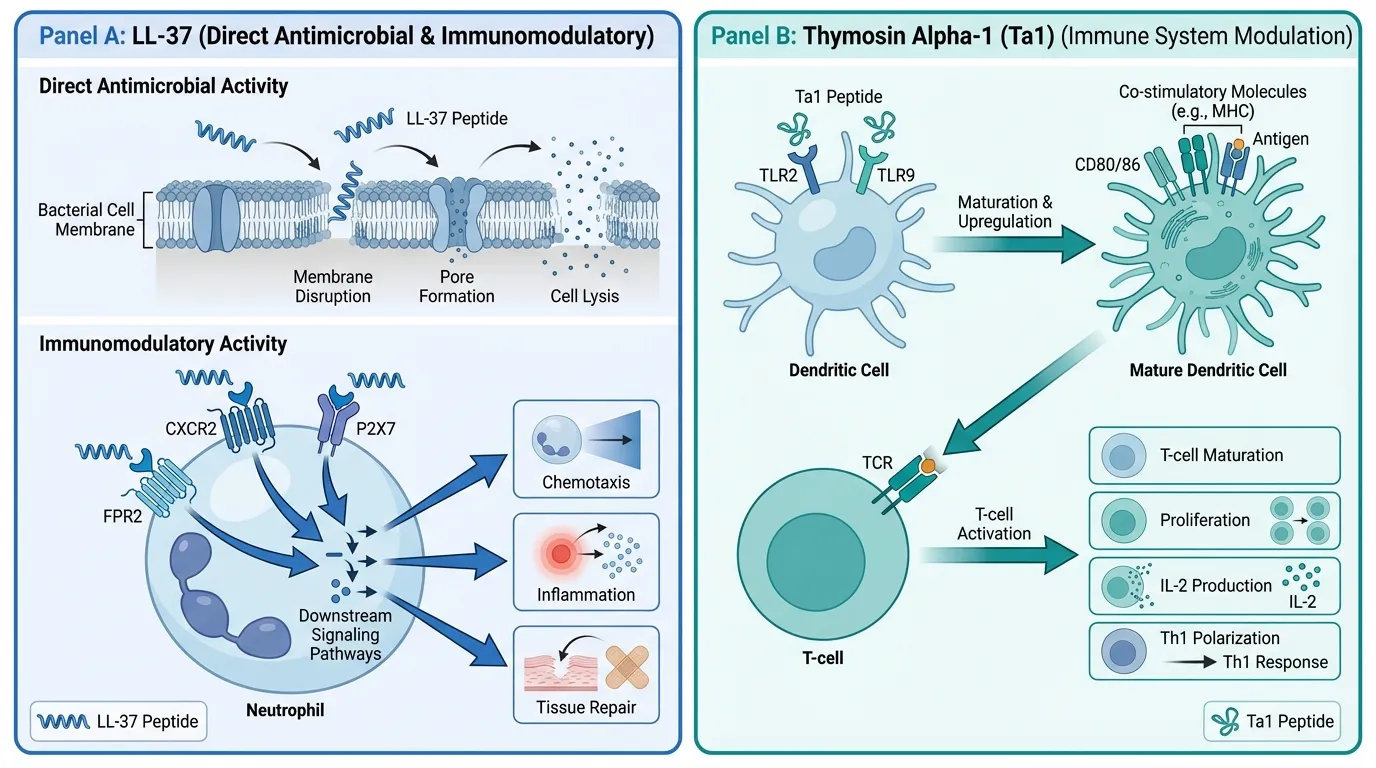
LL-37 is the only human cathelicidin antimicrobial peptide, a 37-amino acid alpha-helical peptide cleaved from the precursor hCAP-18 by proteinase 3. Its mechanism is remarkably pleiotropic, engaging multiple receptors and effector pathways simultaneously.
