Peptides for Wound Healing: BPC-157, GHK-Cu, TB-500, and the Science of Tissue Repair

Introduction#
Wound healing is a coordinated biological process involving hemostasis, inflammation, proliferation, and remodeling. When any phase stalls or becomes dysregulated, wounds become chronic -- a problem that affects an estimated 8.2 million Medicare beneficiaries in the United States alone, with annual costs exceeding $28 billion 1.
Peptides have emerged as a focus of regenerative research because they can target specific phases of the healing cascade with relatively high selectivity and low toxicity. Unlike small-molecule drugs that often have broad receptor profiles, peptides interact with defined molecular pathways -- promoting angiogenesis, modulating inflammation, stimulating cell migration, or restructuring the extracellular matrix.
This guide examines the five most studied wound healing peptides: BPC-157, GHK-Cu, TB-500, KPV, and VIP. For each, we present the mechanism of action, research evidence, wound type specificity, and critical limitations. The goal is to provide researchers with an honest assessment of the evidence landscape, distinguishing between robust clinical data and preliminary preclinical signals.
Regulatory Note: BPC-157 and GHK-Cu were placed in FDA Category 2 (restricted from compounding) in 2024. None of the peptides in this article are FDA-approved for wound healing indications. TB-500 and BPC-157 are prohibited by WADA.
The Wound Healing Cascade and Peptide Targets#
Before examining individual peptides, it is worth understanding where each intervenes in the wound healing process.
Phase 1: Hemostasis and Inflammation (Hours to Days)#
The immediate response to tissue injury involves platelet aggregation, clot formation, and recruitment of neutrophils and macrophages. Excessive or prolonged inflammation is a primary driver of chronic wounds. KPV and VIP target this phase through NF-kB inhibition and cytokine modulation, respectively.
Phase 2: Proliferation (Days to Weeks)#
New tissue formation depends on fibroblast proliferation, collagen deposition, angiogenesis, and epithelialization. BPC-157 acts here through VEGF-mediated angiogenesis and FAK-paxillin-driven cell migration. TB-500 promotes this phase through actin-mediated cell migration and endothelial tube formation. GHK-Cu stimulates fibroblast activity and collagen synthesis.
Phase 3: Remodeling (Weeks to Months)#
Immature type III collagen is gradually replaced by stronger type I collagen, and the wound contracts. GHK-Cu has the strongest profile for this phase, modulating genes involved in extracellular matrix organization, decorin production, and controlled remodeling. TB-500 contributes through its anti-fibrotic properties, reducing excessive scar formation.
