The Science of Peptide-Enhanced Muscle Recovery: From GH Secretagogues to BPC-157

Introduction#
Muscle recovery after exercise or injury involves a coordinated biological response spanning inflammation, satellite cell activation, protein synthesis, and tissue remodeling. This process is governed by a complex interplay of growth factors, hormones, and signaling molecules, several of which are peptides or peptide-regulated.
The growing interest in peptide-enhanced recovery has produced both legitimate research and significant overpromise. This review examines five peptides commonly discussed in the context of muscle recovery, evaluating each against the published evidence. The goal is to distinguish what research actually demonstrates from what marketing claims suggest, providing an evidence-based assessment for each compound.
For a broader ranking of muscle-related peptides, see our top 10 peptides for muscle recovery and growth. For the role of peptides in age-related muscle loss specifically, see peptides for sarcopenia.
The Biology of Muscle Recovery#
Before examining individual peptides, understanding the recovery process itself is essential.
Phase 1: Inflammation and Damage Clearance (0-48 hours)#
Intense exercise causes microtrauma to muscle fibers, initiating an inflammatory response. Neutrophils arrive first, followed by macrophages that clear damaged tissue. Pro-inflammatory cytokines (IL-6, TNF-alpha) are released, and the acute inflammatory response peaks within 24 to 48 hours. This phase is necessary for proper healing; excessive suppression of inflammation can impair recovery.
Phase 2: Satellite Cell Activation and Proliferation (24-72 hours)#
Muscle satellite cells, the resident stem cells of skeletal muscle, are activated by damage signals including hepatocyte growth factor (HGF), nitric oxide, and mechanical disruption of the basal lamina. Once activated, satellite cells proliferate to expand the repair cell pool. This phase is heavily influenced by local growth factors including IGF-1, MGF, and FGF.
Phase 3: Differentiation and Fusion (3-7 days)#
Proliferating satellite cells differentiate into myoblasts, which then fuse with existing muscle fibers to donate new nuclei (increasing the fiber's synthetic capacity) or fuse together to form new myotubes. This process requires IGF-1 signaling through the PI3K/Akt/mTOR pathway.
Phase 4: Remodeling and Hypertrophy (7-28 days)#
Newly repaired muscle undergoes remodeling, with collagen reorganization, angiogenesis (new blood vessel formation), and fiber maturation. Over time, with repeated bouts of exercise and recovery, this process leads to muscle hypertrophy through progressive increases in fiber cross-sectional area and myonuclear number.