Direct antimicrobial activity: LL-37 disrupts microbial membranes through electrostatic interactions between its cationic residues and negatively charged bacterial membrane components. This produces rapid bactericidal activity against both gram-positive and gram-negative bacteria, fungi, and enveloped viruses. LL-37 also disrupts bacterial biofilms and neutralizes lipopolysaccharide (LPS) endotoxin.
Receptor-mediated immune signaling: LL-37 activates multiple receptor classes on immune and epithelial cells:
- FPR2/ALX: Drives chemotaxis, respiratory burst, and NET formation in neutrophils and monocytes via Gi-dependent PLC, Ca2+, ERK/p38, and PI3K/AKT signaling
- CXCR2: Mediates neutrophil chemotaxis and angiogenic responses
- MRGPRX2: Activates mast cell degranulation, contributing to inflammation and neurogenic responses
- P2X7: Regulates NLRP3 inflammasome assembly and IL-1 beta maturation
- EGFR transactivation: Through ADAM17-mediated shedding of EGF-family ligands, driving epithelial proliferation and wound repair
- TLR modulation: Neutralizes LPS to dampen TLR4 signaling, but complexes with nucleic acids to enhance TLR7/8/9 responses
This breadth of signaling makes LL-37 a master coordinator of the innate immune response, linking pathogen detection to inflammation, tissue repair, and adaptive immune priming.
Thymosin Alpha-1#
Thymosin Alpha-1 (Ta1) is a 28-amino acid N-terminally acetylated peptide originally isolated from thymic tissue. Its mechanism centers on enhancing adaptive immune function through dendritic cell and T-cell modulation.
TLR-mediated dendritic cell activation: Ta1 activates TLR9 and TLR2 on dendritic cells, engaging MyD88-dependent and TRIF-dependent signaling cascades. This promotes DC maturation with upregulation of co-stimulatory molecules CD80, CD86, and MHC class II, enhancing antigen presentation capacity.
T-cell maturation and function: Ta1 promotes differentiation of immature thymocytes into mature T-cells by upregulating CD3, CD4, CD8, and TCR expression. It enhances IL-2 receptor expression, IL-2 production, and T-cell proliferation in response to antigen stimulation. Ta1 also supports NK cell expansion and cytotoxicity.
Th1 polarization: Through enhanced IL-12 production by activated dendritic cells, Ta1 drives Th1-polarized immune responses. This cellular immunity bias is therapeutically relevant for viral infections and cancer, where Th1 responses are protective.
Unlike LL-37, Ta1 has no direct antimicrobial activity. Its effects are entirely mediated through host immune cell enhancement.
Evidence and Research Comparison#
LL-37 Research#
LL-37 has an extensive basic science literature but limited clinical translation:
- Antimicrobial studies: Demonstrated broad-spectrum activity against MRSA, Pseudomonas aeruginosa, Candida species, and various drug-resistant organisms in vitro
- Wound healing: Preclinical evidence for accelerated wound closure through EGFR transactivation and angiogenesis promotion
- Anti-biofilm: Effective against biofilm-forming bacteria at sub-MIC concentrations in vitro
- Immunology: Core body of literature on innate immune signaling, inflammasome regulation, and immune cell recruitment
- Dermatology: Role in psoriasis pathogenesis through LL-37-DNA complex activation of TLR9 in plasmacytoid dendritic cells
Human clinical trials with exogenous LL-37 are limited. The peptide has been explored in topical wound healing applications and as an anti-infective agent, but no regulatory approvals have been obtained.
Thymosin Alpha-1 Research#
Ta1 has one of the strongest clinical evidence bases among immunomodulatory peptides:
- Hepatitis B: Phase 3 trials demonstrating enhanced HBV clearance when combined with interferon-alpha; approved indication in multiple countries
- Hepatitis C: Clinical evidence for improved sustained virological response as combination therapy
- Vaccine adjuvant: Demonstrated enhancement of vaccine immunogenicity in elderly and immunocompromised populations
- Cancer: Investigated as immunotherapy adjuvant alongside chemotherapy, with some evidence for improved immune reconstitution
- Sepsis: Exploratory trials suggesting potential benefit for immune restoration in critically ill patients
- Clinical experience: Over 4,400 patients studied in controlled trials, with widespread use in approved markets spanning decades
The contrast with LL-37 is stark: Ta1 has completed the full drug development pathway and achieved regulatory approval, while LL-37 remains primarily a research tool.