BPC-157: Angiogenesis and Cytoprotection#
BPC-157 (Body Protection Compound-157) is a 15-amino-acid peptide derived from a protein found in human gastric juice. It has been studied in over 100 animal studies spanning virtually every tissue type relevant to wound healing.
Mechanism of Action#
BPC-157's wound healing effects center on three interconnected pathways:
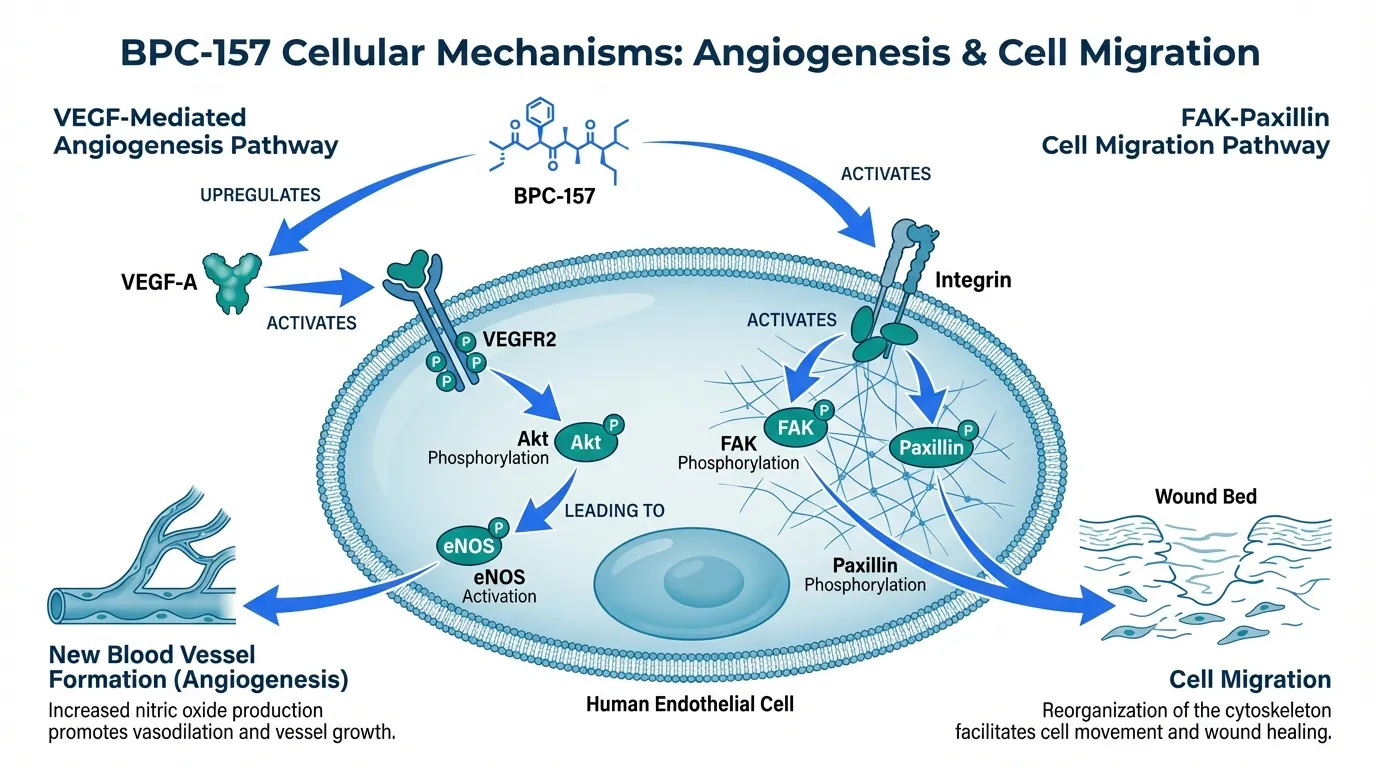
VEGF-Mediated Angiogenesis: BPC-157 upregulates VEGF-A expression and activates VEGFR2, leading to downstream Akt phosphorylation and eNOS activation. This VEGFR2-Akt-eNOS signaling axis promotes new blood vessel formation, which is essential for delivering oxygen and nutrients to healing tissue. In a rat cutaneous wound model, BPC-157 increased VEGF-A expression by approximately 140% compared to controls, with significantly increased capillary density at the wound site 2.
Nitric Oxide System Modulation: Uniquely among healing peptides, BPC-157 demonstrates bidirectional NO modulation -- it counteracts both NO deficiency (L-NAME-induced) and NO excess (L-arginine-induced). This adaptability may explain its broad tissue applicability, as different wound environments have different NO status 3.
FAK-Paxillin Cell Migration: BPC-157 activates focal adhesion kinase (FAK) and paxillin phosphorylation in fibroblasts and tendon cells, promoting cell migration into the wound bed. This pathway is particularly relevant for tendon and ligament repair, where fibroblast migration is the rate-limiting step 4.
Research Evidence by Wound Type#
Skin Wounds: In a rat cutaneous wound model, BPC-157 accelerated wound closure to 77-82% by day 18 compared to 60% in controls, with enhanced collagen deposition and neovascularization 2. Similar results have been reported across multiple skin wound studies using topical, subcutaneous, and systemic administration routes.
Tendon and Ligament Injuries: A systematic review identified consistent improvements in biomechanical properties after BPC-157 treatment in rat Achilles tendon transection, medial collateral ligament (MCL) transection, and rotator cuff models. Maximum force and stiffness measures improved toward normal values in treated animals 5. A 2025 systematic review of 36 studies (35 preclinical, 1 clinical) confirmed BPC-157's role in musculoskeletal healing via growth factor upregulation 6.
Gastrointestinal Wounds: Given its gastric origin, BPC-157 has a particularly strong profile for GI healing. Preclinical data includes fistula closure, anastomotic leak prevention, and mucosal healing in colitis models. A 53-patient enema trial for ulcerative colitis showed tolerability comparable to placebo, though efficacy data from this trial remains limited 7.