GH Secretagogues: The Hormonal Approach#
The GH/IGF-1 Recovery Pathway#
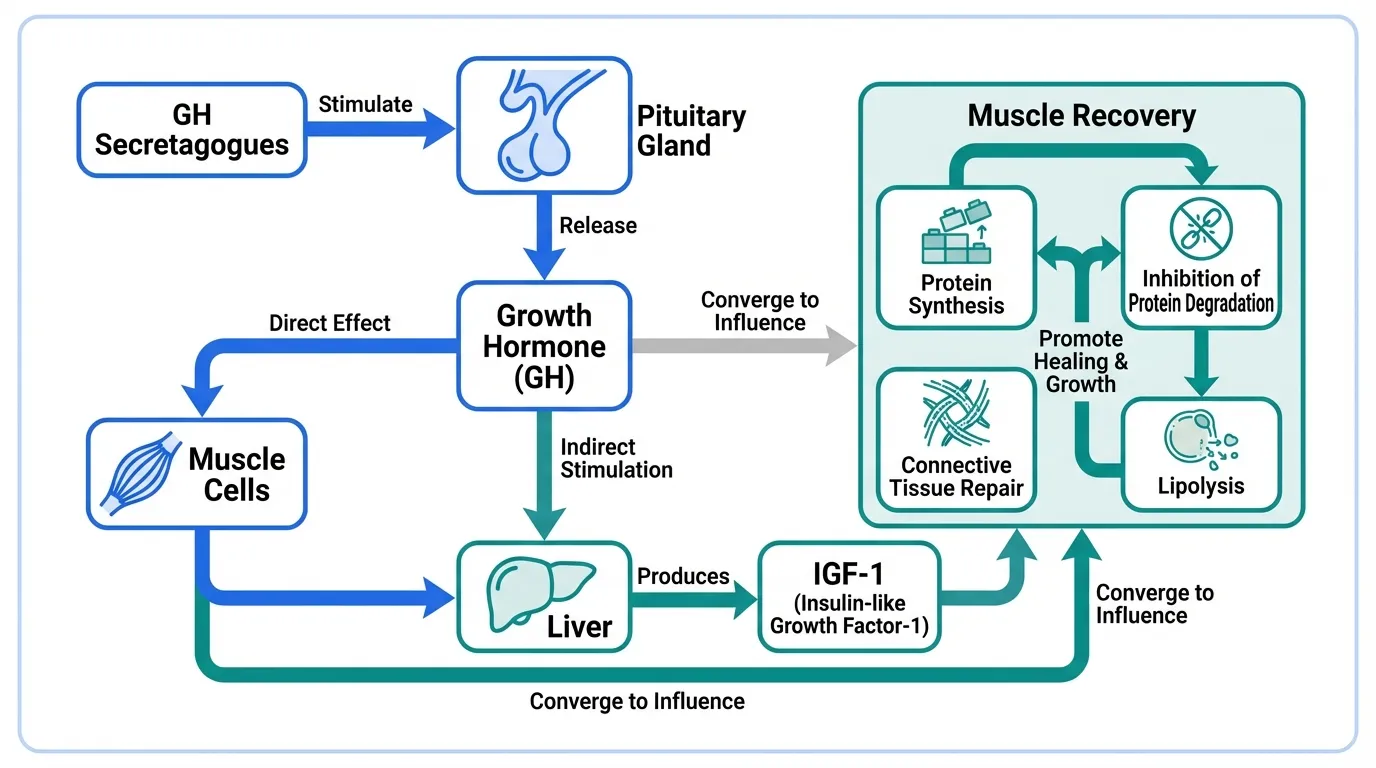
Growth hormone is a key endogenous regulator of recovery, secreted in pulsatile fashion primarily during sleep and after exercise. GH acts on muscle both directly (through GH receptors on muscle cells) and indirectly through stimulating hepatic production of IGF-1. The GH/IGF-1 axis drives protein synthesis, inhibits protein degradation, supports connective tissue repair, and promotes lipolysis to favor lean tissue accretion.
GH secretion declines with age, potentially contributing to slower recovery in older individuals. GH secretagogues aim to restore more youthful GH secretion patterns by stimulating the pituitary gland, rather than providing exogenous GH directly.
Ipamorelin: Selective Ghrelin Receptor Agonist#
Ipamorelin is a synthetic pentapeptide that stimulates GH release through the ghrelin receptor (GHS-R1a). Its distinguishing feature among GH secretagogues is selectivity: ipamorelin produces dose-dependent GH release without significantly elevating cortisol, ACTH, or prolactin at effective doses. This selectivity is notable because cortisol is catabolic to muscle, and avoiding cortisol elevation during recovery is theoretically advantageous.
Human Evidence#
Phase 1 and Phase 2 clinical trials have confirmed ipamorelin's pharmacological activity in humans. Dose-dependent GH release has been demonstrated, and the selectivity profile (GH without cortisol) has been verified in human studies. Postoperative ileus trials showed improvements in GI recovery, suggesting systemic effects of the GH release.
Evidence for Muscle Recovery#
The connection between ipamorelin and muscle recovery is indirect. No published human clinical trial has specifically evaluated ipamorelin for muscle recovery after exercise or injury. The rationale is inferential: ipamorelin stimulates GH, GH stimulates IGF-1, and IGF-1 drives muscle protein synthesis and repair. Each link in this chain is individually well-supported, but the complete pathway from ipamorelin administration to enhanced muscle recovery has not been validated in controlled human studies.
When combined with GHRH-pathway peptides like sermorelin, preclinical models have shown synergistic GH release two to three times greater than either agent alone, reflecting the complementary mechanisms (ghrelin receptor + GHRH receptor).
Honest Assessment#
Ipamorelin's pharmacological action is proven in humans. Its muscle recovery benefit is biologically plausible but not directly demonstrated. Rating: strong pharmacological evidence, indirect evidence for muscle recovery.
