Weight Loss Peptides for Beginners: Understanding Your Options in 2026

Introduction#
If you have been reading about peptide-based weight loss treatments and feel overwhelmed by the options, you are not alone. The field has expanded rapidly since 2020, moving from a single FDA-approved option to an entire pipeline of increasingly potent medications. Terms like "GLP-1 agonist," "dual agonist," and "triple agonist" are everywhere, but what do they actually mean -- and which options have real evidence behind them?
This guide is designed for people who are new to weight loss peptides. It explains the science in plain language, separates FDA-approved drugs from investigational ones, and helps you understand what the clinical trial data actually shows. Nothing in this article is medical advice -- it is an educational resource to help you have informed conversations with your healthcare provider.
What Are Peptides?#
Peptides are short chains of amino acids -- the same building blocks that make up proteins. Your body naturally produces thousands of peptides that act as signaling molecules, telling cells and organs what to do. Hormones like insulin, glucagon, and GLP-1 are all peptides.
Peptide-based weight loss medications work by mimicking or enhancing these natural signals. Most of the effective weight loss peptides target the incretin system -- a group of gut hormones that regulate appetite, blood sugar, and metabolism after you eat.
The key insight behind modern weight loss peptides is that by activating incretin receptors more strongly or more persistently than natural hormones do, you can produce significant reductions in appetite and body weight.
The Incretin System: Why GLP-1 Dominates#
To understand weight loss peptides, you need to understand two hormones:
GLP-1 (Glucagon-Like Peptide-1): Released by your gut after eating, GLP-1 signals your brain to reduce appetite, slows stomach emptying so you feel full longer, and stimulates insulin release. Natural GLP-1 breaks down in minutes. Weight loss peptides are engineered to last days.
GIP (Glucose-Dependent Insulinotropic Polypeptide): Another gut hormone released after eating. GIP has complex effects on metabolism including insulin secretion, fat storage, and potentially appetite regulation. Its role in weight loss is still being studied, but drugs that target both GIP and GLP-1 receptors produce greater weight loss than GLP-1 alone.