Burns: In rat burn wound models, BPC-157 improved re-epithelialization rate and collagen organization compared to controls, though the evidence base for burn wounds is smaller than for other wound types.
Limitations#
The vast majority of BPC-157 evidence comes from animal studies, with total human exposure across all published studies under 100 patients. Most preclinical work originates from a small number of research groups, raising questions about independent replication. A registered Phase I trial (NCT02637284) has unclear completion status. BPC-157 was placed in FDA Category 2 in 2024, restricting its availability from compounding pharmacies.
GHK-Cu: Gene Expression and Tissue Remodeling#
GHK-Cu (glycyl-L-histidyl-L-lysine copper complex) is a naturally occurring tripeptide-copper complex found in human plasma at approximately 200 ng/mL in young adults, declining to approximately 80 ng/mL by age 60. This age-related decline has prompted significant research into its role in tissue repair and regeneration.
Mechanism of Action#
GHK-Cu's wound healing effects operate at the gene expression level, making it mechanistically distinct from other healing peptides.
Broad Gene Modulation: A landmark 2014 Connectivity Map analysis demonstrated that GHK modulates 4,000+ human genes, with significant upregulation of genes involved in collagen synthesis, glycosaminoglycan production, and extracellular matrix organization, and downregulation of genes associated with inflammation and tissue destruction 8.
Collagen Remodeling: GHK-Cu stimulates synthesis of both type I and type III collagen, as well as decorin -- a proteoglycan that regulates collagen fibril assembly and spacing. This dual effect on collagen production and organization is important because scar tissue is characterized by disorganized collagen, while normal tissue has a structured collagen architecture 9.
Copper Delivery: The copper ion in GHK-Cu is not merely structural. Copper is a required cofactor for lysyl oxidase (which cross-links collagen and elastin), superoxide dismutase (which scavenges free radicals), and several other enzymes critical to wound healing. GHK acts as a copper delivery vehicle, concentrating copper at sites where it is needed 10.
Anti-Inflammatory Effects: GHK-Cu suppresses TGF-beta signaling and reduces levels of pro-inflammatory cytokines including TNF-alpha, IL-6, and reactive carbonyl species. This anti-inflammatory action is particularly relevant in chronic wounds where persistent inflammation prevents progression to the proliferative phase 8.
Research Evidence by Wound Type#
Skin Wounds and Cosmetic Applications: GHK-Cu is the most commercially developed peptide on this list, with extensive use in topical cosmeceutical formulations. Clinical studies of topical GHK-Cu creams have demonstrated increased skin thickness, improved elasticity, and enhanced collagen density in aged skin 9. In wound healing contexts, topical GHK-Cu improved re-epithelialization and reduced inflammation in controlled animal studies.
Surgical Wounds: In a controlled study using standardized surgical wounds, GHK-Cu-treated wounds showed significantly enhanced collagen deposition and organized extracellular matrix compared to untreated controls. The remodeling phase was notably accelerated, with earlier transition from type III to type I collagen.
Chronic and Diabetic Wounds: GHK-Cu's combination of pro-angiogenic, anti-inflammatory, and ECM-remodeling properties makes it theoretically well-suited for chronic wounds. However, direct clinical trial data in diabetic wound models is limited. The gene expression data suggests modulation of pathways disrupted in diabetic wound healing, but this has not been validated in controlled human studies.
Limitations#
Despite extensive molecular and gene expression data, GHK-Cu's clinical evidence base consists primarily of topical cosmetic applications rather than controlled wound healing trials. The gap between in vitro gene expression changes and in vivo clinical wound healing outcomes remains significant. Injectable GHK-Cu is not FDA-approved, and the peptide was placed in FDA Category 2 in 2024. The concentration of GHK-Cu that reaches wound beds after topical application versus the concentrations used in gene expression studies may differ substantially.
TB-500: Cell Migration and Anti-Fibrotic Repair#
TB-500 is a synthetic version of thymosin beta-4, a 43-amino-acid peptide that functions as the principal actin-sequestering protein in mammalian cells. TB-500 contains the full thymosin beta-4 sequence and retains its biological activity, including the critical LKKTET actin-binding motif.