Side Effects and Safety Comparison#
LL-37 Side Effects#
Limited human safety data are available for exogenous LL-37:
- Mast cell activation: LL-37 activates MRGPRX2 on mast cells, which could cause histamine release, flushing, and allergic-type reactions
- Pro-inflammatory potential: At higher concentrations, LL-37 may exacerbate inflammation rather than resolve it
- Autoimmune risk: The ability of LL-37-nucleic acid complexes to activate TLR7/8/9 has been implicated in psoriasis and lupus pathogenesis
- Dose sensitivity: Effects are highly concentration-dependent, with beneficial and harmful activities occurring at different levels
- Limited data: Without extensive human studies, the full adverse effect profile remains undefined
Thymosin Alpha-1 Side Effects#
Ta1 has a well-established safety profile from decades of clinical use:
- Common: Mild injection site reactions (redness, soreness) occurring in a minority of patients
- Rare: Occasional flu-like symptoms during initial treatment
- Serious: No significant immunotoxicity, autoimmune events, or organ damage reported in clinical trials or post-marketing surveillance
- Immunomodulatory: Tends to normalize rather than overstimulate immune parameters, reducing risk of immune hyperactivation
- Drug interactions: No significant interactions reported; compatible with interferon, antivirals, and chemotherapy
The safety contrast favors Ta1 considerably, though this largely reflects the difference in clinical development stage rather than inherent toxicity differences.
Dosing and Administration Comparison#
LL-37 Dosing#
| Parameter | Details |
|---|---|
| Route | Variable (topical, injectable, inhaled in research) |
| Standardized dosing | None established for humans |
| Research concentrations | 1-100 mcg/mL in various models |
| Topical | Explored for wound applications |
| Systemic | Limited human experience |
| Storage | Sensitive to proteolysis; requires careful handling |
Thymosin Alpha-1 Dosing#
| Parameter | Details |
|---|---|
| Route | Subcutaneous injection |
| Standard dose | 1.6 mg twice weekly |
| Hepatitis B protocol | 1.6 mg SC twice weekly for 6-12 months |
| Vaccine adjuvant | 1.6 mg SC, various schedules studied |
| Administration | Self-injectable prefilled syringes available |
| Storage | Refrigerated; stable formulation |
The difference in dosing maturity is significant. Ta1 has well-established protocols backed by regulatory-grade pharmacokinetic studies, while LL-37 dosing remains empirical and route-dependent.
Use Case Recommendations#
Choose LL-37 When:#
- Direct antimicrobial activity is the primary research objective
- Innate immunity signaling mechanisms are being investigated
- Wound healing biology and epithelial repair pathways are the focus
- Anti-biofilm strategies are under development
- Host defense peptide research requires a human cathelicidin
Choose Thymosin Alpha-1 When:#
- Clinical immune enhancement is the goal with regulatory backing
- T-cell and dendritic cell function need to be augmented
- Viral hepatitis treatment or prevention is the context
- Vaccine immunogenicity needs to be enhanced in vulnerable populations
- Standardized dosing and established safety data are required
Can They Be Combined?#
LL-37 and Thymosin Alpha-1 target complementary arms of the immune system: LL-37 strengthens innate defense and pathogen clearance, while Ta1 enhances the adaptive immune response. Theoretically, combining them could provide layered immune support spanning both innate and adaptive components.
However, no studies have investigated this combination. The primary concern would be potential immune overstimulation, particularly given LL-37's ability to activate inflammasomes and mast cells alongside Ta1's dendritic cell and T-cell enhancement. Any combination research would need careful dose optimization and monitoring of inflammatory markers.
