Antimicrobial Peptides: LL-37 and KPV in Infection and Inflammation Research

Introduction#
The human body produces its own arsenal of antimicrobial agents — peptides that kill bacteria, neutralize viruses, disrupt fungal membranes, and modulate inflammatory responses. These host defense peptides represent one of the most ancient and conserved arms of the immune system, predating the adaptive immune response by hundreds of millions of years.
Among the most actively researched immune peptides are LL-37 and KPV, which address infection and inflammation through fundamentally different mechanisms. LL-37 is the only human cathelicidin — a direct antimicrobial peptide that physically destroys pathogen membranes while simultaneously orchestrating innate immune responses. KPV is a tripeptide fragment of alpha-melanocyte-stimulating hormone (alpha-MSH) that suppresses inflammation through NF-kappaB inhibition, with particular relevance to gut mucosal immunity.
This review examines the current state of research for both peptides, clarifying their distinct mechanisms, evidence levels, and potential applications in infection and inflammation.
The Innate Immune Defense System#
Before examining individual peptides, it is important to understand the broader context of innate antimicrobial defense.
The innate immune system provides immediate, non-specific protection against pathogens. Unlike the adaptive immune system — which requires days to mount a targeted response through T-cells and antibodies — innate immunity acts within minutes to hours. Antimicrobial peptides are a critical component of this rapid response.
Humans produce several classes of antimicrobial peptides:
- Cathelicidins — LL-37 is the sole human member; produced by neutrophils, macrophages, and epithelial cells
- Defensins — alpha-defensins (produced by neutrophils) and beta-defensins (produced by epithelial cells)
- Histatins — produced in saliva; primarily antifungal
- Dermcidins — produced by eccrine sweat glands
These peptides work synergistically, and their combined activity creates an antimicrobial shield at epithelial surfaces — skin, respiratory tract, gastrointestinal tract, and urogenital tract. When this defense is compromised, susceptibility to infection increases dramatically.
LL-37: The Human Cathelicidin#
Evidence Level: Extensive in vitro and preclinical; limited clinical trials Mechanism: Direct antimicrobial membrane disruption and immune signaling Research Status: Investigational; not FDA-approved
Structure and Production#
LL-37 is a 37-amino-acid cationic peptide with an alpha-helical structure. It is produced as the C-terminal fragment of the 18 kDa precursor protein hCAP-18 (human cationic antimicrobial protein 18), which is cleaved by proteinase 3 to release the active LL-37 peptide.
LL-37 is constitutively expressed in several tissues and cell types:
- Neutrophils — stored in specific granules; released at infection sites
- Macrophages and monocytes — induced by inflammatory signals
- Epithelial cells — expressed in skin, airways, gastrointestinal tract, and urogenital tract
- Mast cells — contribute to LL-37 pools in skin and mucosal tissues
Expression is upregulated by vitamin D signaling (via the vitamin D receptor and vitamin D response elements in the cathelicidin gene), bacterial products, and inflammatory cytokines. The vitamin D connection is significant — it partially explains the association between vitamin D deficiency and increased susceptibility to infections, particularly respiratory and tuberculosis.
Direct Antimicrobial Activity#
LL-37's antimicrobial mechanism involves electrostatic interaction between its cationic residues and the negatively charged components of microbial membranes (lipopolysaccharide in gram-negative bacteria, lipoteichoic acid in gram-positive bacteria). This interaction disrupts membrane integrity, leading to rapid pathogen death.
The spectrum of activity is remarkably broad:
Bacteria: LL-37 kills both gram-positive organisms (including methicillin-resistant Staphylococcus aureus, MRSA) and gram-negative organisms (including Pseudomonas aeruginosa and Escherichia coli). Importantly, bacteria develop resistance to LL-37 far more slowly than to conventional antibiotics, because the peptide targets fundamental membrane structure rather than specific bacterial enzymes.
Fungi: LL-37 has demonstrated activity against Candida species, including drug-resistant strains. The mechanism similarly involves membrane disruption of fungal cell walls.
Viruses: LL-37 disrupts the envelopes of certain viruses, including influenza, HIV, respiratory syncytial virus (RSV), and herpes simplex virus. It also inhibits viral entry into host cells and can neutralize viral particles directly.
Biofilms: One of LL-37's most clinically significant properties is its ability to disrupt bacterial biofilms. Biofilms — structured bacterial communities encased in extracellular matrix — are a major cause of chronic, antibiotic-resistant infections in wounds, prosthetic implants, and chronic respiratory disease. LL-37 disrupts biofilm formation at sub-bactericidal concentrations and can penetrate established biofilms to kill resident bacteria.