Mechanism of Action#
Actin-Mediated Cell Migration: Approximately 50% of cellular actin exists as monomeric G-actin bound to thymosin beta-4 in a 1:1 stoichiometric complex. When cells receive wound-related migration signals, G-actin is released from this complex, enabling rapid actin polymerization at the leading edge of migrating cells. This controlled actin release is the primary mechanism by which TB-500 accelerates wound closure 11.
Anti-Fibrotic Properties: TB-500 reduces myofibroblast differentiation in healing tissues, resulting in decreased scar formation. Its N-terminal metabolite Ac-SDKP has independent anti-fibrotic activity and is normally degraded by angiotensin-converting enzyme (ACE). This creates a pharmacologically relevant interaction: ACE inhibitors can elevate Ac-SDKP levels and potentially enhance TB-500's anti-scarring effects 12.
ILK-Akt Survival Signaling: TB-500 activates integrin-linked kinase (ILK), which phosphorylates Akt and promotes cell survival under ischemic conditions. This mechanism, demonstrated in the landmark 2004 Nature study by Bock-Marquette and colleagues, is particularly relevant for wounds in poorly perfused tissue 13.
Research Evidence by Wound Type#
Chronic Dermal Wounds: TB-500 has the strongest clinical evidence among healing peptides for dermal wound applications. A Phase II trial demonstrated that thymosin beta-4 accelerated healing of venous stasis ulcers and pressure ulcers by approximately one month compared to placebo in responders 14. The foundational 1999 Malinda study showed a 42% increase in re-epithelialization at day 4 and 61% at day 7 in a rat wound model 11.
Corneal Wounds: The RGN-259 formulation (0.1% thymosin beta-4 eye drops) advanced through Phase III clinical trials for neurotrophic keratopathy, demonstrating a 35.1% reduction in ocular discomfort and 59.1% reduction in corneal staining versus placebo. This represents the most advanced clinical development for any healing peptide on this list 15.
Cardiac Tissue: Thymosin beta-4 was the first molecule shown to promote simultaneous cardiomyocyte survival and vascular regeneration in a mouse myocardial infarction model. However, translation to large animals has been inconsistent -- a pig model failed to replicate the rodent findings 16.
Burns: Preclinical burn wound studies show accelerated re-epithelialization and reduced scar formation with TB-500 treatment, consistent with its dual cell migration and anti-fibrotic mechanisms.
Limitations#
While TB-500 has more clinical trial data than most healing peptides, the Phase III results were specifically for ophthalmic (corneal) indications using a topical formulation. The Phase II dermal wound data, while promising, was in a relatively small study. Long-term human safety data extends only to 14 days of IV dosing. Translation from rodent cardiac models to large animal models was unsuccessful, raising questions about species-specific effects. TB-500 is not FDA-approved for any indication and is prohibited by WADA.
KPV: Anti-Inflammatory Wound Modulation#
KPV (Lys-Pro-Val) is a tripeptide derived from the C-terminal end of alpha-melanocyte-stimulating hormone (alpha-MSH). Unlike the other peptides in this guide that primarily target the proliferative phase of healing, KPV targets the inflammatory phase -- making it particularly relevant for wounds stalled in chronic inflammation.
Mechanism of Action#
NF-kB Inhibition: KPV inhibits nuclear factor kappa-B (NF-kB) activation in a dose-dependent manner. NF-kB is the master transcription factor for inflammatory cytokine production, and its persistent activation is a hallmark of chronic non-healing wounds. By suppressing NF-kB, KPV reduces production of TNF-alpha, IL-1beta, IL-6, and IL-8 17.
PepT1-Mediated Uptake: Unusually for a peptide, KPV is absorbed via the PepT1 transporter in intestinal epithelial cells and immune cells. This receptor-mediated uptake allows oral bioavailability -- a significant advantage over peptides that require injection. PepT1-mediated uptake also concentrates KPV in inflamed intestinal tissue, where PepT1 expression is upregulated 18.
Superior Anti-Inflammatory Potency: Comparative studies have shown that KPV exerts a stronger anti-inflammatory effect than the full-length alpha-MSH peptide from which it is derived. This is attributed to its small size allowing efficient cellular uptake and its retained ability to interact with the same downstream signaling pathways 19.