Glucagon: Primarily known for raising blood sugar, glucagon also increases energy expenditure and promotes fat burning in the liver. The newest weight loss peptides add glucagon receptor activation to boost calorie expenditure beyond what appetite reduction alone achieves.
Evidence Tiers: How to Evaluate What You Read#
Not all weight loss peptides have equal evidence. Before diving into specific options, it helps to understand the hierarchy:
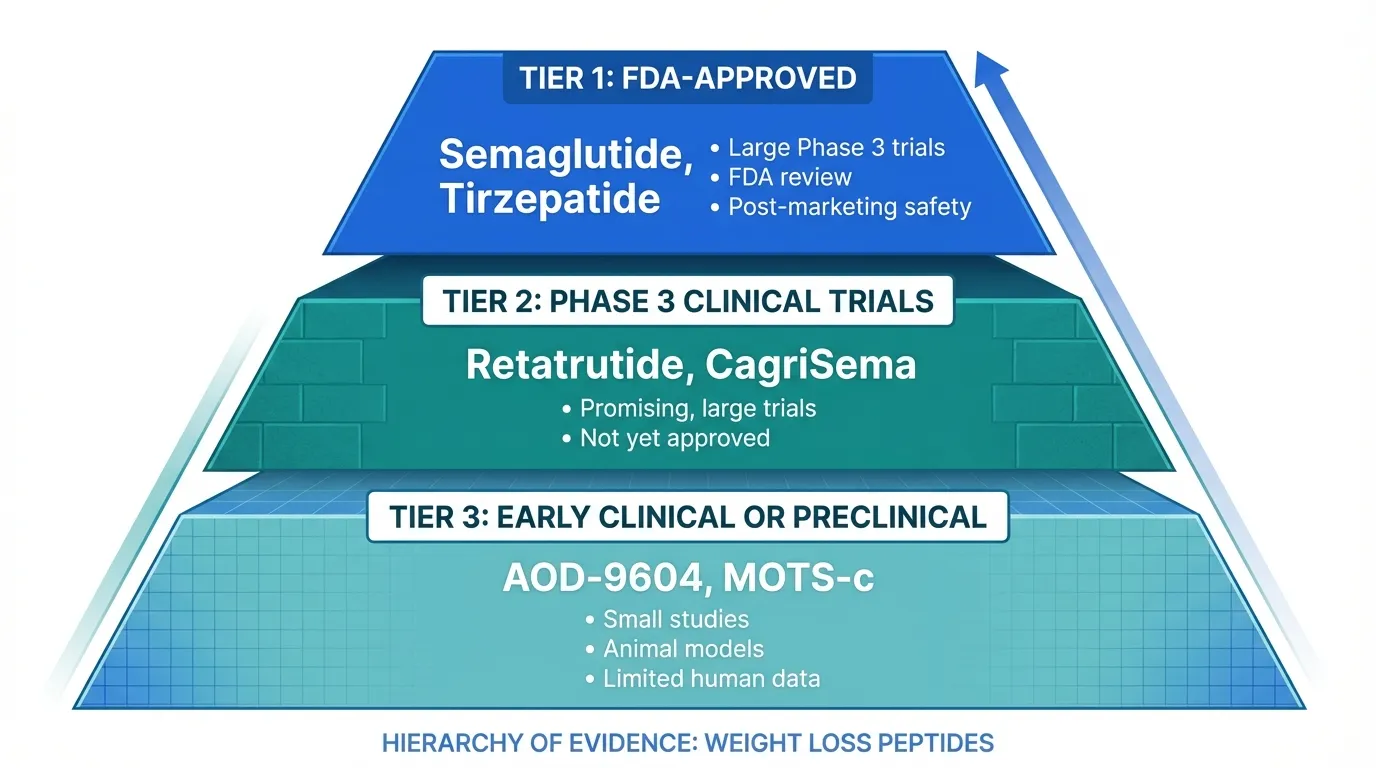
Tier 1 -- FDA-Approved (Strongest Evidence): These have completed large Phase 3 trials with thousands of patients, survived FDA review, and have post-marketing safety surveillance. Currently, this includes Semaglutide (Wegovy) and Tirzepatide (Zepbound).
Tier 2 -- Phase 3 Clinical Trials (Strong Evidence): These have demonstrated efficacy in mid-stage trials and are being tested in large Phase 3 programs. Results are promising but not yet confirmed in the broader populations required for approval. Retatrutide and CagriSema (Cagrilintide + semaglutide) fall here.
Tier 3 -- Early Clinical or Preclinical (Limited Evidence): These have shown signals in small studies, animal models, or early human trials. They are not established treatments. AOD-9604 and MOTS-c are in this category.
When evaluating any weight loss peptide, always ask: How many people were studied? Was it a randomized controlled trial? Has it been replicated? Is it FDA-approved?
FDA-Approved Options#
Semaglutide (Wegovy / Ozempic)#
Semaglutide is the peptide that started the modern weight loss revolution. It is a GLP-1 receptor agonist -- meaning it activates a single receptor type -- and was the first GLP-1 drug approved specifically for chronic weight management.
How it works: Semaglutide mimics GLP-1 but is engineered to resist breakdown, giving it a half-life of about one week. It reduces appetite by acting on brain centers that control hunger and satiety, and it slows gastric emptying.
What the evidence shows: In the landmark STEP 1 trial, participants taking semaglutide 2.4 mg weekly lost an average of 14.9% of their body weight at 68 weeks, compared to 2.4% with placebo. Subsequent STEP trials confirmed these results across different populations, including people with type 2 diabetes.
Side effects: Gastrointestinal issues are the most common: nausea (20-40%), diarrhea (15-35%), and vomiting (10-21%). These typically improve over the first few months, especially with gradual dose escalation over 16-20 weeks.
Bottom line: Semaglutide is the most studied weight loss peptide available. It is widely prescribed, has years of real-world safety data, and is the benchmark against which all newer agents are compared.