Immune Signaling Functions#
Beyond direct pathogen killing, LL-37 serves as a multifunctional immune signaling molecule:
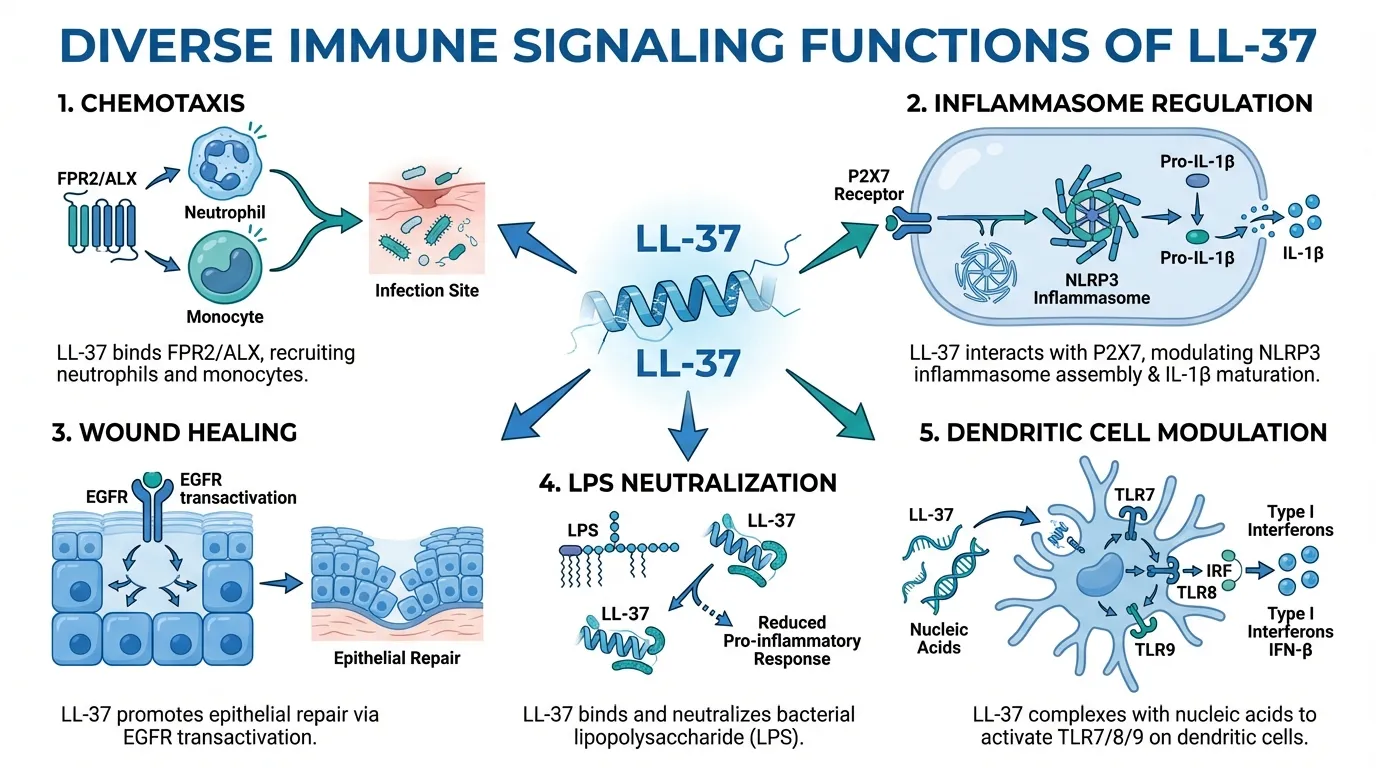
Chemotaxis: LL-37 recruits immune cells to infection sites by activating formyl peptide receptor 2 (FPR2/ALX) on neutrophils, monocytes, and macrophages. This chemotactic activity ensures that additional immune cells are drawn to sites where LL-37 is released during pathogen encounter.
Inflammasome regulation: Through P2X7 receptor interactions, LL-37 regulates NLRP3 inflammasome assembly and IL-1beta maturation, influencing the intensity of inflammatory responses.
Wound healing: LL-37 promotes epithelial repair through EGFR transactivation via ADAM17-mediated shedding of EGF-family ligands. This drives keratinocyte migration and proliferation, accelerating wound closure.