Research Evidence#
Inflammatory Bowel Disease Models: The primary evidence for KPV comes from murine colitis models. KPV reduced disease severity in both DSS-induced and TNBS-induced colitis when administered orally, with decreased mucosal inflammation, reduced weight loss, and improved histological scores 20. These models are relevant to wound healing because intestinal inflammation involves the same inflammatory cascades present in chronic dermal wounds.
Inflammatory Wound Environments: While direct dermal wound healing studies with KPV are limited, its mechanism of action -- NF-kB suppression and cytokine reduction -- addresses the primary barrier to healing in chronic wounds: persistent inflammation. In vitro studies confirm that KPV reduces inflammatory mediator production in macrophages and epithelial cells at wound-relevant concentrations.
Limitations#
All KPV research is preclinical. No human clinical trials have been conducted for any indication. The evidence base is significantly smaller than for BPC-157 or TB-500. Direct evidence for dermal wound healing is limited; most data comes from gut inflammation models. While the mechanistic rationale for wound healing is sound, translation from IBD models to chronic wound applications has not been validated.
VIP: Immunomodulation in Complex Wound Environments#
VIP (Vasoactive Intestinal Peptide) is a 28-amino-acid neuropeptide with broad immunomodulatory and anti-inflammatory properties. Originally characterized for its effects on intestinal smooth muscle and secretion, VIP has been studied for its role in modulating immune responses in wound environments.
Mechanism of Action#
Broad Immunomodulation: VIP acts through VPAC1 and VPAC2 receptors, which are expressed on macrophages, dendritic cells, T cells, and epithelial cells. Receptor activation triggers cAMP-dependent signaling cascades that shift the immune response from pro-inflammatory (M1 macrophage, Th1/Th17) toward anti-inflammatory and reparative (M2 macrophage, Treg) phenotypes 21.
Cytokine Regulation: VIP suppresses production of pro-inflammatory cytokines (TNF-alpha, IL-6, IL-12) while promoting anti-inflammatory mediators (IL-10, TGF-beta). This balanced immunomodulation is distinct from simple immunosuppression -- VIP does not abolish immune function but redirects it toward tissue repair 22.
Vascular Effects: As its name suggests, VIP promotes vasodilation and increases blood flow to wound sites. It also supports endothelial barrier integrity and reduces vascular permeability, which can help resolve wound edema.
Research Evidence#
Autoimmune and Inflammatory Models: VIP has demonstrated efficacy in multiple preclinical models of inflammatory disease, including experimental autoimmune encephalomyelitis, rheumatoid arthritis, and sepsis models. In each case, VIP reduced inflammatory tissue damage and promoted tissue preservation 22.
Wound-Adjacent Applications: VIP has been studied for respiratory epithelial protection, intestinal mucosal defense, and skin barrier maintenance. In a model of radiation-induced tissue injury, VIP improved mucosal healing and reduced inflammatory infiltration. These wound-adjacent findings suggest potential for direct wound healing applications.
Chronic Inflammatory Wounds: The theoretical case for VIP in chronic wounds rests on its ability to resolve the persistent inflammatory state that prevents wound progression. Chronic wounds -- diabetic ulcers, venous stasis ulcers, pressure injuries -- are characterized by a pro-inflammatory microenvironment with elevated M1 macrophages, excess proteases, and reduced growth factor availability. VIP's ability to shift macrophage polarization from M1 to M2 directly addresses this pathology.
Limitations#
VIP has not been studied specifically in wound healing clinical trials. Its evidence base for wound applications is inferred from its immunomodulatory mechanism and results in adjacent inflammatory models. VIP is a 28-amino-acid peptide with a very short half-life (approximately 1-2 minutes in circulation), which presents significant delivery challenges. The peptide's broad receptor distribution means systemic administration could produce vasodilatory side effects. VIP research for wound healing remains largely theoretical compared to the direct wound evidence for BPC-157 and TB-500.