Tirzepatide (Zepbound / Mounjaro)#
Tirzepatide is a dual GIP/GLP-1 receptor agonist -- it activates two receptor types simultaneously. This dual mechanism produces greater weight loss than semaglutide.
How it works: Tirzepatide activates both GIP and GLP-1 receptors using a single molecule. The GIP component appears to enhance the metabolic effects beyond what GLP-1 alone achieves, though the exact mechanism of GIP's contribution to weight loss is still being studied.
What the evidence shows: The SURMOUNT-1 trial demonstrated 20.9% mean weight loss at 72 weeks with the 15 mg dose, compared to 3.1% with placebo. Critically, the SURMOUNT-5 trial directly compared tirzepatide to semaglutide: at 72 weeks, tirzepatide produced 20.2% weight loss versus 13.7% for semaglutide -- a statistically significant difference of 6.5 percentage points.
Side effects: Similar to semaglutide but generally comparable or slightly better tolerated. Nausea (12-33%), diarrhea (12-21%), and vomiting (5-13%) are the most common adverse events.
Bottom line: Tirzepatide currently offers the best combination of proven efficacy and regulatory approval. Head-to-head data confirms it produces significantly more weight loss than semaglutide.
Pipeline Drugs: What Is Coming Next#
Retatrutide (Triple Agonist)#
Retatrutide represents the next leap in incretin-based therapy. While tirzepatide targets two receptors, retatrutide targets three: GLP-1, GIP, and glucagon. This is why it is called a "triple agonist."
Why the glucagon receptor matters: Adding glucagon receptor activation brings a new dimension -- increased energy expenditure. While GLP-1 and GIP primarily reduce how much you eat, glucagon boosts how many calories you burn and promotes fat oxidation in the liver. The combination of eating less and burning more may explain retatrutide's exceptional results.
What the evidence shows: The TRIUMPH-4 Phase 3 trial (reported December 2025) showed 28.7% mean weight loss at 68 weeks with the 12 mg dose and 26.4% with the 9 mg dose, compared to 2.1% with placebo. These are the largest weight reductions ever reported in an obesity clinical trial.
Safety considerations: The greater efficacy comes with higher rates of GI side effects. Nausea (38-43%), diarrhea (33-35%), and vomiting (20-21%) are more common than with tirzepatide or semaglutide. The Phase 3 trial also identified a new safety signal: dysesthesia (abnormal sensations of touch) occurred in 8.8% and 20.9% of patients on the 9 mg and 12 mg doses respectively, compared to 0.7% with placebo. These events were generally mild and rarely led to discontinuation, but they are being monitored in ongoing trials.
Current status: Seven additional Phase 3 trials in the TRIUMPH program are expected to complete in 2026. FDA approval could potentially come in 2027 if results remain positive. Retatrutide is NOT currently available as a prescription medication.
CagriSema (Cagrilintide + Semaglutide)#
CagriSema takes a different approach to combination therapy. Instead of building a single molecule that hits multiple receptors, it combines two separate drugs: Cagrilintide (an amylin analog) and Semaglutide (a GLP-1 agonist), co-administered as a single weekly injection.
Why amylin matters: Amylin is a hormone co-secreted with insulin that reduces appetite and slows gastric emptying through different brain pathways than GLP-1. By combining amylin and GLP-1 signaling, CagriSema targets appetite through two complementary mechanisms.
What the evidence shows: The REDEFINE 1 Phase 3 trial (published June 2025 in the New England Journal of Medicine) showed CagriSema produced 20.4% mean weight loss at 68 weeks, compared to 14.9% with semaglutide alone, 11.5% with cagrilintide alone, and 3.0% with placebo. Notably, 60% of CagriSema participants achieved at least 20% weight loss, and 23% lost 30% or more.
Current status: CagriSema is in late-stage development by Novo Nordisk. It is not yet FDA-approved.
Non-GLP-1 Alternatives#
Not all weight loss peptides work through the incretin system. These alternatives operate through entirely different mechanisms, but their evidence base is substantially weaker.
AOD-9604#
AOD-9604 is a modified fragment of human growth hormone (specifically, amino acids 177-191). It was developed to retain the fat-metabolizing properties of growth hormone without its growth-promoting or diabetogenic effects.