Sermorelin: GHRH Analog with Clinical History#
Sermorelin is a 29-amino acid peptide corresponding to the bioactive portion of human growth hormone-releasing hormone (GHRH). It was previously FDA-approved as Geref for diagnostic testing and treatment of GH deficiency in children, providing an unusual level of clinical validation for a GH secretagogue.
Human Evidence#
Sermorelin has been studied extensively in humans across multiple contexts. In aging adults, sermorelin administration has demonstrated increased GH secretion, improved body composition (increased lean mass and decreased fat mass), and enhanced sleep quality. The body composition data is particularly relevant: clinical studies have shown measurable increases in lean body mass in GH-deficient and aging populations.
Evidence for Muscle Recovery#
Like ipamorelin, sermorelin's connection to muscle recovery operates through the GH/IGF-1 axis. The body composition improvements documented in human trials (increased lean mass) suggest enhanced protein synthetic capacity, which would logically support recovery. Sermorelin preserves pulsatile GH secretion and negative feedback regulation, producing a more physiological GH profile than exogenous GH injection.
The previous FDA approval (discontinued for commercial reasons, not safety concerns) provides an unusual level of confidence in sermorelin's safety profile and pharmacological action, even though it was not specifically approved for muscle recovery.
Honest Assessment#
Sermorelin has the strongest clinical pedigree of any GH secretagogue, with previous FDA approval and documented body composition effects. The muscle recovery application is supported by GH/IGF-1 biology but not by dedicated recovery trials. Rating: strong clinical evidence for GH stimulation and body composition, indirect evidence for muscle recovery.
GH Secretagogue Limitations#
It is important to note what GH secretagogues can and cannot do for recovery:
What the evidence supports: Stimulation of endogenous GH release, maintenance of pulsatile secretion, modest improvements in body composition over months of use.
What the evidence does not support: Dramatic acute recovery enhancement, meaningful effects from single doses, or performance gains comparable to supraphysiological GH administration.
The GH/IGF-1 axis supports recovery as a background hormonal environment. Optimizing this axis through secretagogues may improve recovery capacity over time, particularly in older individuals with declining GH secretion, but expecting dramatic acute effects from GH secretagogues is not supported by the available evidence.
Tissue Repair Peptides: BPC-157 and TB-500#
BPC-157: The Most-Studied Repair Peptide#
BPC-157 (Body Protection Compound-157) is a 15-amino acid peptide derived from human gastric juice proteins. It has accumulated over 100 published preclinical studies demonstrating tissue repair effects across muscle, tendon, ligament, bone, and other tissue types.
Mechanism of Action#
BPC-157 promotes tissue repair through multiple interconnected pathways:
- Angiogenesis: Upregulation of vascular endothelial growth factor (VEGF) promotes new blood vessel formation at injury sites, improving oxygen and nutrient delivery critical for repair
- Growth factor modulation: BPC-157 upregulates receptors for multiple growth factors including EGF, FGF, and HGF, amplifying the repair signaling cascade
- FAK-paxillin pathway: Activation of focal adhesion kinase and paxillin supports cell migration to injury sites
- Nitric oxide system: Modulation of the NO system supports vascular function and has anti-inflammatory effects
- Tendon and ligament repair: BPC-157 appears to promote tenocyte migration and collagen organization, which is relevant to the connective tissue component of musculoskeletal recovery
Preclinical Evidence for Muscle Recovery#
The preclinical data on BPC-157 for musculoskeletal repair is extensive and consistent:
- Muscle: Accelerated healing of transected quadriceps muscles, crushed muscles, and denervated muscle tissue in rodent models
- Tendon: Faster Achilles tendon repair with improved biomechanical properties, enhanced tendon-to-bone healing in rotator cuff models
- Ligament: Accelerated medial collateral ligament healing in rat knee injury models
- Protective effects: Protection against muscle damage from NSAIDs and corticosteroids
The consistency across dozens of independent research groups and injury models is notable. BPC-157 has demonstrated positive results in gastric, musculoskeletal, vascular, and neurological injury models, suggesting a fundamental tissue repair mechanism rather than tissue-specific effects.
The Human Evidence Gap#
Despite the extensive preclinical data, BPC-157 has no completed randomized controlled human clinical trials published as of early 2026. A clinical trial for irritable bowel syndrome has been registered, but results have not been published. This is the most significant limitation of BPC-157 research: the translation from animal models to human outcomes is unconfirmed.