Comparing Wound Healing Peptides#
Evidence Quality by Wound Type#
| Wound Type | BPC-157 | GHK-Cu | TB-500 | KPV | VIP |
|---|---|---|---|---|---|
| Acute Surgical | Strong preclinical | Moderate preclinical | Moderate preclinical | Limited | Theoretical |
| Chronic Dermal | Moderate preclinical | Moderate preclinical | Phase II clinical | Limited | Theoretical |
| Tendon/Ligament | Strong preclinical | Not studied | Moderate preclinical | Not applicable | Not studied |
| Burns | Moderate preclinical | Limited preclinical | Moderate preclinical | Not studied | Limited preclinical |
| GI/Mucosal | Strong preclinical | Limited | Not studied | Moderate preclinical | Moderate preclinical |
| Corneal | Moderate preclinical | Not studied | Phase III clinical | Not studied | Not studied |
Mechanism Comparison#
| Feature | BPC-157 | GHK-Cu | TB-500 | KPV | VIP |
|---|---|---|---|---|---|
| Primary target | Proliferation | Remodeling | Migration | Inflammation | Immunomodulation |
| Key pathway | VEGFR2-Akt-eNOS | Gene expression (4,000+ genes) | G-actin sequestration | NF-kB inhibition | VPAC1/VPAC2-cAMP |
| Angiogenesis | Strong (VEGF) | Moderate | Moderate (migration) | None | Mild (vasodilation) |
| Anti-inflammatory | Moderate (NO) | Moderate (TGF-beta) | Moderate (NF-kB via ILK) | Strong (NF-kB) | Strong (cytokine shift) |
| Anti-fibrotic | Not characterized | Strong (ECM remodeling) | Strong (Ac-SDKP) | Not characterized | Not characterized |
| Oral feasibility | Yes (gastric stability) | No | No | Yes (PepT1 uptake) | No |
Clinical Development Status#
| Peptide | Highest Clinical Phase | Human Safety Data | FDA Status |
|---|---|---|---|
| BPC-157 | Phase I (limited) | n < 100 total | Category 2 (banned from compounding) |
| GHK-Cu | Cosmetic use (topical) | Extensive (topical only) | Category 2 (banned from compounding) |
| TB-500 | Phase III (ophthalmic) | Phase I completed (n=70+) | Not approved |
| KPV | None | None | Not approved |
| VIP | Phase II (other indications) | Limited | Not approved |
Wound Type-Specific Considerations#
Surgical Wounds#
For clean surgical wounds where the healing cascade proceeds normally, the key therapeutic target is accelerating the proliferative phase. BPC-157's angiogenic mechanism and TB-500's cell migration effects are the most directly relevant. GHK-Cu may be valuable in the later remodeling phase to optimize collagen architecture and minimize scarring.
Chronic Non-Healing Wounds#
Chronic wounds -- diabetic ulcers, venous stasis ulcers, pressure injuries -- are fundamentally different from acute wounds because they are stalled in the inflammatory phase. The therapeutic priority shifts to resolving inflammation before proliferation can proceed. KPV and VIP, with their anti-inflammatory mechanisms, address this root cause directly. BPC-157's NO system modulation may also help normalize the dysregulated wound environment. TB-500's Phase II data in venous stasis ulcers provides the only controlled clinical evidence in this category.
Burns#
Burn wounds present unique challenges: massive tissue destruction, systemic inflammatory response, impaired vascularization of the burn bed, and high risk of pathological scarring. BPC-157's angiogenic properties and TB-500's anti-fibrotic effects are mechanistically relevant, though the burn-specific evidence for both is limited to small animal studies.
Tendon and Ligament Injuries#
BPC-157 has the strongest evidence base for musculoskeletal healing, with consistent results across multiple tendon and ligament transection models. Its activation of the FAK-paxillin pathway directly promotes tendon fibroblast migration, and its upregulation of growth hormone receptors enhances responsiveness to endogenous growth factors. TB-500's actin-mediated cell migration provides a complementary mechanism, though with less tendon-specific data.
The Combination Question#
The concept of combining healing peptides is popular in the research community, but controlled combination studies are virtually nonexistent. The most discussed combination is BPC-157 plus TB-500 (the "Wolverine Stack"), which has a theoretical rationale based on complementary mechanisms: BPC-157 provides the vascular infrastructure (angiogenesis) while TB-500 promotes cell migration into the newly vascularized wound bed.
Adding GHK-Cu could theoretically enhance the remodeling phase and reduce scarring. Including KPV or VIP in chronic wound protocols could address the inflammatory barrier that prevents other healing peptides from working effectively.
However, it must be emphasized that none of these combinations have been evaluated in controlled studies. Potential interactions -- synergistic, additive, or antagonistic -- are unknown. The NO-modulating effects of BPC-157, for example, could theoretically interact with VIP's vasodilatory properties in unpredictable ways.