LPS neutralization: LL-37 binds and neutralizes lipopolysaccharide (LPS), the bacterial endotoxin that drives septic shock. This endotoxin-neutralizing capacity has generated interest in LL-37 as a potential anti-sepsis agent.
Dendritic cell modulation: LL-37 complexes with nucleic acids to activate TLR7/8/9 on dendritic cells, bridging innate and adaptive immune responses. However, this same mechanism has been implicated in the pathogenesis of psoriasis, where LL-37-DNA complexes drive aberrant interferon-alpha production.
Research Challenges#
Despite extensive mechanistic data, LL-37's clinical development faces several obstacles:
- Proteolytic degradation — LL-37 is rapidly broken down by proteases in serum and at infection sites, limiting its systemic bioavailability
- Concentration-dependent effects — LL-37 is beneficial at physiological concentrations but can become cytotoxic to host cells at higher levels
- Mast cell activation — Through MRGPRX2 receptor activation, LL-37 can trigger mast cell degranulation and histamine release
- Manufacturing cost — The 37-amino-acid peptide is expensive to synthesize at pharmaceutical scale
- Dual role in disease — LL-37's involvement in psoriasis and potentially other autoimmune conditions complicates its therapeutic profile
Current research is exploring modified LL-37 analogs, delivery systems (nanoparticles, hydrogels, topical formulations), and truncated fragments that retain antimicrobial activity while reducing cytotoxicity.
KPV: Anti-Inflammatory Tripeptide#
Evidence Level: Preclinical only (animal studies and in vitro) Mechanism: NF-kappaB inhibition via alpha-MSH pathway Research Status: No human clinical trials conducted; not FDA-approved
Origin and Structure#
KPV is a tripeptide consisting of three amino acids — lysine, proline, and valine (Lys-Pro-Val) — derived from the C-terminal end of alpha-melanocyte-stimulating hormone (alpha-MSH). Alpha-MSH is a 13-amino-acid neuropeptide with well-characterized anti-inflammatory properties. Research demonstrated that the C-terminal tripeptide KPV retains the anti-inflammatory activity of the full alpha-MSH peptide, and in some experimental systems exceeds it.
This is a significant finding because tripeptides offer practical advantages over larger peptides: they are simple and inexpensive to synthesize, more stable than longer peptides, and — in the case of KPV — may be orally bioavailable.
Mechanism of Action#
KPV's anti-inflammatory mechanism centers on inhibition of the NF-kappaB signaling pathway:
NF-kappaB inhibition: NF-kappaB is a master transcription factor that regulates the expression of hundreds of genes involved in inflammation, immune responses, and cell survival. When activated by inflammatory stimuli (bacterial products, cytokines, oxidative stress), NF-kappaB translocates to the nucleus and drives the expression of pro-inflammatory cytokines, chemokines, adhesion molecules, and enzymes. KPV inhibits this nuclear translocation in a dose-dependent manner, suppressing the downstream inflammatory cascade.
Cytokine suppression: Studies have demonstrated that KPV reduces the production of several key pro-inflammatory mediators:
- IL-8 (CXCL8) — a neutrophil chemokine involved in acute inflammation
- TNF-alpha — a central pro-inflammatory cytokine
- IL-1beta — a key mediator of inflammatory and immune responses
- IL-6 — a cytokine involved in acute phase responses and chronic inflammation
PepT1 transport: One of the most notable findings in KPV research is that the tripeptide is absorbed through the PepT1 transporter in intestinal epithelial cells. PepT1 is a proton-coupled peptide transporter expressed on the apical surface of enterocytes that normally absorbs dietary di- and tripeptides. This provides a mechanism for oral KPV delivery to intestinal immune cells — an unusual property for a bioactive peptide.
Gut Immunity Research#
The most developed area of KPV research concerns its effects on gut inflammation:
DSS-induced colitis model: In the dextran sodium sulfate (DSS) mouse model of inflammatory bowel disease, oral administration of KPV significantly reduced colitis severity. Treated animals showed reduced weight loss, decreased colon shortening, improved histological scores, and lower colonic levels of pro-inflammatory cytokines. The effect was mediated through PepT1-dependent uptake in colonic epithelial cells.
TNBS-induced colitis model: KPV also demonstrated efficacy in the TNBS (2,4,6-trinitrobenzenesulfonic acid) model, which represents a Th1-driven colitis pattern. This suggests that KPV's anti-inflammatory effects are not limited to a single inflammatory pathway.