What the evidence shows: AOD-9604 showed some promise in early clinical trials for fat loss, but it has never completed the Phase 3 trials required for FDA approval as a weight loss treatment. It is currently approved in some regions as a food supplement ingredient. The evidence base is substantially weaker than for any of the incretin-based drugs discussed above.
Important context: AOD-9604 is widely available from peptide suppliers and is one of the most commonly discussed peptides in online communities. However, the gap between its popularity and its clinical evidence is significant. There are no large randomized controlled trials demonstrating meaningful weight loss.
MOTS-c#
MOTS-c is a mitochondrial-derived peptide -- meaning it is encoded in mitochondrial DNA rather than nuclear DNA. It has been called an "exercise mimetic" because it activates some of the same metabolic pathways as physical exercise.
What the evidence shows: MOTS-c has demonstrated effects on glucose metabolism, insulin sensitivity, and fat oxidation in preclinical studies. A small pilot study in humans showed improvements in insulin sensitivity. However, there are no large clinical trials establishing MOTS-c as a weight loss treatment, and it is years away from the kind of evidence that GLP-1 drugs have accumulated.
Important context: MOTS-c is an interesting research target, but it should not be considered an alternative to evidence-based weight loss treatments. Its potential role may be as a complementary metabolic peptide rather than a primary weight loss agent.
Common Misconceptions#
"Peptides are natural, so they are safer than drugs"#
While many weight loss peptides are based on natural hormones, the therapeutic versions are highly engineered synthetic molecules. Semaglutide, for example, has been chemically modified to last a week in the body instead of the minutes that natural GLP-1 survives. "Natural" does not mean safe, and "synthetic" does not mean dangerous. What matters is clinical evidence.
"You will regain all the weight when you stop"#
Weight regain after stopping GLP-1 medications is real -- the STEP 1 extension study showed participants regained roughly two-thirds of lost weight within a year of stopping semaglutide. However, this is true of almost all obesity treatments, including diet and exercise interventions. Obesity is increasingly understood as a chronic condition requiring ongoing management, not a problem with a one-time fix.
"The newer the peptide, the better it must be"#
Newer does not automatically mean better, especially when newer drugs lack the safety data of established ones. Retatrutide produces more weight loss than semaglutide, but it also has higher rates of side effects, a new dysesthesia signal, and no post-marketing safety data. For many people, a well-characterized drug with a known risk profile may be preferable to a more potent but less-studied one.
"Non-GLP-1 peptides are a good alternative if you want to avoid side effects"#
The GI side effects of GLP-1 drugs are well documented, and it is understandable to want alternatives. However, non-GLP-1 peptides like AOD-9604 and MOTS-c have dramatically less evidence for weight loss. Avoiding a proven treatment in favor of an unproven one is not necessarily a safer choice -- it may simply mean trading known risks for unknown ones and lower efficacy.
How to Compare: A Quick Reference#
| Peptide | Type | Max Weight Loss | Status | Evidence Level |
|---|---|---|---|---|
| Semaglutide | GLP-1 agonist | ~15% (68 wk) | FDA-approved | High |
| Tirzepatide | Dual GIP/GLP-1 | ~21% (72 wk) | FDA-approved | High |
| Retatrutide | Triple GIP/GLP-1/Glucagon | ~29% (68 wk) | Phase 3 | Moderate |
| CagriSema | GLP-1 + Amylin | ~20% (68 wk) | Phase 3 | Moderate |
| AOD-9604 | GH fragment | Unestablished | Not approved | Low |
| MOTS-c | Mitochondrial peptide | Unestablished | Preclinical | Very low |
What to Discuss With Your Doctor#
If you are considering a weight loss peptide, here are evidence-based questions to bring to your healthcare provider:
-
Am I a candidate? FDA-approved weight loss medications are typically indicated for adults with a BMI of 30 or greater, or 27 or greater with at least one weight-related condition.
-
Which medication fits my profile? Tirzepatide produces more weight loss than semaglutide in clinical trials, but availability, insurance coverage, cost, and your specific medical history all factor into the decision.