Key Takeaways#
-
Evidence quality varies dramatically across wound healing peptides. TB-500 has Phase II-III clinical trial data for dermal and corneal wounds. BPC-157 has extensive but almost entirely preclinical evidence. KPV and VIP have only preclinical data, with VIP's wound-specific evidence being largely inferential.
-
Different peptides target different healing phases. There is no single "best" wound healing peptide -- the optimal choice depends on the wound type, the phase of healing that is disrupted, and the specific tissue involved.
-
The animal-to-human translation gap is the central challenge. Impressive results in rodent wound models have not consistently translated to large animal studies (as seen with TB-500's cardiac data) or human trials. This gap should temper expectations for peptides with only preclinical evidence.
-
Chronic wounds may require inflammatory resolution first. The anti-inflammatory peptides (KPV, VIP) address a fundamentally different problem than the pro-proliferative peptides (BPC-157, TB-500, GHK-Cu). In chronic wounds, proliferation fails not because it lacks stimulation but because persistent inflammation prevents it.
-
Regulatory access has narrowed. The 2024 FDA Category 2 designations for BPC-157 and GHK-Cu restrict their availability from compounding pharmacies, even as research continues. Researchers should be aware of current regulatory status in their jurisdiction.
References#
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- BPC-157 Overview and Research Guide
- BPC-157 Dosing Protocols
- BPC-157 Side Effects and Safety
- GHK-Cu Overview and Research Guide
- GHK-Cu Dosing Protocols
- GHK-Cu Side Effects and Safety
- KPV Overview and Research Guide
- KPV Dosing Protocols
- KPV Side Effects and Safety
- TB-500 Overview and Research Guide
- TB-500 Dosing Protocols
- TB-500 Side Effects and Safety
- VIP Overview and Research Guide
- VIP Dosing Protocols
- VIP Side Effects and Safety
Footnotes#
-
Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Advances in Wound Care. 2021;10(5):281-292. PMID: 33733885. ↩
-
Hsieh MJ, Liu HT, Wang CN, et al. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. J Mol Med. 2017;95(3):323-333. PMID: 28013389. ↩ ↩2
-
Seiwerth S, Brcic L, Vuletic LB, et al. BPC 157 and blood vessels. Curr Pharm Des. 2014;20(7):1014-1023. PMID: 23755723. ↩
-
Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JH. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J Appl Physiol. 2011;110(3):774-780. PMID: 21030672. ↩
-
Gastric pentadecapeptide body protection compound BPC 157 and its role in accelerating musculoskeletal soft tissue healing. World J Orthop. 2019;10(11):404-411. PMID: 30915550. ↩
-
Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. PMID: 40756949. 2025. ↩
-
ClinicalTrials.gov Identifier NCT02637284 and associated publications on BPC-157 in ulcerative colitis. ↩
-
Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. Biomed Res Int. 2015;2015:648108. PMID: 26236730. ↩ ↩2
-
Pickart L, Vasquez-Soltero JM, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of New Gene Data. Int J Mol Sci. 2018;19(7):1987. PMID: 29986520. ↩ ↩2
-
Pickart L. The human tri-peptide GHK and tissue remodeling. J Biomater Sci Polym Ed. 2008;19(8):969-988. PMID: 18644225. ↩
-
Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. J Invest Dermatol. 1999;113(3):364-368. PMID: 10469335. ↩ ↩2
-
Smart N, Risebro CA, Melville AA, et al. Thymosin beta4 induces adult epicardial progenitor mobilization and neovascularization. Nature. 2007;445(7124):177-182. PMID: 17108969. ↩
-
Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature. 2004;432(7016):466-472. PMID: 15565145. ↩
-
Treadwell T, Kleinman HK, Crockford D, Hardy MA, Guarnera GT, Goldstein AL. The regenerative peptide thymosin beta-4 accelerates the rate of dermal healing in preclinical animal models and in patients. Ann N Y Acad Sci. 2012;1270:37-44. PMID: 23050815. ↩
-
Sosne G, Dunn SP, Kim C. Thymosin beta4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial. Cornea. 2015;34(5):491-496. PMID: 25782404. ↩
-