Intestinal epithelial cell studies: In vitro studies using human intestinal epithelial cell lines (Caco-2, HT-29) confirmed that KPV is transported via PepT1, enters colonocytes, and suppresses NF-kappaB activation and cytokine production in response to inflammatory stimuli.
Important Caveats#
All KPV research is preclinical. No human clinical trials have been conducted, and none are currently registered. Several important caveats apply:
- Mouse colitis models have historically been poor predictors of efficacy in human IBD
- The gap between preclinical promise and clinical translation for IBD therapies is particularly large
- Optimal dosing, long-term safety, and pharmacokinetics in humans are entirely unknown
- Claims about KPV efficacy in humans are speculative until clinical data emerges
KPV remains a compound of preclinical interest, not a validated therapeutic agent.
LL-37 vs. KPV: Different Approaches to Immune Defense#
These two peptides represent fundamentally different strategies:
| Feature | LL-37 | KPV |
|---|---|---|
| Size | 37 amino acids | 3 amino acids (tripeptide) |
| Primary action | Antimicrobial + immune activation | Anti-inflammatory |
| Direct pathogen killing | Yes | No |
| NF-kappaB effect | Complex (context-dependent) | Inhibition |
| Inflammation | Can promote or resolve | Consistently suppresses |
| Clinical trials | Limited, ongoing | None |
| Oral bioavailability | No (proteolytic degradation) | Possible (PepT1 transport) |
| Gut applications | Antimicrobial, biofilm disruption | Anti-inflammatory, colitis models |
| Primary research focus | Infections, wound healing | Inflammatory bowel disease |
LL-37 activates and coordinates immune responses, while KPV suppresses excessive inflammation. In the context of gut immunity, they address different aspects of the problem: LL-37 targets the pathogen, while KPV targets the host inflammatory response.
For a detailed head-to-head analysis, see our KPV vs LL-37 comparison.
The Role of Supporting Immune Molecules#
Glutathione and Oxidative Defense#
Glutathione, the body's primary intracellular antioxidant, plays a supporting role in antimicrobial defense. Immune cells — particularly neutrophils and macrophages — generate large amounts of reactive oxygen species (ROS) during pathogen killing. Glutathione protects these immune cells from oxidative self-damage, maintaining their viability and function during sustained immune responses.
Glutathione depletion has been associated with impaired LL-37 expression and reduced antimicrobial capacity. This connection suggests that antioxidant status may influence the effectiveness of innate antimicrobial defense. For more on glutathione's role in immune function, see the top immune-boosting peptides guide.
Thymosin Alpha-1 and Adaptive Immunity#
While LL-37 and KPV operate in the innate immune space, Thymosin Alpha-1 addresses the adaptive arm through T-cell and dendritic cell modulation. The adaptive immune system provides pathogen-specific, long-lasting immunity — the complement to the rapid but non-specific innate defense provided by antimicrobial peptides.
The relationship between innate and adaptive immunity is bidirectional. LL-37, for example, promotes dendritic cell maturation and T-cell polarization through its signaling functions, demonstrating that antimicrobial peptides influence adaptive immune responses beyond their direct pathogen-killing role. For a detailed comparison, see LL-37 vs Thymosin Alpha-1.
Clinical Translation Challenges#
Both LL-37 and KPV face significant hurdles in clinical development, though the specific challenges differ:
LL-37 Clinical Challenges#
- Stability: Rapid proteolytic degradation limits systemic administration. Research is exploring D-amino acid substitutions, PEGylation, and nanoparticle encapsulation.
- Therapeutic window: The concentration range between antimicrobial efficacy and host cell toxicity is narrow and context-dependent.
- Dual inflammation effects: LL-37 can both promote and resolve inflammation depending on concentration, timing, and tissue context.
- Cost of synthesis: 37-amino-acid peptides require expensive solid-phase synthesis.
- Delivery: Most clinical applications likely require topical or localized rather than systemic delivery.
KPV Clinical Challenges#
- Lack of human data: No clinical trials exist, making any discussion of human efficacy speculative.
- Animal model limitations: Murine IBD models do not faithfully recapitulate human inflammatory bowel disease.
- Mechanism specificity: NF-kappaB inhibition is a broad mechanism with potential for immunosuppression beyond the desired anti-inflammatory effect.
- Dose optimization: Optimal human dosing is entirely unknown.
- Regulatory pathway: Without an IND filing or clinical trial registration, KPV's path to regulatory evaluation remains undefined.