-
What about side effects? Understanding the GI side effect profile and the dose escalation schedule is important for setting realistic expectations. Most side effects improve with time and proper titration.
-
How long will I need to take it? Current evidence suggests long-term use is needed to maintain weight loss. Discuss the plan for ongoing treatment with your provider.
-
What about muscle loss? Significant weight loss from any cause results in some lean mass loss. Ask about protein intake targets and resistance training to preserve muscle. This is an active area of research -- see our article on preserving muscle mass on GLP-1 medications.
The Bigger Picture#
The weight loss peptide field is in a period of rapid advancement. In just a few years, we have gone from ~15% weight loss with semaglutide to ~29% with retatrutide, and combination approaches like CagriSema and bimagrumab + semaglutide are addressing the muscle loss concern.
For beginners, the most important takeaway is this: focus on evidence. The FDA-approved options -- Semaglutide and Tirzepatide -- have the strongest data and the most understood risk profiles. Pipeline drugs like Retatrutide and CagriSema show extraordinary promise but are not yet available as approved treatments. And non-GLP-1 peptides, while interesting from a research perspective, do not yet have the evidence to be considered reliable weight loss options.
This field will continue to evolve. Staying informed, being skeptical of hype, and working with qualified healthcare providers are the best strategies for navigating it.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- AOD-9604 Overview and Research Guide
- AOD-9604 Dosing Protocols
- AOD-9604 Side Effects and Safety
- Cagrilintide Overview and Research Guide
- Cagrilintide Dosing Protocols
- Cagrilintide Side Effects and Safety
- MOTS-c Overview and Research Guide
- MOTS-c Dosing Protocols
- MOTS-c Side Effects and Safety
- Retatrutide Overview and Research Guide
- Retatrutide Dosing Protocols
- Retatrutide Side Effects and Safety
- Semaglutide Overview and Research Guide
- Semaglutide Dosing Protocols
- Semaglutide Side Effects and Safety
- Tirzepatide Overview and Research Guide
- Tirzepatide Dosing Protocols
- Tirzepatide Side Effects and Safety

{kind=link}
Frequently Asked Questions About Weight Loss Peptides for Beginners: Understanding Your Options in 2026
What does this article cover?
A beginner-friendly guide to weight loss peptides in 2026, covering GLP-1 agonists, dual and triple agonists, non-GLP-1 alternatives, and how to evaluate the evidence behind each option. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers AOD-9604, Cagrilintide, MOTS-c, Retatrutide, Semaglutide, Tirzepatide. Key context: AOD-9604 (Non-GLP-1 peptide fragment of growth hormone studied for fat metabolism); Cagrilintide (Amylin analog combined with semaglutide in CagriSema for enhanced weight loss); MOTS-c (Mitochondrial-derived peptide investigated for metabolic regulation and exercise mimicry). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Weight Loss Peptides for Beginners: Understanding Your Options in 2026." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Non-GLP-1 peptide fragment of growth hormone studied for fat metabolism. Amylin analog combined with semaglutide in CagriSema for enhanced weight loss. Mitochondrial-derived peptide investigated for metabolic regulation and exercise mimicry. These takeaways are based on the research data available at the time of publication.
What is AOD-9604 and why is it significant?
AOD-9604 is a peptide discussed in this article because: Non-GLP-1 peptide fragment of growth hormone studied for fat metabolism. For a complete profile of AOD-9604, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading
Weight Loss Peptides: Mechanisms, Evidence, and How They Compare
A mechanism-focused guide to weight loss peptides — how GLP-1, GIP, and glucagon pathways drive fat loss, how single, dual, and triple agonists compare, and what the clinical evidence actually shows.
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.

AOD-9604 + Tesamorelin + MOTS-C Stack: Fat Loss and Metabolic Peptide Research
An evidence-based review of the AOD-9604, tesamorelin, and MOTS-C peptide stack for body composition and metabolic health, examining clinical evidence for each component, the rationale for combining them, and critical gaps.
You Might Also Like
Related content you may find interesting