Stark C, Taimen P, Savunen T, Koskenvuo J. Exogenous thymosin beta4 fails to promote cardiomyocyte survival and cardiac repair in a porcine model of acute myocardial infarction. Peptides. 2016;78:1-4. PMID: 26820940. ↩
-
Brzoska T, Luger TA, Maaser C, Abels C, Bohm M. Alpha-melanocyte-stimulating hormone and related tripeptides: biochemistry, antiinflammatory and protective effects in vitro and in vivo, and future perspectives for the treatment of immune-mediated inflammatory diseases. Endocr Rev. 2008;29(5):581-602. PMID: 18612058. ↩
-
Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, Yan Y, Sitaraman S, Merlin D. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology. 2008;134(1):166-178. PMID: 18061177. ↩
-
Catania A, Rajora N, Capsoni F, Minonzio F, Star RA, Lipton JM. The neuropeptide alpha-MSH has specific receptors on neutrophils and reduces chemotaxis in vitro. Peptides. 1996;17(4):675-679. PMID: 12750433. ↩
-
Laroui H, Dalmasso G, Nguyen HT, Yan Y, Sitaraman SV, Merlin D. Drug-loaded nanoparticles targeted to the colon with polysaccharide hydrogel reduce colitis in a mouse model. Gastroenterology. 2010;138(3):843-853. PMID: 18092346. ↩
-
Delgado M, Ganea D. Vasoactive intestinal peptide: a neuropeptide with pleiotropic immune functions. Amino Acids. 2013;45(1):25-39. PMID: 21847611. ↩
-
Gonzalez-Rey E, Chorny A, Delgado M. Regulation of immune tolerance by anti-inflammatory neuropeptides. Nat Rev Immunol. 2007;7(1):52-63. PMID: 17186031. ↩ ↩2

{kind=link}
Frequently Asked Questions About Peptides for Wound Healing: BPC-157, GHK-Cu, TB-500, and the Science of Tissue Repair
What does this article cover?
Evidence-based guide to wound healing peptides including BPC-157, GHK-Cu, TB-500, KPV, and VIP with mechanisms, research findings, and clinical data. This guide is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers BPC-157, GHK-Cu, KPV, TB-500, VIP. Key context: BPC-157 (Most extensively studied healing peptide with preclinical data across tendon, ligament, muscle, s...); GHK-Cu (Copper tripeptide complex with gene expression data showing modulation of 4,000+ genes involved i...); KPV (Alpha-MSH-derived anti-inflammatory tripeptide studied for reducing inflammation in wound environ...). Each peptide is discussed based on available research evidence.
Who is this guide written for?
This guide is written for researchers and individuals seeking an evidence-based overview of the topic covered in "Peptides for Wound Healing: BPC-157, GHK-Cu, TB-500, and the Science of Tissue Repair." It summarizes available research data without making treatment recommendations. Always consult a healthcare provider for medical decisions.
What are the key takeaways from this article?
The main findings covered in this article include: Most extensively studied healing peptide with preclinical data across tendon, ligament, muscle, s.... Copper tripeptide complex with gene expression data showing modulation of 4,000+ genes involved i.... Alpha-MSH-derived anti-inflammatory tripeptide studied for reducing inflammation in wound environ.... These takeaways are based on the research data available at the time of publication.
What is BPC-157 and why is it significant?
BPC-157 is a peptide discussed in this article because: Most extensively studied healing peptide with preclinical data across tendon, ligament, muscle, skin, and GI tissue repair models. For a complete profile of BPC-157, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

FDA Peptide Categories Explained: Category 1 vs Category 2 (2026)
Understand the FDA peptide classification system. Learn the difference between Category 1, Category 2, and Category 3 peptides and what the 2024-2026 regulatory changes mean for researchers.
Most Popular Therapeutic Peptides in 2026: 15 Ranked by Research Interest
The 15 most popular therapeutic peptides in 2026, ranked by clinical trial activity, search interest, and research community adoption. From semaglutide to BPC-157.

Best Healing Peptides: BPC-157, TB-500, and Beyond
A comprehensive review of the top healing peptides in research, including BPC-157, TB-500, GHK-Cu, Thymosin Alpha-1, and KPV, with evidence levels, mechanisms, and key study citations for each.
You Might Also Like
Related content you may find interesting