For researchers interested in immune peptide combinations, Thymalin is another thymic peptide that could be considered alongside Ta1, while KPV offers anti-inflammatory modulation that might complement LL-37's pro-inflammatory tendencies.
Verdict#
Thymosin Alpha-1 is the clear winner for anyone seeking an immune peptide with clinical validation. Its approval in 35+ countries, decades of safety data, and standardized dosing protocols make it the most evidence-supported immunomodulatory peptide available. LL-37 occupies a completely different niche as the only human cathelicidin, providing direct antimicrobial activity and innate immune signaling that no other peptide replicates.
These peptides are better understood as complementary rather than competitive. LL-37 addresses the innate, frontline immune response against pathogens, while Thymosin Alpha-1 strengthens the adaptive immune system that provides lasting protection. The appropriate choice depends entirely on which arm of immunity the research or clinical question targets.
For more on immune peptides, see our profiles on KPV and TB-500, or explore the half-life comparison tool to understand peptide pharmacokinetics.
Further Reading#

{kind=link}
{kind=link}
Which Is Better For...
Clinical immune support with regulatory backing
Thymosin Alpha-1
Approved in 35+ countries with standardized dosing and decades of safety data from clinical use
Direct antimicrobial activity research
LL-37
Only human cathelicidin with direct broad-spectrum antimicrobial, anti-biofilm, and LPS-neutralizing properties
Hepatitis B treatment adjunct
Thymosin Alpha-1
Approved indication with Phase 3 clinical evidence for enhanced viral clearance
Wound healing and innate immunity research
LL-37
Pleiotropic effects on epithelial repair, angiogenesis, and immune cell recruitment through multiple receptor pathways
Continue Your Research
Get comparison updates
We publish new head-to-head comparisons regularly. Subscribe to see them first.
Frequently Asked Questions About LL-37 vs Thymosin Alpha-1: Immune Peptides Compared
Which is better, LL-37 or Thymosin Alpha-1?
Thymosin Alpha-1 has a decisive advantage in clinical validation, with regulatory approval in over 35 countries and a well-characterized safety profile from decades of therapeutic use. LL-37 offers a unique mechanism as a direct antimicrobial peptide with broad innate immune effects, but remains in preclinical development. For immune modulation research with clinical translation potential, Thymosin Alpha-1 is the evidence-backed choice. For antimicrobial peptide research and innate immunity s... Individual responses may vary, and this comparison is based on available research data, not a treatment recommendation.
What are the key differences between LL-37 and Thymosin Alpha-1?
The main differences across comparison categories are: Mechanism of Action: advantage goes to neither (tie); Research Evidence: advantage goes to Thymosin Alpha-1; Side Effect Profile: advantage goes to Thymosin Alpha-1. 2 additional categories are analyzed in the full comparison. Each category evaluates a different dimension of the two peptides.
When should I consider Thymosin Alpha-1 over LL-37?
For the scenario of "Clinical immune support with regulatory backing," research data suggests Thymosin Alpha-1 may be more relevant. Approved in 35+ countries with standardized dosing and decades of safety data from clinical use. This is based on currently available evidence and individual circumstances may differ.
How do LL-37 and Thymosin Alpha-1 differ in their mechanisms of action?
LL-37: Cationic antimicrobial peptide acting through direct membrane disruption, multiple GPCR/TLR pathways, and immune cell chemotaxis; broad pleiotropic effects on innate immunity and wound healing. Thymosin Alpha-1: Thymic peptide that activates dendritic cells via TLR2/TLR9 signaling, promotes T-cell maturation and differentiation, and modulates cytokine networks toward Th1 responses.
Which has fewer side effects, LL-37 or Thymosin Alpha-1?
In terms of side effects and tolerability, the advantage goes to Thymosin Alpha-1. LL-37: Limited human safety data; potential for mast cell activation and histamine release at higher concentrations; theoretical autoimmune risk from TLR .... Thymosin Alpha-1: Well-established safety profile from decades of clinical use; generally well-tolerated with mild injection site reactions; no significant immunotox....
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.