Honest Assessment#
BPC-157 has the broadest and most consistent preclinical evidence base of any tissue repair peptide. The mechanistic pathways are well-characterized and biologically plausible for muscle, tendon, and ligament recovery. However, the complete absence of published human clinical trial data means that claims about human efficacy remain unproven. Rating: extensive preclinical evidence, no human clinical confirmation.
TB-500: Cell Migration and Tissue Repair#
TB-500 is a synthetic version of thymosin beta-4, a naturally occurring 43-amino acid peptide present in virtually all nucleated cells. Thymosin beta-4 is one of the most abundant intracellular peptides, with roles in cytoskeletal regulation, cell migration, and wound healing.
Mechanism of Action#
TB-500 promotes tissue repair through distinct mechanisms:
- G-actin sequestration: Thymosin beta-4 is the primary G-actin sequestering peptide in cells, regulating the actin cytoskeleton dynamics essential for cell migration and tissue repair
- Cell migration promotion: By regulating actin dynamics, TB-500 enhances the ability of repair cells (macrophages, endothelial cells, keratinocytes) to migrate to injury sites
- Anti-inflammatory effects: Inhibition of NF-kB signaling reduces excessive inflammatory response that can impair recovery
- Angiogenesis: Promotion of new blood vessel formation supports tissue repair with improved vascular supply
- Laminin-5 upregulation: Promotes cell adhesion and extracellular matrix organization during repair
Research Evidence#
TB-500 has a broader evidence base than many preclinical peptides because thymosin beta-4 has entered human clinical trials:
- Cardiac repair: Studied in Phase 1/2 trials for cardiac repair after myocardial infarction
- Wound healing: Phase 2 trials for dermal wound healing
- Corneal healing: The RGN-259 formulation (thymosin beta-4 eye drops) completed Phase 3 clinical trials for dry eye disease and neurotrophic keratopathy, demonstrating the peptide's tissue repair properties in human tissue
- Equine studies: Improved recovery from tendon injuries in horses, which has practical relevance given the biomechanical similarity of equine tendons
Evidence for Muscle Recovery#
Muscle-specific recovery data for TB-500 comes primarily from animal models and cell culture studies. The cardiac repair trials demonstrate that thymosin beta-4 can promote tissue regeneration in human muscle (cardiac, not skeletal), providing at least partial translation to human biology. The cell migration and anti-inflammatory mechanisms are relevant to the early phases of muscle recovery.
Honest Assessment#
TB-500 benefits from thymosin beta-4's progression into multiple human clinical trials, providing human safety data and proof of tissue repair activity. However, skeletal muscle recovery specifically has not been evaluated in human trials. Rating: moderate human evidence for tissue repair, indirect evidence for skeletal muscle recovery.
MGF: The Muscle-Specific Growth Factor#
MGF (Mechano Growth Factor) occupies a unique position in the muscle recovery peptide landscape because it is the endogenous signal for exercise-induced muscle repair.
The Endogenous Role#
MGF is a splice variant of the IGF-1 gene that is expressed specifically in response to mechanical loading and muscle damage. When muscle fibers are subjected to stretch, contraction, or injury, MGF mRNA is rapidly upregulated in the damaged tissue. This local expression distinguishes MGF from circulating IGF-1: MGF acts as an autocrine/paracrine signal at the site of damage.
The primary function of MGF in recovery is satellite cell activation. MGF activates the muscle stem cell pool, stimulating satellite cells to enter the cell cycle and proliferate. Crucially, MGF promotes proliferation without immediately driving differentiation, expanding the available repair cell pool before commitment to myoblast formation. This expansion of the stem cell pool is considered a rate-limiting step in muscle repair.
The Aging Problem#
MGF expression is particularly relevant to muscle recovery research because it declines with age. Studies in human subjects have demonstrated that older adults produce significantly less MGF mRNA after resistance exercise compared to younger individuals performing the same relative workload. This blunted MGF response may contribute to the slower muscle recovery and reduced adaptive capacity observed in aged muscle.
This finding has generated interest in whether exogenous MGF administration could compensate for the age-related decline in endogenous MGF production, potentially restoring a more youthful recovery capacity.