Antibiotic Resistance Context#
LL-37 research is gaining urgency in the context of the global antibiotic resistance crisis. The World Health Organization has identified antimicrobial resistance as one of the top global health threats. Antimicrobial peptides like LL-37 offer potential advantages over conventional antibiotics:
- Multiple killing mechanisms — targeting fundamental membrane structures rather than specific enzymes makes resistance development slower
- Broad spectrum — activity against bacteria, fungi, and viruses with a single agent
- Anti-biofilm activity — addressing a major source of chronic, antibiotic-resistant infections
- Synergy with antibiotics — some studies show that LL-37 enhances the activity of conventional antibiotics, potentially allowing dose reduction
- Immunomodulatory effects — enhancing the host immune response alongside direct killing
However, LL-37 alone is unlikely to replace conventional antibiotics. Its clinical development challenges, concentration-dependent toxicity, and cost of production mean that antimicrobial peptides will likely serve as complements to — not replacements for — traditional antibiotics.
Conclusion#
LL-37 and KPV represent two distinct approaches to immune defense: direct antimicrobial action and anti-inflammatory modulation, respectively. LL-37 has extensive mechanistic data demonstrating broad-spectrum antimicrobial activity, biofilm disruption, and immune signaling — though clinical translation remains challenging. KPV has compelling preclinical data for gut anti-inflammatory effects via NF-kappaB inhibition, but no human data exists.
Researchers evaluating these peptides should maintain clear distinction between in vitro/preclinical findings and clinical evidence. LL-37's antimicrobial properties are well-established in laboratory settings but face significant pharmacokinetic barriers to therapeutic use. KPV's colitis model data is promising but the track record of translating murine IBD results to human outcomes is poor.
Both peptides address real and significant clinical needs — antimicrobial resistance and inflammatory bowel disease — which ensures continued research interest regardless of the current evidence limitations.
For further reading on immune peptides, see our thymic peptides guide, top immune-boosting peptides overview, and the KPV vs LL-37 comparison.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- LL-37 Overview and Research Guide
- LL-37 Dosing Protocols
- LL-37 Side Effects and Safety
- KPV Overview and Research Guide
- KPV Dosing Protocols
- KPV Side Effects and Safety
- Glutathione Overview and Research Guide
- Glutathione Dosing Protocols
- Glutathione Side Effects and Safety
- Thymosin Alpha-1 Overview and Research Guide
- Thymosin Alpha-1 Dosing Protocols
- Thymosin Alpha-1 Side Effects and Safety

{kind=link}
Frequently Asked Questions About Antimicrobial Peptides: LL-37 and KPV in Infection and Inflammation Research
What does this article cover?
LL-37 and KPV antimicrobial peptide research reviewed — mechanisms of action, infection defense, gut immunity, and anti-inflammatory pathways. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers LL-37, KPV, Glutathione, Thymosin Alpha-1. Key context: LL-37 (Human cathelicidin antimicrobial peptide with broad-spectrum activity against bacteria, fungi, vi...); KPV (Anti-inflammatory tripeptide derived from alpha-MSH that inhibits NF-kB signaling and shows gut i...); Glutathione (Endogenous tripeptide antioxidant discussed in context of oxidative stress defense supporting imm...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Human cathelicidin antimicrobial peptide with broad-spectrum activity against bacteria, fungi, vi.... Anti-inflammatory tripeptide derived from alpha-MSH that inhibits NF-kB signaling and shows gut i.... Endogenous tripeptide antioxidant discussed in context of oxidative stress defense supporting imm.... These takeaways are based on the research data available at the time of publication.
What is LL-37 and why is it significant?
LL-37 is a peptide discussed in this article because: Human cathelicidin antimicrobial peptide with broad-spectrum activity against bacteria, fungi, viruses, and biofilms. For a complete profile of LL-37, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Immune-Modulating Peptides: Thymosin Alpha-1, KPV, LL-37, and Beyond
Comprehensive research review of immune-modulating peptides including thymosin alpha-1, KPV, LL-37, thymalin, VIP, and glutathione. Clinical evidence, mechanisms of immune regulation, and implications for autoimmune and inflammatory conditions.

Can Peptides Help with Inflammation? A Research-Based Guide
Anti-inflammatory peptides — KPV, BPC-157, LL-37, thymosin alpha-1, VIP, and glutathione — with mechanisms and clinical evidence.

Top Immune-Boosting Peptides: Research Overview
Top immune-boosting peptides including Thymosin Alpha-1, Thymalin, LL-37, KPV, and Glutathione — evidence levels and mechanisms reviewed.
You Might Also Like
Related content you may find interesting