Preclinical Evidence#
Animal studies have demonstrated that exogenous MGF peptide can activate satellite cells and enhance muscle regeneration in damage models. In rodent studies, local injection of MGF into damaged muscle increased the number of activated satellite cells and accelerated the early phases of repair.
The PEGylated form (PEG-MGF) addresses the rapid degradation of native MGF in circulation, extending the half-life from minutes to hours. However, the PEGylation may alter tissue distribution and receptor binding kinetics.
Evidence Assessment#
MGF's biological role in muscle recovery is among the best-characterized of any peptide discussed here. The endogenous expression after exercise, the satellite cell activation mechanism, and the age-related decline are all documented in human studies. However, the critical distinction is between endogenous MGF biology (well-established) and exogenous MGF peptide therapy (poorly studied in humans). No human clinical trials have evaluated exogenous MGF peptide for muscle recovery or sarcopenia. Rating: strong biological rationale, no human therapeutic evidence.
Evidence Hierarchy: Where Each Peptide Stands#
| Peptide | Human Pharma Data | Muscle Recovery Evidence | Key Strength | Key Weakness |
|---|---|---|---|---|
| Sermorelin | FDA-approved (prior) | Indirect (GH/IGF-1 axis) | Clinical safety record | Not proven for acute recovery |
| Ipamorelin | Phase 2 | Indirect (GH/IGF-1 axis) | Selective GH release | No muscle-specific trials |
| TB-500 | Phase 2/3 (non-muscle) | Indirect (tissue repair) | Human trial data exists | Skeletal muscle not studied |
| BPC-157 | None (preclinical) | Preclinical only | Extensive, consistent data | No human trials |
| MGF | None (preclinical) | Preclinical only | Endogenous biology validated | Exogenous dosing unstudied |
Distinguishing Evidence from Hype#
What the Research Supports#
- GH secretagogues (ipamorelin, sermorelin) reliably stimulate endogenous GH release in humans, with documented effects on body composition over months of use
- BPC-157 consistently accelerates tissue repair in animal models across multiple tissue types and injury models
- TB-500 (thymosin beta-4) has demonstrated tissue repair activity in human clinical trials for non-muscle indications
- MGF is a genuine endogenous repair signal expressed after exercise-induced muscle damage
- The GH/IGF-1 axis is a validated driver of muscle protein synthesis and recovery
What the Research Does Not Support#
- Claims of dramatic acute recovery enhancement from single peptide doses
- Extrapolation from animal studies to guaranteed human efficacy, particularly for BPC-157
- Equivalence between endogenous peptide biology and exogenous peptide therapy, particularly for MGF
- Stacking multiple peptides for "synergistic recovery" without evidence that combinations are superior to individual agents
- Performance enhancement beyond normal physiological recovery capacity
The Translation Problem#
The gap between preclinical promise and clinical reality is significant across all drug development, and peptides are no exception. Historically, fewer than 10 percent of drugs that show efficacy in animal models succeed in human clinical trials. The peptides discussed here span a wide range of this translation, from sermorelin (fully translated to human use) to BPC-157 (entirely preclinical).
When evaluating claims about these peptides, the evidence hierarchy matters: FDA-approved > Phase 2/3 human data > Phase 1 human data > animal models > cell culture. A compound with consistent animal data is scientifically interesting, but claiming human efficacy from animal data alone is a category error that is common in the peptide space.
Conclusion#
The five peptides reviewed here represent three distinct approaches to muscle recovery: hormonal optimization (ipamorelin, sermorelin), tissue repair acceleration (BPC-157, TB-500), and satellite cell activation (MGF). Each has genuine scientific basis and published research supporting its mechanism, but the evidence levels vary dramatically.
Sermorelin and ipamorelin have the strongest human evidence, with confirmed pharmacological activity and, in sermorelin's case, previous FDA approval. Their connection to muscle recovery operates through the well-established GH/IGF-1 axis, making the rationale solid even though dedicated recovery trials are lacking.
BPC-157 has the most extensive preclinical evidence of any repair peptide, but the complete absence of human clinical trial data remains its most significant limitation. TB-500 benefits from thymosin beta-4's entry into human trials for other indications, providing some human safety and efficacy data.
MGF has the most compelling biological story as the endogenous exercise-induced repair signal, but exogenous MGF peptide therapy in humans is unstudied.
For anyone evaluating these compounds, the critical question is always: what has been demonstrated in humans versus what is extrapolated from preclinical models? Maintaining this distinction is essential for evidence-based decision-making in a field where marketing often outpaces the science.
Related Peptide Profiles#
Learn more about the peptides discussed in this article:
- BPC-157 Overview and Research Guide
- BPC-157 Dosing Protocols
- BPC-157 Side Effects and Safety
- Ipamorelin Overview and Research Guide
- Ipamorelin Dosing Protocols
- Ipamorelin Side Effects and Safety
- MGF Overview and Research Guide
- MGF Dosing Protocols
- MGF Side Effects and Safety
- Sermorelin Overview and Research Guide
- Sermorelin Dosing Protocols
- Sermorelin Side Effects and Safety
- TB-500 Overview and Research Guide
- TB-500 Dosing Protocols
- TB-500 Side Effects and Safety

{kind=link}
Frequently Asked Questions About The Science of Peptide-Enhanced Muscle Recovery: From GH Secretagogues to BPC-157
What does this article cover?
Research review of peptides for muscle recovery including BPC-157, TB-500, ipamorelin, sermorelin, and MGF with mechanisms, evidence levels, and clinical data analysis. This research review is for educational purposes only and does not constitute medical advice.
Which peptides are discussed in this article?
This article covers BPC-157, Ipamorelin, MGF, Sermorelin, TB-500. Key context: BPC-157 (Gastric pentadecapeptide with extensive preclinical evidence for tendon, ligament, and muscle rep...); Ipamorelin (Selective GH secretagogue that stimulates endogenous growth hormone release without cortisol elev...); MGF (Mechano Growth Factor splice variant of IGF-1 expressed locally in muscle after mechanical loadin...). Each peptide is discussed based on available research evidence.
What level of evidence does this research review cover?
This research review examines published preclinical and clinical studies related to the peptides discussed. Evidence quality varies between peptides and indications. The article distinguishes between FDA-approved uses and investigational applications where applicable.
What are the key takeaways from this article?
The main findings covered in this article include: Gastric pentadecapeptide with extensive preclinical evidence for tendon, ligament, and muscle rep.... Selective GH secretagogue that stimulates endogenous growth hormone release without cortisol elev.... Mechano Growth Factor splice variant of IGF-1 expressed locally in muscle after mechanical loadin.... These takeaways are based on the research data available at the time of publication.
What is BPC-157 and why is it significant?
BPC-157 is a peptide discussed in this article because: Gastric pentadecapeptide with extensive preclinical evidence for tendon, ligament, and muscle repair through angiogenesis and growth factor modulation. For a complete profile of BPC-157, see the dedicated peptide page on this site.
Continue reading this research review
Free access to the complete analysis with citations and evidence ratings.
150+ peptide profiles · 30+ comparisons · 18 research tools
Medical Disclaimer
This website is for educational and informational purposes only. The information provided is not intended to diagnose, treat, cure, or prevent any disease. Always consult with a qualified healthcare professional before using any peptide or supplement.
Join 2,000+ researchers getting biweekly updates
Enjoyed this article?
The Research Briefing delivers deep-dives like this biweekly — plus new study breakdowns, safety updates, and tool announcements.
Free forever. No spam. Unsubscribe in one click.
Where to Find These Peptides
Continue Exploring
Peptide Profiles
Keep Reading

Peptides for Athletic Recovery: Beyond BPC-157 and TB-500
A comprehensive guide to peptides researched for athletic recovery, covering BPC-157, TB-500, GH secretagogues, MGF, GHK-Cu, and DSIP. Includes WADA anti-doping considerations, evidence levels, and recovery-focused protocol rationale.

Top 10 Peptides for Muscle Recovery and Growth: Evidence-Based Research Guide
The 10 most studied peptides for muscle recovery and growth, including BPC-157, TB-500, IGF-1 LR3, ipamorelin, and follistatin, with mechanisms, evidence levels, and key research data.
Understanding Peptide Side Effects: A Comprehensive Safety Guide
A thorough, evidence-based guide to peptide side effects by category — covering GLP-1 agonists, GH secretagogues, tissue repair peptides, and melanocortins — with serious risk flags, drug interactions, monitoring recommendations, and guidance on when to stop.
You Might Also Like
Related content you may find interesting